

Abstract
Transverse aortic constriction (TAC) in mice has been used as a valuable model to study mechanisms of cardiac hypertrophy and heart failure1. A reliable noninvasive method is essential to assess real-time cardiac morphological and functional changes in animal models of heart disease. Transthoracic echocardiography represents an important tool for noninvasive assessment of cardiac structure and function2. Here we used a high-resolution ultrasound imaging system to monitor myocardial remodeling and heart failure progression over time in a mouse model of TAC. B-mode, M-mode, and Doppler imaging were used to precisely assess cardiac hypertrophy, ventricular dilatation, and functional deterioration in mice following TAC. Color and pulse wave (PW) Doppler imaging was used to noninvasively measure pressure gradient across the aortic constriction created by TAC and to assess transmitral blood flow in mice. Thus transthoracic echocardiographic imaging provides comprehensive noninvasive measurements of cardiac dimensions and function in mouse models of heart disease.
Keywords: Medicine, Issue 112, trans-thoracic echocardiography, Doppler imaging, transverse aortic constriction, mouse model of heart disease, cardiac hypertrophy, heart failure
Introduction
Mouse models of heart disease, such as TAC and myocardial infarction (MI), have been proven to be valuable to study disease mechanisms as well as to develop novel therapeutic strategies3. TAC initially induces compensatory hypertrophy, but prolonged pressure overload leads to cardiac dilatation and heart failure4. The tightness of the aortic constriction directly determines the degree of cardiac hypertrophy and its transition to heart failure. Noninvasive and reliable measurement of pressure gradient across the aortic constriction is essential for the success of these studies. Doppler imaging has been used to assess pressure gradient produced by TAC5, which is a noninvasive alternative for catheter-based pressure measurement.
Echocardiography has been widely used to noninvasively measure cardiac morphology as well as systolic and diastolic function in mice6-8. Two-dimensional B-mode imaging is used to detect abnormal movements or structural changes of the heart. One-dimensional M-mode imaging is used for quantification of cardiac dimensions and contractility. Color and PW Doppler imaging has recently been used on rodent ultrasound, which has broad applications for echocardiography, including measurement of flow directionality and velocity, as well as systolic and diastolic performance9.
Longitudinal real-time monitoring of cardiac function using echocardiography in B-mode, M-mode, color and PW Doppler mode provides comprehensive assessment of cardiac structure and function in mice under physiological and pathological conditions. Here we provide a detailed description of the use of echocardiographic imaging to monitor dynamic cardiac morphological and functional changes in mice following TAC or sham surgery.
Protocol
The protocol follows the guidelines of the Institutional Animal Care and Use Committee of University of Washington.
1. Surgical Procedure and Preparation for Imaging
Subject C57BL/6 mice to TAC or sham surgery as previously described10.
One week after TAC or sham surgery, anesthetize the mouse in the induction chamber with 2% isoflurane mixed with 1 L/min O2. Confirm proper anesthetization by unresponsiveness to toe or tail pinching. Use veterinary ointment on eyes to prevent dryness while under anesthesia. Remove the chest hair by applying hair removal cream. Disinfect mouse skin with 70% ethanol.
Secure the mouse to an animal-handling platform in the supine position. To maintain a steady level of anesthesia, use a nosecone to deliver 0.5 - 1% isoflurane mixed with 1 L/min O2.
Apply electrode gel to the paws of the mouse and tape them to the electrode pad.
Insert a rectal probe to monitor body temperature. Maintain the body temperature at 37 °C via a heating pad or lamp.
Apply a layer of pre-warmed ultrasound gel to the mouse chest, mainly the area overlying the heart. Note: remove ultrasound gel and dry the mouse with sterile gauze after the imaging procedure.
2. In the Aortic Arch View, Use B-mode and Doppler Imaging to Evaluate Transverse Aortic Constriction
- Use the B-mode setting to obtain the aortic arch view in order to visualize the aorta, major arterial branches, and the constriction site.
- Tilt the left side of the platform up as far as possible to rotate the mouse into left decubitus position. Hold the ultrasound transducer by stand in vertical position and place it on the chest along the right parasternal line, with the notch pointing towards the chin of the mouse. Note: Do not compress the mouse thorax when lowering the transducer; minimal amount of pressure is required.
