

Abstract
The aims of this longitudinal study were to investigate a significant threshold shift (STS) among personnel working on board the Royal Norwegian Navy's (RNoN) vessels between 2012 and 2014 and to identify possible determinants of STS. Hearing thresholds were measured by pure tone audiometry in two consecutive examinations (n = 226). STS was defined as an average change in hearing thresholds ≥ + 10 dB at 2,000 Hz, 3,000 Hz, and 4,000 Hz in either ear. Determinants of STS were assessed through a questionnaire. The incidence of STS was 23.0%. Significant determinants of STS were the number of episodes of temporary threshold shifts (TTS) in the Navy, exposure to continuous loud noise during work on board, and the number of gun shots (in the Navy, hunting, and sports). This study indicated a significant association between noise exposure on board Navy vessels and development of STS.
Keywords: Audiometry, continuous noise exposure, hearing conservation, hearing loss, impulse noise exposure
Introduction
Hearing loss is a common public health problem. In a Norwegian population-based study comprising more than 50,000 participants, disabling hearing loss was found among 10.3% of the participants.[1] Exposure to noise is an important cause of hearing loss and hearing loss is frequently found in workplaces known for high noise levels, e.g., the mining and construction industries.[2,3] In the military, noise exposure is among the most prevalent occupational health hazards, with hearing loss commonly reported.[3,4,5,6]
Noise levels measured in different locations on board the Royal Norwegian Navy's (RNoN) vessels have been found to exceed the recommended maximum noise levels in most vessel classes.[7] Work on board Navy vessels is associated with exposures to continuous noise from the vessel machinery and to impulse noise from shooting and explosions. Although impulse noise exposure has been shown to be more harmful to hearing than continuous noise,[8] there is limited knowledge concerning the effect of long periods of continuous noise without the possibility to recover.
A high prevalence of impaired hearing has been described in previous RNoN studies. Subjectively reduced hearing was reported among 24% of the RNoN employees working either on shore or on board Navy vessels between 2002 and 2003.[9] In a recent cross-sectional study conducted in the RNoN, the prevalence of hearing loss measured by audiometry among personnel working on board Navy vessels was 31.4%, and time spent on board Navy vessels was identified as a predictor.[10]
Military personnel are dependent on proper hearing acuity in order to secure effective verbal communication. Hence, the consequences of impaired hearing are considerable as it may degrade performance and have negative effects on operational readiness during military activities. Previous research concerning impaired hearing in the Navy includes data mainly from hearing conservation programs (HCP) and medical record databases in which information regarding possible determinants of impaired hearing is limited.[11,12] In order to assess cause and effect, longitudinal epidemiological studies are needed.[13]
The aims of this longitudinal study among personnel on board RNoN vessels were to investigate the incidence of significant threshold shift (STS) between 2012 and 2014 and to identify the determinants of STS development.
Methods
Study population
This longitudinal study is part of a project concerning noise exposure and health in the RNoN carried out by university researchers in collaboration with the RNoN. Data were collected in two time periods: from April 2012 to June 2013 (baseline) and from August 2013 to December 2014 (follow-up). The audiometry was performed by trained personnel at three naval bases, supervized by a university researcher.
Two contact persons in the RNoN were provided with a complete sailing plan for the RNoN and lists of personnel on board. The contact persons were responsible for informing the management on board each vessel about the objectives of the project before commencing the examinations. Next, the management was asked to communicate this information to the Navy personnel on board each vessel in plenary. Information was also put up as posters on most vessels. Sailing officers, enlisted and civilians were scheduled to meet for audiometry when they arrived at the naval bases. No conscripts were invited, as their limited time of service made follow-up difficult. When entering the audiometry examination facilities, the Navy personnel received a typed letter with information regarding the study, and those who wished to participate confirmed by signing an informed consent. Each participant was asked to fill out a questionnaire regarding the possible risk factors for hearing loss before completing the audiometric test.
Our intention was to assess the one-year development of hearing loss among Navy personnel. However, due to inaccessibility of participants at the scheduled examination and reduced workforce among the trained hearing test personnel at the naval bases (sick leave and leave of absence), the mean number of days between the baseline and follow-up was 530, ranging 242-959 days.
Questionnaire
A questionnaire was prepared to identify the determinants of STS development between examinations. The questionnaire included questions about vessel affiliation, work history, past and present occupational noise exposures and non-occupational noise exposure, use of hearing protection devices (HPDs), general and ear-specific health, and other exposures that might affect hearing (e.g., diving and smoking) [Table 1]. The trained personnel ensured that the questionnaires were completed.
Table 1.