- Tilt the transducer up at the level of scapula and rotate slightly clockwise until aortic arch comes into view. Observe the transverse aortic constriction site, which is located between the branching of innominate artery (IA) and left common carotid artery (LCCA) (Figure 1). Note: No constriction is detected in sham-operated mouse.
Click the "color Doppler" button on the workstation to switch to color Doppler mode to monitor directionality and velocity of the blood flow across the constriction site. Acquire and store images by clicking the "cine store" button.
Click the "PW Doppler" button to switch to pulse wave Doppler mode, and place sample volume (the dashed cursor box) immediately distal to the constriction site to search for the stenotic jet with the highest velocity, then click the "PW Doppler" button to obtain waveforms of aortic flow and measure peak velocity (Figure 2).
Calculate pressure gradient across the constriction site using the modified Bernoulli's equation: pressure gradient = 4 x Vmax2. Only include mice with a pressure gradient ranging from 40 to 80 mmHg for further analysis.
3. In the Parasternal Long Axis View, Use B-mode and M-mode Imaging to Assess Cardiac Dimensions and Contractility
With the mouse lying in the supine position on the platform, hold the transducer in vertical fashion with the notch pointing to the mouse's head. Lower the transducer on the thorax parallel to the left parasternal line and rotate 30° counter-clockwise.
Use B-mode imaging to obtain a full long axis "sagittal" view of the heart. Adjust the angle of the transducer and focus depth to visualize left ventricle, the intraventricular septal wall, and a slight portion of the right ventricular wall. Save the images for later measurements of cardiac wall thickness and chamber dimension. Using "cardiac package", select parameters such as IVS or LVAW, LVID, and LVPW, and then click on the image to draw corresponding lines for each parameter to obtain the measurements.
Observe cardiac wall movement patterns and check for possible motion abnormalities, including akinesia, hypokinesia, and asynchrony. Note: Akinesia and hypokinesia denote complete and partial loss of movement of the cardiac wall, respectively. Asynchrony denotes irregular, uncoordinated cardiac wall movement.
Switch to M-mode, place M-mode cursor perpendicular to the LV walls at the level of the papillary muscle, and acquire images for later measurement of cardiac dimensions and fractional shortening (Figure 3).
4. In the Parasternal Short Axis View, Use B-mode and M-mode Imaging to Assess Cardiac Morphology and Function
From the parasternal long axis view, obtain parasternal short axis view by rotating the transducer 90° clockwise. Adjust the transducer to give a horizontal cross-sectional "transverse" view of the heart in B-mode, with both papillary muscles clearly visible and located to the right (the 2 and 4 o'clock position).
Switch to M-mode and place the M-mode axis at the mid-level of the left ventricle. Acquire and store images for later measurements of cardiac wall thickness, chamber dimension, and fractional shortening (Figure 4). Using "cardiac package", select parameters in SAX (short axis) including IVS or LVAW, LVID, and LVPW, and click on the image to draw corresponding lines for each parameter to obtain the measurements. Note: Measurements obtained here should correlate closely to those obtained in the parasternal long axis view (Figure 5).
5. In the Apical Four-chamber View, Use Doppler Imaging to Assess Systolic and Diastolic Function
Obtain the apical four-chamber view to visualize both left and right ventricles with the atria at the bottom of the screen. In B-mode, from the short axis view, tilt the upper left corner of the platform to angle the mouse's head down and orient the transducer towards the right shoulder of the mouse. This is essentially to achieve a "coronal" view of the heart looking up towards the apex.
Visualize the mitral valve in B-mode, and switch to color Doppler mode, placing the sample volume (the dashed cursor box) at the tip of the mitral valve.
Switch to PW Doppler mode to assess flow patterns across the mitral valve. Align the Doppler probe cursor parallel to the direction of mitral blood flow. Use a probe angle less than 20° to determine peak velocity (Figure 6).
Save the images for later measurements. Use "cardiac package" and select "MV flow". Click each parameter and draw corresponding lines to obtain the measurements. Available measurements include: peak E velocity (early filling with active ventricular relaxation), peak A velocity (late filling with atrial contraction), mitral isovolumic relaxation and contraction times (IVRT and IVCT respectively), and ejection time (ET).
Calculate myocardial performance index (MPI) by MPI = (IVCT + IVRT)/ET.
6. Post-procedural Treatment of Animal
Give analgesia and/or sterile saline intraperitoneally to surgical animals when necessary.
Allow the animal to recover on a heating pad in the prone position. Do not leave an animal unattended until it has regained sufficient consciousness to maintain sternal recumbency. Do not return an animal that has undergone the procedure to the company of other animals until fully recovered.
Representative Results
Figure 1 shows B-mode images of the aortic arch view of mouse heart subjected to sham (Figure 1A) or TAC surgery (Figure 1B). The aortic arch, innominate artery, left common carotid artery, and left subclavian artery are shown. Note that aortic constriction is clearly visible in TAC but not sham heart. Color Doppler images from aortic view are shown in Figure 2A. The waveforms of aortic flow across the constriction site were captured by PW Doppler imaging (Figure 2B). Successful TAC will lead to a significantly increased flow velocity downstream the constriction site (typically ~4 m/sec in TAC mice). Pressure gradient across the constriction was calculated based on peak flow velocity, according to the modified Bernoulli's equation (Figure 2C).
Figure 3 shows B- and M-mode images of the parasternal long axis view of sham (Figure 3A) or TAC heart (Figure 3B). The upper panel shows the B-mode images of the left ventricle, the interventricular septum, and a portion of the right ventricle from sham or TAC mice. The lower panel shows the M-mode tracings of several cardiac cycles from sham or TAC mice. The measurements of cardiac dimensions are shown, including the left ventricular anterior wall thickness (LVAW), left ventricular internal diameter (LVID), left ventricular posterior wall thickness (LVPW) in diastole and systole. Note significantly increased wall thickness in mouse heart subjected to TAC compared with sham surgery.
Figure 4 shows images of the parasternal short axis view of sham (Figure 4A) or TAC heart (Figure 4B). The upper portion of each panel shows the M-mode axis (the dotted line) placed in the center of the left ventricle. The lower portion of each panel is the M-mode tracing with lines indicating cardiac dimensions as described above. As a marker of hypertrophy, ventricular and septal wall thickness can be accurately determined. Mice subjected to TAC showed increased wall thickness as assessed by LVAWd and LVPWd, ventricular dilatation as assessed by LVISd and LVISs, decreased contractility as assessed by LVFS and LVEF, and increased LV mass (Figure 5).
Figure 6 shows B-mode apical four-chamber view (Figure 6A,B) and PW Doppler images of transmitral flow patterns (Figure 6C,D). Measurements of peak E and A velocity, IVCT, IVRT, and ET are shown. The E/A ratio and MPI are calculated (Figure 6E - I). A healthy mouse heart has an E/A ratio ≥1 and a MPI value ≤0.5. In pathological conditions with diastolic or systolic cardiac dysfunction, such as in mice subjected to TAC, a decreased E/A ratio and/or an increased MPI value are typically observed.
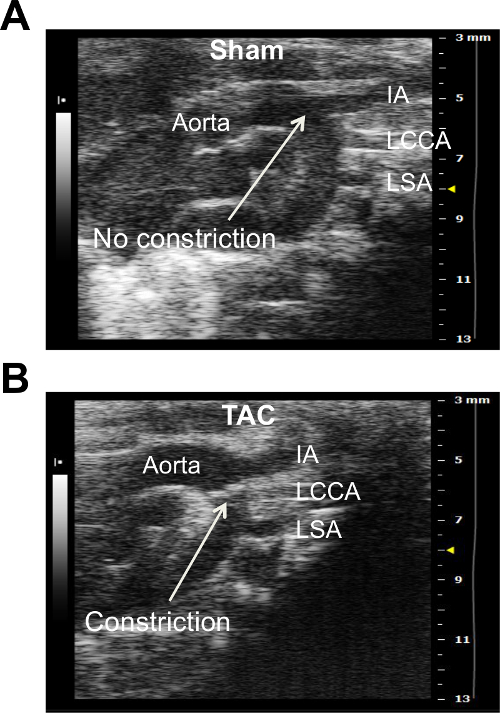 Figure 1. B-mode Image of the Aortic Arch View of Mouse Heart Subjected to Sham Surgery (A) or TAC (B). Major aortic branches including innominate artery (IA), left common carotid artery (LCCA), and left subclavian artery (LSA) are shown. Note that transverse aortic constriction (indicated by the white arrow) can be visualized in TAC but not sham heart. Please click here to view a larger version of this figure.