Questions and response alternatives in a questionnaire concerning noise exposure and health given to Navy personnel in the Royal Norwegian Navy (RNoN), 2013-2014
| Question | Response alternatives | ||
|---|---|---|---|
| Work history | Current vessel affiliation | Free texta | |
| Job category | Work on deck/electrician/cook/engine room personnel/navigator/work in operation room/work in ships office/weapon technician | ||
| Months of sailing in the Navy during the last 12 months | Number of months | ||
| Current and prior occupational noise exposure | Are you currently in your work on board exposed to noise so loud that it is difficult to have a conversation? | No, never <5 h/week 5-15 h/week >15 h/week |
|
| Have you been exposed to impulse noise (explosions, etc.) in your work in the Navy without wearing hearing protection during the last 12 months? | Yes/No | Number of times c | |
| Have you had temporary reduced hearing, fullness or ringing in the ears after being exposed to noise in the Navy during the last 12 months? b | Yes/No | Number of times c | |
| Have you used hearing protection in high-noise areas on board vessels in the Navy during the last 12 months? | Yes, most of the time Sometimes No Of no relevance |
||
| Do you wear hearing protection while shooting? | Yes, most of the time Sometimes No |
||
| Current and prior non-occupational noise exposure | Have you been exposed to impulse noise (explosions, etc.) outside the Navy without wearing hearing protection during the last 12 months? | Yes/No | Number of timesc |
| Have you been hunting during the last 12 months? | Yes/No | ||
| Do you wear hearing protection while hunting? | Yes, most of the time Sometimes No | ||
| Number of gunshots (in the Navy, hunting, and sports) during the last 12 months: | Number of gunshotsc | ||
| Have you been playing in a band during the last 12 months? | Yes/No | ||
| Have you had temporary reduced hearing, fullness, or ringing in the ears after being exposed to noise outside the Navy during the last 12 months?b | Yes/No | Number of timesc | |
| How often have you been attending concerts/disco, etc., playing loud music during the last 12 months? | Weeklyd Sometimes/monthd Sometimes/year Seldom/never |
||
| Are you currently using MP3 player, etc., with plugs/phones? | >6 h/weeke 3-6 h/weeke 1-2 h/week Seldom/never |
||
| Medical history | Have you been diagnosed with any of these diseases during the last 12 months? | Heart disease Hypertension Diabetes, type 2 | Yes/No |
| Have you had otitis during the last 12 months? | Yes/No/I do not know | ||
| Have you had any other ear disease during the last 12 months? | Yes/No | ||
| Have you been hospitalized due to head injury during the last 12 months? | Yes/No | ||
| Have you been using ototoxic medication during the last 12 months (diuretics, broad spectrum antibiotics, cytotoxins)? | Yes/No/I do not know | ||
| Have you been bothered by tinnitus (ringing in the ears) the last 12 months? | Yes/No | A bit bothered/greatly bothered | |
| Have you been bothered by vertigo the last 12 months? | Yes/No | ||
| Do you believe that your hearing has impaired during the last 12 months? | Yes/No/I do not know | ||
| Other current and prior occupational or non-occupational exposure | Have you been diving during the last 12 months? | Yes, professional in the Navy Yes, professional outside the Navy Yes, leisure diving No, never |
|
| Have you had ear damage following diving during the last 12 months (being treated in recompression chamber due to the ear damage)? | Yes/No | ||
| How often have you been working with organic solvents (paint/washing with thinner) during the last 12 months? | Daily Weekly Monthly Seldom/never |
||
| Have you been smoking the last 12 months? | Yes, daily Sometimes Earlier No |
||
| Have you been using moist snuff the last 12 months? | Yes, daily Sometimes Earlier No |
||
aGrouped in five vessel classes, bDefined as temporary threshold shift (TTS), cDeterminants grouped in approximately equal sizes as quartiles could not be provided, dThe alternatives “weekly” and “sometimes/month” were merged due to low numbers to the alternative “≥sometimes/month”, eThe alternatives “>6 h/week” and “3-6 h/week” were merged due to low numbers to the alternative “≥3 h/week”
Pure tone audiometry
Pure tone audiometry was made using the Interacoustics AS, (Audiometer Allé 15500, Middelfart, Denmark), AD226 audiometer with Amplivox Audiocups or Peltor earphones. The audiometry was performed in sound booths. Ambient noise levels inside the sound booths were measured using Brüel and Kjær (Nærum, Denmark) sound level meter hand-held analyzer type 2250 (15-s measurement period) and were found to be in accordance with ISO 8253-1.[14] Interacoustics AD226 provided hearing thresholds from - 10 dB. The following frequencies were measured for both ears separately: 250 Hz, 500 Hz, 1,000 Hz, 2,000 Hz, 3,000 Hz, 4000 Hz, 6,000 Hz, and 8,000 Hz. Hearing threshold levels were in general established using an automated test procedure; however, manual audiometry was performed for participants with present tinnitus, known hearing loss, or uncertainty regarding measured hearing thresholds. The sound level meter used was calibrated immediately prior to the measurements while audiometers and fitted earphones were calibrated annually.[14]
In order to ensure proper data quality, a test protocol was developed. After every examination, a stepwise checklist was completed to make sure that the protocol had been followed. The presence of ear canal obstruction was assessed by otoscopy prior to audiometry and in cases of complete obstruction, the cerumen was removed and a new audiometric test was completed at least 1 week later. Exposure to loud area noise, loud workshop noise or other loud noise exposure in the previous 16 h was noted in the checklist. Temporary threshold shift (TTS) was suspected among participants with recent loud noise exposure and hearing thresholds ≥25 dB in either ear at 3,000 Hz, 4,000 Hz, or 6,000 Hz. These participants could only be included in the study if a new audiometry was conducted without prior exposure to loud noise. Audiometry was not performed if participants had acute airway infections involving sinuses, nose or ears, and a new appointment was made when these participants were asymptomatic. All audiometric tests were evaluated by the university researcher and an occupational health physician in collaboration with an otolaryngologist, and referrals were made when necessary.