Figure 1. B-mode Image of the Aortic Arch View of Mouse Heart Subjected to Sham Surgery (A) or TAC (B). Major aortic branches including innominate artery (IA), left common carotid artery (LCCA), and left subclavian artery (LSA) are shown. Note that transverse aortic constriction (indicated by the white arrow) can be visualized in TAC but not sham heart. Please click here to view a larger version of this figure.
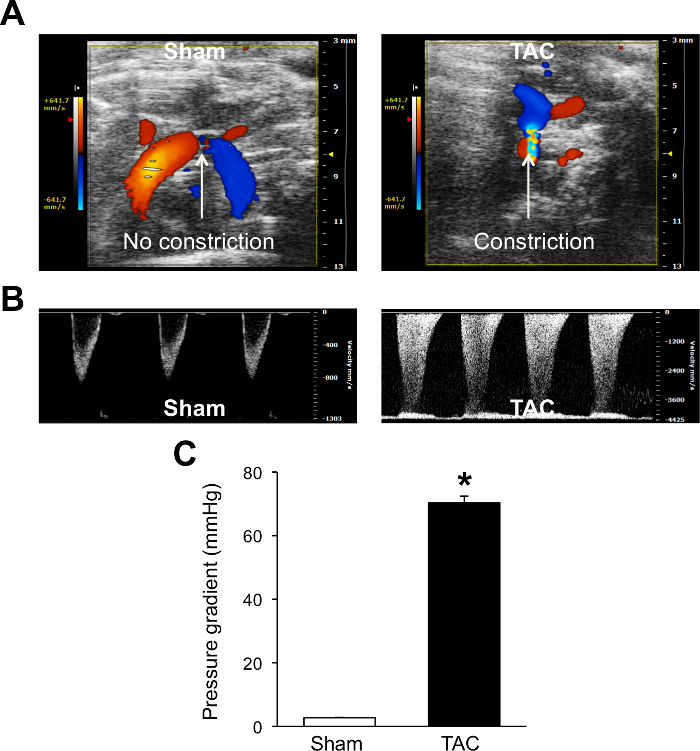 Figure 2. Color/PW Doppler Imaging of the Transverse Aorta Blood Fow from the Aortic Arch View. Color (A) and PW (B) Doppler images from sham and TAC hearts are shown. Peak aortic velocity obtained from PW Doppler imaging is used to calculate pressure gradient according to the modified Bernoulli equation (C). These data confirm a successful TAC surgery with the pressure gradient of ~70 mmHg. *P <0.05 vs. Sham. Data are expressed as mean ± s.e.m. n = 15 for Sham and n = 13 for TAC. Student's t-test was used to determine statistical significance. Please click here to view a larger version of this figure.
Figure 2. Color/PW Doppler Imaging of the Transverse Aorta Blood Fow from the Aortic Arch View. Color (A) and PW (B) Doppler images from sham and TAC hearts are shown. Peak aortic velocity obtained from PW Doppler imaging is used to calculate pressure gradient according to the modified Bernoulli equation (C). These data confirm a successful TAC surgery with the pressure gradient of ~70 mmHg. *P <0.05 vs. Sham. Data are expressed as mean ± s.e.m. n = 15 for Sham and n = 13 for TAC. Student's t-test was used to determine statistical significance. Please click here to view a larger version of this figure.
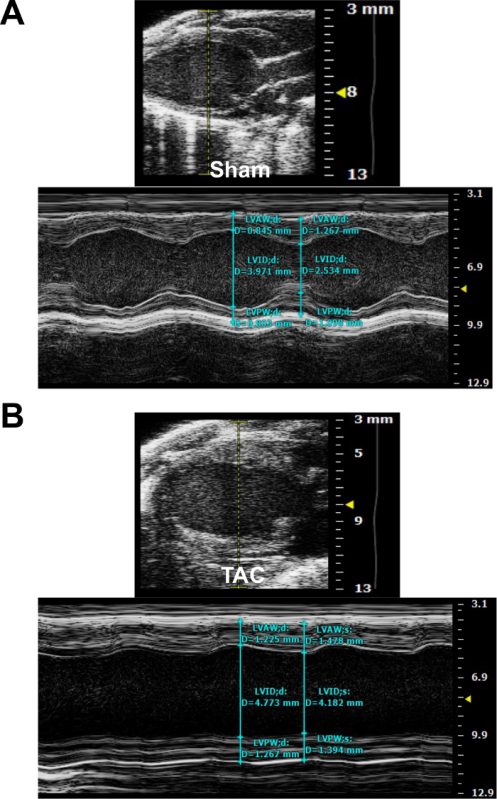 Figure 3. Parasternal Long Axis (PLAX) View of Mouse Heart Subjected to Sham Surgery (A) or TAC (B). M-mode images indicate the placement of the sample volume (dotted yellow line in the upper panel) and measurement of cardiac dimensions in diastole and systole (blue lines in the lower panel). Please click here to view a larger version of this figure.
Figure 3. Parasternal Long Axis (PLAX) View of Mouse Heart Subjected to Sham Surgery (A) or TAC (B). M-mode images indicate the placement of the sample volume (dotted yellow line in the upper panel) and measurement of cardiac dimensions in diastole and systole (blue lines in the lower panel). Please click here to view a larger version of this figure.
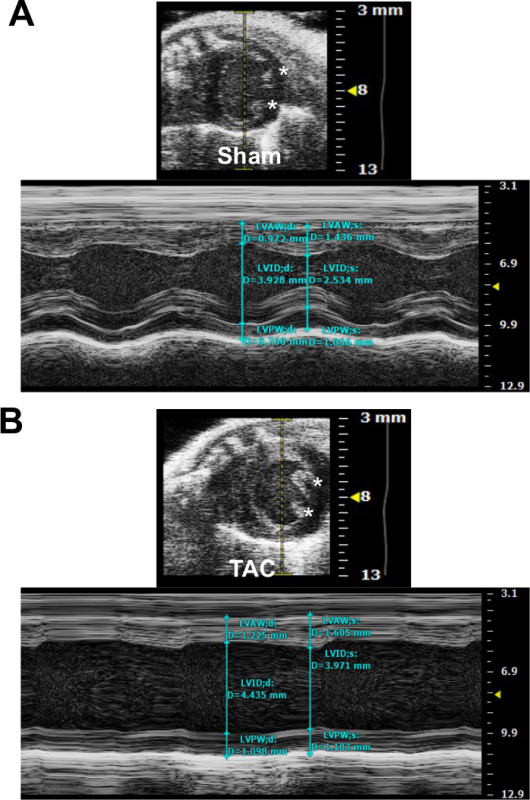 Figure 4. Parasternal Short Axis (PSAX) View of Mouse Heart Subjected to Sham Surgery (A) or TAC (B). M-mode images indicate the placement of the sample volume (dotted yellow line in the upper panel) and measurement of cardiac dimensions in diastole and systole (blue lines in the lower panel). The asterisks indicate papillary muscles. Please click here to view a larger version of this figure.
Figure 4. Parasternal Short Axis (PSAX) View of Mouse Heart Subjected to Sham Surgery (A) or TAC (B). M-mode images indicate the placement of the sample volume (dotted yellow line in the upper panel) and measurement of cardiac dimensions in diastole and systole (blue lines in the lower panel). The asterisks indicate papillary muscles. Please click here to view a larger version of this figure.
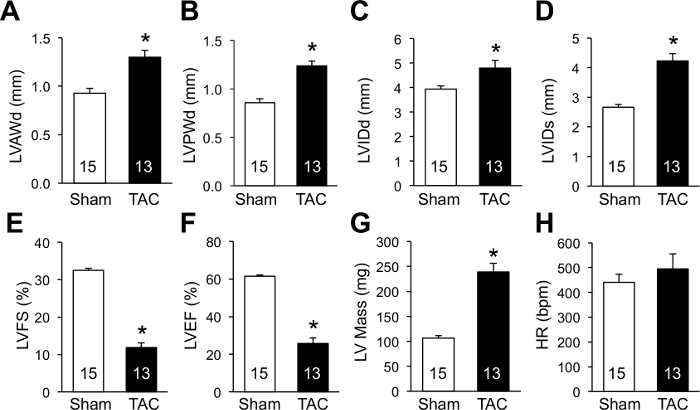 Figure 5. Echocardiographic Assessment of Cardiac Morphological and Functional Changes Following TAC. M-mode imaging in short axis view was performed as in Figure 4. (A) LVAWd, left ventricular anterior wall thickness in diastole. (B) LVPWd, left ventricular posterior wall thickness in diastole. (C) LVIDd, left ventricular internal diameter in diastole. (D) LVIDs, left ventricular internal diameter in systole. (E) LVFS, left ventricular fractional shortening. LVFS (%) = (LVIDd-LVIDs)/LVIDd x100%. (F) LVEF, left ventricular ejection fraction. LVEF (%) = (LVEDV-LVESV)/LVEDV x100%. LVEDV and LVESV denote left ventricular end-diastolic and end-systolic volume, respectively. LV volume and ejection fraction are precisely assessed by Simpson's method. LV volume is estimated by fitting numerous disks into the ventricle: Simpson volume = [area(1) + area(2) + … + area(n)] x length. Simpson area and length are obtained by tracing the endocardial border of the LV in the long axis and short axis view. (G) LV (left ventricular) mass. LV mass (mg) = 1.05 x [(LVIDd + LVPWd + IVSd)3 - (LVIDd)3]. The factor 1.05 represents the specific density of the myocardium. (H) HR, heart rate. *P <0.05 vs. Sham. The number of mice analyzed is shown in the bars of each panel. Data are expressed as mean ± s.e.m. Student's t-test was used to determine statistical significance. Please click here to view a larger version of this figure.