Selection of participants
A total of 938 Navy personnel were scheduled to meet for the baseline examination [Figure 1]. However, 149 did not show up and 17 did not wish to participate in the study. Thus, data were collected from 772 participants giving a response rate at a baseline of 82%. Due to missing compliance with the protocol and technical failure of one of the audiometers, the number of participants included at the baseline was reduced to 605.
Figure 1.
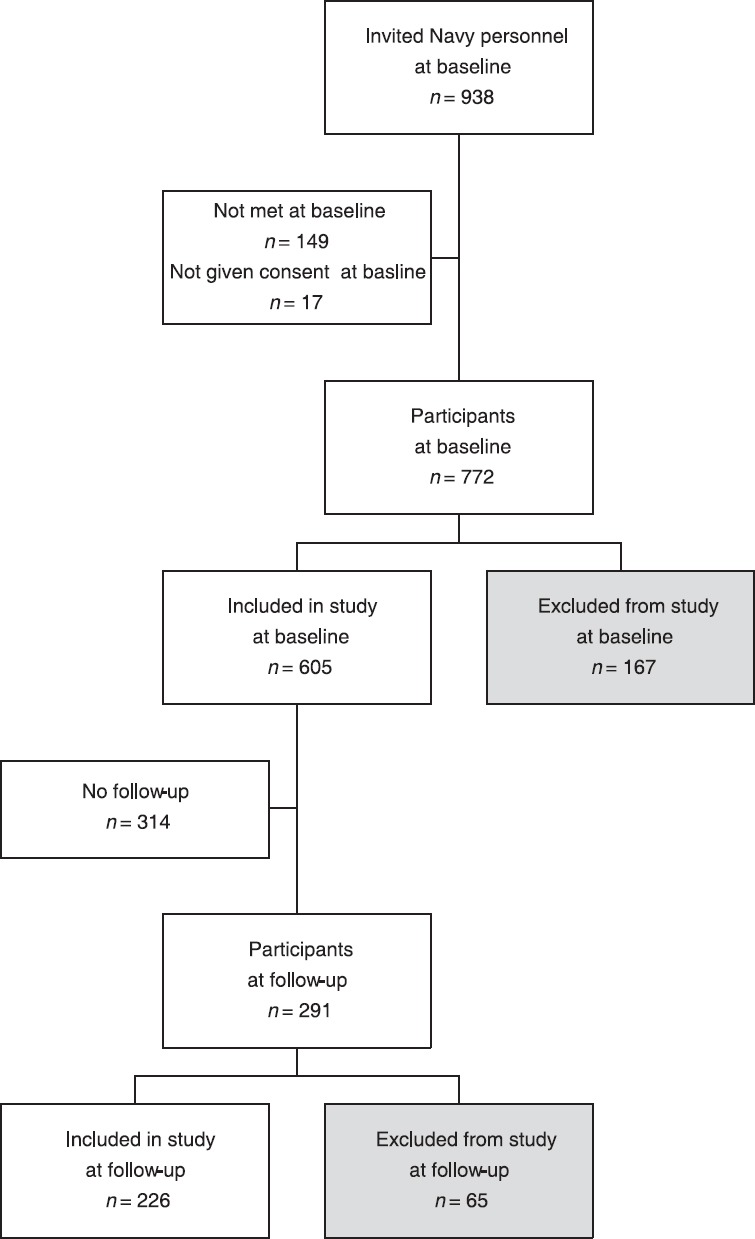
Navy personnel participating in the Royal Norwegian Navy (RNoN) study on hearing loss, 2012-2014. The gray shaded boxes indicate participants who were excluded. Exclusion at baseline due to noncompliance with the protocol (n = 81) or due to technical failure of one of the audiometers (n = 86). Exclusion at follow-up due to noncompliance with the protocol (n = 65)
Of the 605 participants included at the baseline, 291 completed the follow-up (response rate of 48%). Unfortunately, data from 65 participants in the follow-up were excluded as the examination was not performed in accordance with the protocol. Thus, the longitudinal study comprised data from 226 participants.