Figure 5. Echocardiographic Assessment of Cardiac Morphological and Functional Changes Following TAC. M-mode imaging in short axis view was performed as in Figure 4. (A) LVAWd, left ventricular anterior wall thickness in diastole. (B) LVPWd, left ventricular posterior wall thickness in diastole. (C) LVIDd, left ventricular internal diameter in diastole. (D) LVIDs, left ventricular internal diameter in systole. (E) LVFS, left ventricular fractional shortening. LVFS (%) = (LVIDd-LVIDs)/LVIDd x100%. (F) LVEF, left ventricular ejection fraction. LVEF (%) = (LVEDV-LVESV)/LVEDV x100%. LVEDV and LVESV denote left ventricular end-diastolic and end-systolic volume, respectively. LV volume and ejection fraction are precisely assessed by Simpson's method. LV volume is estimated by fitting numerous disks into the ventricle: Simpson volume = [area(1) + area(2) + … + area(n)] x length. Simpson area and length are obtained by tracing the endocardial border of the LV in the long axis and short axis view. (G) LV (left ventricular) mass. LV mass (mg) = 1.05 x [(LVIDd + LVPWd + IVSd)3 - (LVIDd)3]. The factor 1.05 represents the specific density of the myocardium. (H) HR, heart rate. *P <0.05 vs. Sham. The number of mice analyzed is shown in the bars of each panel. Data are expressed as mean ± s.e.m. Student's t-test was used to determine statistical significance. Please click here to view a larger version of this figure.
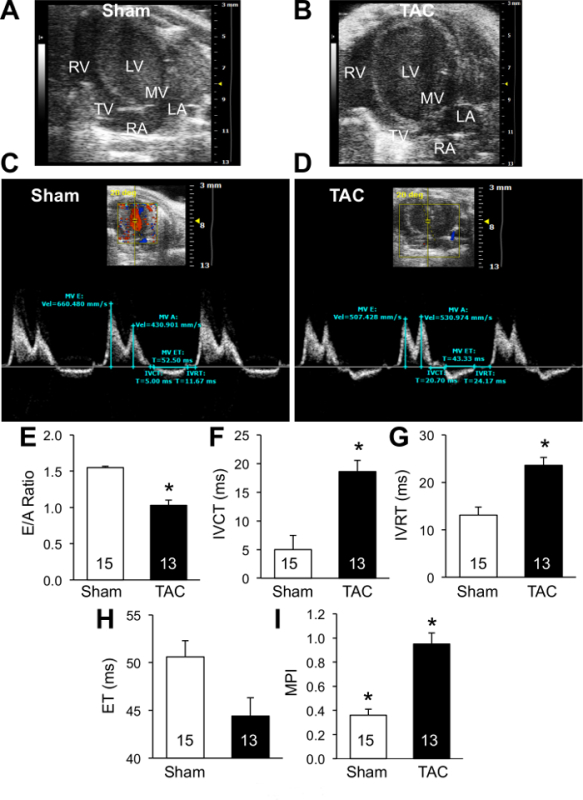 Figure 6. Assessment of Transmitral Blood Flow by Doppler Imaging. (A and B) B-mode apical four-chamber view of sham (A) or TAC (B) heart. LV, left ventricle; RV, right ventricle; MV, mitral valve; TV, tricuspid valve; LA, left atrium; RA, right atrium. (C and D) PW Doppler waveform of trans-mitral blood flow in sham (C) or TAC (D) heart. Relevant measurements are shown. (E) E/A, peak E and A velocity ratio. (F) IVCT, isovolumic contraction time. (G) IVRT, isovolumic relaxation time. (H) ET, ejection time. (I) MPI, myocardial performance index. *P <0.05 vs. Sham. The number of mice analyzed is shown in the bars of each panel. Data are expressed as mean ± s.e.m. Student's t-test was used to determine statistical significance. Please click here to view a larger version of this figure.