Loss of follow-up (n = 314) was due to reassignment to work on shore (n = 63), termination of service (n = 129), or other reasons (n = 122) such as difficulties in synchronizing the hearing examinations with the prearranged sailing pattern as well as absence due to courses, time off, or leave of absence/sick leave. All participants agreed to join the study by signing an informed consent at baseline. Thus, we do not believe that loss of follow-up might be caused by refusal to participate.
Data analysis
The design of the study was longitudinal and prospective. STS was calculated based on results from the two audiometric tests provided for each participant, and was defined as an average change in hearing thresholds ≥ + 10 dB at 2,000 Hz, 3,000 Hz, and 4,000 Hz in either ear in accordance with definitions used by the US Navy[15] and by the Occupational Safety and Health Administration (OSHA).[16]
Mean hearing thresholds at baseline and follow-up were calculated for each of the frequencies 250 Hz, 500 Hz, 1,000 Hz, 2,000 Hz, 3,000 Hz, 4,000 Hz, 6,000 Hz, and 8,000 Hz for the left ear and right ear separately. For each of these frequencies, median expected hearing thresholds by age (at follow-up) and gender were calculated as proposed by ISO 7029:2000, selecting the 50 percentile.[17]
Paired sample t-test was used to determine whether the mean hearing threshold for each frequency differed significantly between the two audiometric tests for the left ear and right ear. This test was also used to assess whether the mean hearing threshold for each frequency at follow-up differed significantly from the median hearing thresholds as expected by ISO 7029:2000.
Log binomial univariate regression analyses were performed to estimate associations between independent determinants from the follow-up questionnaire and STS. Log binomial multivariate regression analysis was then performed to assess the relationship between significant noise exposure determinants and STS.
Continuous determinants from the questionnaire were initially categorized in quartiles. However, due to poor spread of data, we chose to distribute the exposed groups of the following determinants into approximately equal sizes: number of episodes of impulse noise both in and outside the Navy, number of gun shots (in the Navy, hunting, and sports) and number of TTS episodes in and outside the Navy. Results were presented as relative risks (RRs) with 95% confidence intervals (CIs). P values < 0.05 were considered to be significant.
Difference in prevalence of hearing loss at baseline among the participants included in the study compared to participants who did not did not meet at follow-up was assessed using the chi-square test. In these analyses, hearing loss was defined as ≥25 dB at 3,000 Hz, 4,000 Hz or 6,000 Hz in either ear.
The data were analyzed using IBM SPSS Statistics, version 22, (Armonk, NY, USA).
Research ethics
The study was approved by the Regional Committee of Medical and Health Research Ethics (REC South East) and was performed in accordance with the 1964 Declaration of Helsinki and its later amendments. The participants were informed about the research project and gave written consent to take part in the study. Withdrawal from the study could be made at any point. There was no payment or other benefit for participation. Each individual audiometric test was evaluated. If any deviation from normality was discovered, the participants were informed and given advice for help in a personal letter. The data were otherwise registered with id numbers, not names, during the statistical analyses. The list of id numbers and names was locked safe by the researchers. The audiometry data were not accessible to anyone in the Navy except the trained personnel performing the audiometry. The trained personnel were not allowed to report the results to anyone except the researchers. Thus, it was emphasized that the audiometry results would not be used in evaluation of medical suitability for continued service. The RNoN funded the study but a contract between the RNoN and the university stated that the university had the right to publish all results at the group level.
Results
Among the 226 participants, 217 were males and nine were females. The mean age was 33 years, ranging 20-53 years. On an average, the participants had sailed for five of the last 12 months. The incidence of STS among the Navy personnel during the study period (April 2012 to December 2014) was 23.0%.
For the left ear, significantly higher mean hearing thresholds (i.e., impaired hearing) were found at frequencies 250-6000 Hz, and significantly lower at 8000 Hz at follow-up compared to baseline [Figure 2]. For the right ear, mean hearing thresholds were significantly higher at follow-up than at the baseline at the frequencies 1,000 Hz, 2,000 Hz, 3,000 Hz, and 4,000 Hz [Figure 2].
Figure 2.