Figure 6. Assessment of Transmitral Blood Flow by Doppler Imaging. (A and B) B-mode apical four-chamber view of sham (A) or TAC (B) heart. LV, left ventricle; RV, right ventricle; MV, mitral valve; TV, tricuspid valve; LA, left atrium; RA, right atrium. (C and D) PW Doppler waveform of trans-mitral blood flow in sham (C) or TAC (D) heart. Relevant measurements are shown. (E) E/A, peak E and A velocity ratio. (F) IVCT, isovolumic contraction time. (G) IVRT, isovolumic relaxation time. (H) ET, ejection time. (I) MPI, myocardial performance index. *P <0.05 vs. Sham. The number of mice analyzed is shown in the bars of each panel. Data are expressed as mean ± s.e.m. Student's t-test was used to determine statistical significance. Please click here to view a larger version of this figure.
Discussion
Echocardiography has been widely used to assess cardiac function in rodent models of heart disease2,6. Compared to invasive or terminal methodologies such as pressure-volume loop measurement11 and ex vivo working heart12, echocardiography provides a powerful, noninvasive tool to assess ongoing cardiac structural and functional changes in living animals. To obtain reliable data, it is important to maintain body temperature and heart rate within physiological range13 by careful adjusting the heating apparatus and the anesthesia level. All images should be captured and analyzed consistently according to the standardized imaging procedures, to facilitate the comparison between mice of different strain or genotype.
TAC is commonly used to induce cardiac hypertrophy and heart failure in mice1. Noninvasive measurement of pressure gradient across the constriction site by Doppler imaging represents a reliable assessment of the degree of pressure overload in mice. Successful TAC typically produces a pressure gradient ≥40 mmHg. Only mice subjected to similar degree of pressure overload should be included for further analysis, while mice with a pressure gradient too low or too high should be excluded. Following TAC, mice are expected to develop cardiac hypertrophy within 1-2 weeks, and cardiac dilatation after 4 weeks, depending the degree of pressure overload and the genetic background of mice tested. The dynamic cardiac remodeling and functional changes following TAC can be reliably assessed by echocardiographic imaging as described above.
In contrast to its frequent usage in humans14, color/PW Doppler has only been recently available in rodent ultrasound imaging9. Here also we described the applications of Doppler imaging in measuring pressure gradient as well as systolic and diastolic performance. Measurement of mitral and tricuspid blood flow directionality and velocity (i.e., E/A ratio, IVRT, IVCT, ET, and MPI) provides important information on cardiac function. Thus echocardiographic imaging represents an important tool to study cardiac physiology and pathophysiology in small animals.
The limitation of cardiac ultrasound imaging is related to measurement variability and reproducibility. To reduce inter- and intra- operator variability, it is important to standardize how images are acquired and analyzed. Measurements should be performed from multiple acoustic windows and modes (B-mode, M-mode, and PW/color Doppler) and at least 3 separate measurements should be averaged to ensure accuracy and reliability. In addition, there are limited acoustic windows and sometimes low quality images are obtained in small rodents subjected to surgical procedures such as TAC, due to tissue swelling, surgical scars, and lung edema that interfere with the ultrasound beams. For Doppler imaging, sometimes it is challenging to separate E and A waves and obtain a complete waveform of the mitral flow, due to a relatively high heart rate in small rodents, especially in mice subjected to TAC or MI surgery. Lowering the heart rate may be helpful to get measurements, but this will affect values obtained by Doppler imaging and hence the data interpretation.
With recent technical advances, newly released ultrasound systems provide high image resolution and frame/sampling rates to ensure accurate quantitative measurement in small animals. New echocardiography technologies will also improve the sensitivity of echocardiographic evaluation of cardiac function and permit early detection of cardiac pathology. For example, speckle-tracking strain imaging15 has been used to precisely measure regional myocardial function. New transducer technologies currently under development will provide the potential for real-time, 3D or 4D imaging. Contrast echocardiography that is in advanced development will allow for volumetric measurements, tissue perfusion assessments, molecular imaging of cardiovascular disease, and delivery of therapeutic agents.
Disclosures
This work was supported in part by NIH/NHLBI grants R00HL0908076 and R01HL116507 (to Q.L.).
Acknowledgments
The authors have nothing to disclose.
References
- Rockman HA, et al. Segregation of atrial-specific and inducible expression of an atrial natriuretic factor transgene in an in vivo murine model of cardiac hypertrophy. Proc Natl Acad Sci USA. 1991;88(18):8277–8281. doi: 10.1073/pnas.88.18.8277. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tanaka N, et al. Transthoracic echocardiography in models of cardiac disease in the mouse. Circulation. 1996;94(5):1109–1117. doi: 10.1161/01.cir.94.5.1109. [DOI] [PubMed] [Google Scholar]
- Patten RD, Hall-Porter MR. Small animal models of heart failure: development of novel therapies, past and present. Circ Heart Fail. 2009;2(2):138–144. doi: 10.1161/CIRCHEARTFAILURE.108.839761. [DOI] [PubMed] [Google Scholar]
- Heineke J, Molkentin JD. Regulation of cardiac hypertrophy by intracellular signalling pathways. Nat Rev Mol Cell Biol. 2006;7(8):589–600. doi: 10.1038/nrm1983. [DOI] [PubMed] [Google Scholar]
- Oka T, et al. Cardiac-specific deletion of Gata4 reveals its requirement for hypertrophy, compensation, and myocyte viability. Circ Res. 2006;98(6):837–845. doi: 10.1161/01.RES.0000215985.18538.c4. [DOI] [PubMed] [Google Scholar]
- Gardin JM, Siri FM, Kitsis RN, Edwards JG, Leinwand LA. Echocardiographic assessment of left ventricular mass and systolic function in mice. Circ Res. 1995;76(5):907–914. doi: 10.1161/01.res.76.5.907. [DOI] [PubMed] [Google Scholar]
- Respress JL, Wehrens XH. Transthoracic echocardiography in mice. J Vis Exp. 2010. p. e1738. [DOI] [PMC free article] [PubMed]
- Pistner A, Belmonte S, Coulthard T, Blaxall B. Murine echocardiography and ultrasound imaging. J Vis Exp. 2010. p. e2100. [DOI] [PMC free article] [PubMed]
- Patten RD, Aronovitz MJ, Bridgman P, Pandian NG. Use of pulse wave and color flow Doppler echocardiography in mouse models of human disease. J Am Soc Echocardiogr. 2002;15(7):708–714. doi: 10.1067/mje.2002.118912. [DOI] [PubMed] [Google Scholar]
- deAlmeida AC, van Oort RJ, Wehrens XH. Transverse aortic constriction in mice. J Vis Exp. 2010. p. e1729. [DOI] [PMC free article] [PubMed]
- Pacher P, Nagayama T, Mukhopadhyay P, Bátkai S, Kass DA. Measurement of cardiac function using pressure-volume conductance catheter technique in mice and rats. Nat Protoc. 2008;3(9):1422–1434. doi: 10.1038/nprot.2008.138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Larsen TS, et al. The isolated working mouse heart: methodological considerations. Pflugers Arch. 1999;437(6):979–985. doi: 10.1007/s004240050870. [DOI] [PubMed] [Google Scholar]
- Roth DM, Swaney JS, Dalton ND, Gilpin EA, Ross J., Jr Impact of anesthesia on cardiac function during echocardiography in mice. Am J Physiol Heart Circ Physiol. 2002;282(6):H2134–H2140. doi: 10.1152/ajpheart.00845.2001. [DOI] [PubMed] [Google Scholar]
- Pearlman AS, Stevenson JG, Baker DW. Doppler echocardiography: applications, limitations and future directions. Am J Cardiol. 1980;46(7):1256–1262. doi: 10.1016/0002-9149(80)90296-9. [DOI] [PubMed] [Google Scholar]
- Bauer M, et al. Echocardiographic speckle-tracking based strain imaging for rapid cardiovascular phenotyping in mice. Circ Res. 2011;108(8):908–916. doi: 10.1161/CIRCRESAHA.110.239574. [DOI] [PMC free article] [PubMed] [Google Scholar]