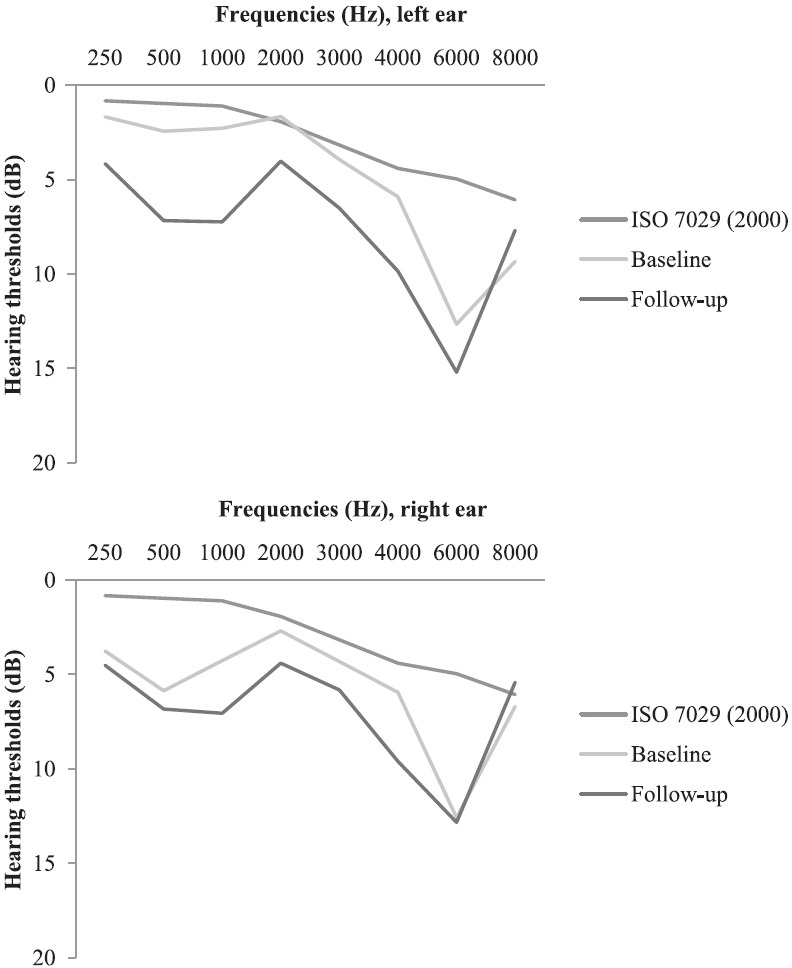
Mean hearing thresholds (dB) 250-8,000 Hz measured in 226 personnel from the Royal Norwegian Navy in a study on hearing loss 2012-2014
The mean hearing thresholds measured at follow-up were significantly higher than the International Organization for Standardization (ISO) standard at 250-6,000 Hz for both ears [Figure 2].
Participants who reported exposure to >5 episodes of TTS in the Navy during the last 12 months had a significantly higher risk of STS in the log binomial univariate analyses compared to Navy personnel without this exposure [Table 2]. Participants who were currently exposed to >15 h/week of loud noise during work on board (making it difficult to have a conversation) had a significantly higher risk of STS compared to Navy personnel without this exposure [Table 2]. A significantly higher risk of STS was also found among participants who had been shooting 1-200 gun shots (in the Navy, hunting, or sports) during the last 12 months compared to participants who had not been shooting at all [Table 2]. The estimates also increased for shooting >200 gun shots although these were not significant. In multivariate regression analyses, the two noise exposure determinants were both associated with a higher STS risk although estimates were slightly reduced (>15 h/week of loud noise: RR 1.83, CI 0.80-4.23 and 1-200 gunshots: RR 2.35, CI 0.95-5.81). TTS was not included in the log binomial multivariate regression analysis as TTS is caused by noise exposure and is not considered to be an individual determinant of impaired hearing.
Table 2.
Significant determinants of significant threshold shift (STS) in 226 Navy personnel from the Royal Norwegian Navy (RNoN), measured in two consecutive audiometric examinations between 2012 and 2014
| Determinant | Total | STSa | No STS | |||
|---|---|---|---|---|---|---|
| n | n (%) | n (%) | RRb | 95% CIc | ||
| “Have you had temporary reduced hearing, fullness, or ringing in the earsd after being exposed to noise in the Navy during the last 12 months?”e | 0 (ref) | 178 | 37 (20.8) | 141 (79.2) | 1 | |
| 1-5 | 24 | 5 (20.8) | 19 (79.2) | 1.00 | 0.44-2.30 | |
| > 5 | 23 | 10 (43.5) | 13 (56.5) | 2.09* | 1.21-3.62 | |
| “Are you currently in your work on board exposed to noise so loud that it is difficult to have a conversation?” | No, never (ref) | 32 | 7 (21.9) | 25 (78.1) | 1 | |
| <5 h/week | 142 | 30 (21.1) | 112 (78.9) | 0.97 | 0.47-2.00 | |
| 5-15 h/week | 36 | 7 (19.4) | 29 (80.6) | 0.89 | 0.35-2.26 | |
| >15 h/week | 16 | 8 (50.0) | 8 (50.0) | 2.29* | 1.01-5.18 | |
| “Number of gun shots (in the Navy, hunting and sports) during the last 12 months” | 0 (ref) | 44 | 5 (11.4) | 39 (88.6) | 1 | |
| 1-200 | 87 | 25 (28.7) | 62 (71.3) | 2.53* | 1.04-6.15 | |
| >200 | 95 | 22 (23.2) | 73 (76.8) | 2.04 | 0.83-5.03 | |
aSignificant threshold shift: Average change in hearing threshold ≥ + 10 dB at 2,000 Hz, 3,000 Hz, and 4,000 Hz in either ear, bRR = Relative risk, cCI = Confidence interval, dDefined as temporary threshold shift (TTS), eOne missing participant, *Statistical significance
No significant association was found between STS and the following determinants from the questionnaire: age, gender, vessel class, job category, duration of sailing, impulse noise in or outside the Navy, use of HPDs, work with organic solvents, diving, heart disease, hypertension, diabetes, otitis or other ear disease, tinnitus, TTS outside the Navy, vertigo, admittance to hospital due to head injury, use of ototoxic medication, use of cigarettes or moist snuff, hunting, playing in a band or attending concerts/disco, use of MP3 player, and subjectively impaired hearing. No significant association was found between STS and number of days between baseline and follow-up.
Analyses were made to assess the prevalence of hearing loss at baseline among the participants who completed both examinations, compared to the participants who only participated at baseline. The prevalence of hearing loss among the 226 included in the present study (35%) and the 314 who did not meet at follow-up (27.8%) was not significantly different (P = 0.08).
Discussion
After an observation period ranging from 8 months to 2.5 years, 23% of the Navy personnel developed STS and the mean hearing thresholds had deteriorated significantly between the two audiometric tests for the majority of frequencies. The mean hearing thresholds were significantly higher than expected by ISO 7029:2000 at all frequencies but 8,000 Hz. Univariate analyses indicated a significant association between the number of episodes of TTS in the Navy and STS development. Participants who were currently exposed to >15 h/week of loud noise (making it difficult to have a conversation) during work on board Navy vessels had a significantly higher risk of STS compared to participants without this exposure and participants who had been shooting 1-200 gunshots (in the Navy, hunting, and sports) the last 12 months had a higher risk of STS than participants who had not been shooting. The multivariate regression analyses showed an increased risk of STS for both these two noise exposure determinants, however with slightly decreased estimates when compared to the univariate model. A clear interpretation of whether the continuous noise or impulse noise was most important for developing STS was difficult due to low numbers.
Two previous US Navy studies have reported similar occurrences of STS as found in our study.[18,19] Investigation of 12,492 audiometric records from the personnel working on board vessels in the US Navy revealed an STS incidence of 29% between 1987 and 1990.[18] Records collected between 1995 and 1999 showed an STS incidence of 18.1% among 54,057 US Navy personnel either working on board vessels or ashore.[19] The different STS rates in the two studies might be explained by different noise exposures on board vessels and ashore, indicating a higher risk of hearing damage among personnel on board Navy vessels.[19] This hypothesis is supported by our present findings, showing that personnel exposed to noise during their work on board had a significantly higher risk of STS. Our findings correspond with results from a previous investigation of audiometric records from almost 268,000 enlisted US Navy sailors from 1982 to 2004. This study showed that personnel working 1 year on board warships had a higher risk of STS (RR 1.06, CI 1.06-1.07) than personnel working 1 year on shore (RR 1.04, CI 1.03-1.04).[20] In a recent cross-sectional study conducted in the RNoN, a significant association between hearing loss and years of sailing was found, indicating a 0.48-dB increase in hearing threshold level (poorer hearing) at 4,000 Hz per year of sailing.[10] An association between the number of months of sailing and STS was not found in the current study probably due to the short observation period.
As few Navy studies have reported on the incidence of STS; it is relevant to compare our findings with results from other military branches, which may have similar exposures such as the Army. Studies from the Swedish Army have demonstrated high levels of noise exposure, both to continuous noise from armored vehicles (103-107 dB(A)) and impulse noise from various firearms (156-184 dB SPL).[21,22] The development of deteriorated hearing thresholds among conscripts in the Swedish Army was evaluated in two studies showing STS incidences of 6.6%[22] and 7.9%.[21] The STS incidences described in these studies were lower than the STS incidence found in our study. The higher STS incidence found in our study might be explained by continuous exposure to moderate noise levels for days and weeks on board RNoN vessels.[7] However, the lower incidences described in the Swedish Army studies might also be explained by a shorter observation period (7-11 months), and thereby shorter exposure time, and a lower average age (18-19 years) with a lower risk of age-related hearing loss. Different STS incidences might also result from the use of different STS definitions. In the Swedish Army studies, STS was defined as a 15-dB decline in hearing thresholds in at least one ear, at one of the frequencies 250-8000 Hz[21] or 500-8000 Hz.[22] Hence, when compared to our STS definition, a greater shift was needed to induce STS in the Swedish studies although more frequencies were included. The varying incidence of STS can also be explained by use of different audiometric test methods. We included registration of hearing thresholds below 0 dB while the Swedish studies limited registration to hearing thresholds of 10 dB or above.[21,22] Registration of hearing thresholds below 0 dB will detect deteriorated hearing thresholds at an earlier stage, thus increasing STS.
We found a significant association between the number of gunshots (in the Navy, hunting, and sports) and STS. However, interpretation was difficult as there was no linear relationship between this determinant and STS. One might assume that the participants with the highest noise exposure were more tolerant to noise and thus, did not develop STS. The participants with the highest number of gunshots could also have been more experienced, with proper use of HPDs. An association between shooting and hearing loss has previously been described in both military and population-based studies.[23,24,25,26] In a study on Brazilian military personnel, the group who had practiced handgun shooting regularly [with noise levels ranging 119-133 dB(C)] had significantly poorer hearing than the administrative staff.[26] Nondahl et al. assessed the relationship between recreational firearm use and high-frequency hearing loss in a population-based US study comprising 3,753 participants. The authors found that participants who had been engaged in target shooting during the last year had a higher risk of hearing loss compared to participants who had not been shooting (OR 2.00, CI 1.15-3.46).[25]
We found that the measured hearing thresholds were poorer than the expected hearing thresholds according to ISO 7029:2000[17] for all frequencies but 8,000 Hz. The screening criteria in the ISO 7029:2000 is based on subjects without symptoms of ear disease, cerumen, or any undue history of noise exposure. These criteria are similar to those utilized in our protocol; however, in our study we had no restrictions regarding previous history of noise exposure. Hence, it is reasonable to assume that the poorer hearing thresholds measured in our study were caused by noise exposure. Our findings are in line with previous research on the US Navy and US Marine Corps personnel indicating that mean threshold levels for men were worse than the OSHA age-adjusted values.[6,16] Deteriorated hearing thresholds were also discovered for officers serving in an infantry regiment of the Swedish Army.[27] Here, significant hearing loss was found for all frequencies investigated when compared to ISO 1999(1990), database A.[28]
The audiometric curves in our study showed a downward slope from 2,000 Hz with a notch at 6,000 Hz and improvement at 8,000 Hz for both ears at both tests. Previous studies have assessed audiometric curves in relation to continuous noise and impulse noise, however with some discrepancy.[23,24,29] In a large Norwegian population-based study comprising more than 50,000 participants, exposure to occupational noise was associated with threshold shifts at 3,000-4,000 Hz while exposure to impulse noise (e.g., explosions and shooting) showed the strongest effects at 3,000-8,000 Hz.[24] Similar results were found when comparing industrial workers engaged in recreational shooting with non-shooting industrial workers. Participants who were engaged in recreational shooting had a 5-10 dB poorer hearing sensitivity for 3,000 Hz, 4,000 Hz and 6,000 Hz than those who were not shooting.[29] In a study examining 361 Finnish Army conscripts with acute acoustic trauma, the greatest hearing loss was found at 6,000 Hz, thus equivalent to our study.[23] Although our study showed that hearing impairment dominated at the higher frequencies, we discovered impaired hearing at the lower frequencies (500-1,000 Hz). In the Finnish study, low frequency hearing loss (500-2,000 Hz) occurred among 25% of the conscripts and was thought to be explained by noise exposure from cannons and explosions.[23] The hearing loss developed among the participants in our study might have been caused both by continuous noise and impulse noise; yet we cannot determine their separate contribution by evaluating audiometric findings. However, both exposures might be harmful to hearing and studies have indicated that the combination of the two cause more profound changes than either separately.[30]
We found that hearing was more impaired in the right ear at low frequencies and in the left ear at high frequencies. Our findings are in line with previous literature concerning left-right asymmetry. A Finnish population-based study comprising 3,487 participants also described poorer hearing in the right ear at low frequencies and in the left ear at high frequencies.[31] In military studies, great loss in the left ear at high frequencies has been emphasized, and has been explained by exposure to gun shots.[23,32]
Our questionnaire data indicated a higher risk of STS among participants with prior occurrence of TTS due to noise exposure in the Navy. Previous military studies have assessed the association between TTS and noise exposure in terms of aircraft noise exposure[33] and exposure during shooting.[34] In these studies, only minor TTS was registered. However, our study indicates that TTS in the Navy is a potential threat for development of permanent threshold shifts (PTS).
The longitudinal design of our study in combination with objective audiometry results and the utilization of detailed questionnaires on potential determinants made it possible to address cause–effect associations. Data from previous military studies are frequently acquired from frequently acquired from HCPs and and medical record databases with limited information on possible determinants of hearing impairment.
When an STS is discovered, one would normally acquire a follow-up shortly after the last test to verify the hearing impairment. Unfortunately, we did not have resources to provide an additional audiometry soon after the measurements as the participants were sailing in many different locations, and the RNoN could not coordinate more examinations during the time ashore. However, as we used a strict protocol and a checklist to assure proper quality in audiometry measurements, we believe to have limited the introduction of false positive results. The use of this strict protocol for data collection and audiometry measurement is a strength of our study.
The results from the audiometric tests were used to assess hearing capabilities among the RNoN personnel and not to assess individual medical skillfulness related to work on board Navy vessels. The participants were assured that their results would not be given to anyone except the researchers. The management on board the vessels scheduled appointments for all Navy personnel. They had no information regarding individual hearing abilities; hence, they could not influence the outcome.
We were not able to include as many participants as intended at follow-up, primarily because a significant number of participants was reassigned or had their service terminated. Although the prevalence of hearing loss at baseline was higher among the participants included in the study than among personnel who did not meet at follow-up, the difference was not significant. Hence, we do not believe that the loss of follow-up has influenced the results and consider the participants included to be representative of the Navy population. Still, a higher response rate would have been an advantage.
Another limitation of this study was that we could not present individual objective noise exposure data. Ideally, detailed information regarding individual noise exposure on board and the time of sailing should be collected using individual log books. However, such quantitative exposure assessment was not feasible in this field study.
The incidence of hearing loss among Navy personnel was higher than anticipated in this young population being selected for work on board Navy vessels by strict medical criteria. Our results indicate that both the continuous noise exposure to moderate noise levels on board and impulse noise exposure is detrimental to hearing. Based on the findings from this and recent RNoN studies,[7,10,35] we are of the opinion that a more specified and targeted HCP should be implemented in the RNoN. Reduction of noise exposure and further awareness of the harmful effects of noise are important in order to prevent impaired hearing.
Financial support and sponsorship
The study is funded by the Royal Norwegian Navy.
Conflicts of interest
The authors declare that there are no conflicts of interest.
Acknowledgements
We would like to thank Hjalmar Johansen, Christin Pedersen, and Eirik Veum Wilhelmsen in the RNoN for cooperation. We thank Ellen Skare, Unni Nicolaysen, Pål Pedersen, Jane Berit Berg, Hilde Kristin Pettersen, and Geir Marvin Engerstø for collecting the data, Ågot Irgens and Lorentz Irgens for helpful support with the statistics and proofreading, and Truls Gjestland, Hilde Gundersen, Camilla Hauge, Gunhild Koldal, Ole Jacob Møllerløkken, Gunnhild Oftedal, and Erlend Sunde for valuable contributions in completion of the project.
References
- 1.Engdahl B, Tambs K. Occupation and the risk of hearing impairment-results from the Nord-Trøndelag study on hearing loss. Scand J Work Environ Health. 2010;36:250–7. doi: 10.5271/sjweh.2887. [DOI] [PubMed] [Google Scholar]
- 2.Tak S, Calvert GM. Hearing difficulty attributable to employment by industry and occupation: An analysis of the National Health Interview Survey-United States, 1997 to 2003. J Occup Environ Med. 2008;50:46–56. doi: 10.1097/JOM.0b013e3181579316. [DOI] [PubMed] [Google Scholar]
- 3.Lie A, Skogstad M, Johannessen HA, Tynes T, Mehlum IS, Nordby KC, et al. Occupational noise exposure and hearing: A systematic review. Int Arch Occup Environ Health. 2016;89:351–72. doi: 10.1007/s00420-015-1083-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Meyer JD, Chen Y, McDonald JC, Cherry NM. Surveillance for work-related hearing loss in the UK: OSSA and OPRA 1997-2000. Occup Med (Lond) 2002;52:75–9. doi: 10.1093/occmed/52.2.75. [DOI] [PubMed] [Google Scholar]
- 5.Helfer TM, Canham-Chervak M, Canada S, Mitchener TA. Epidemiology of hearing impairment and noise-induced hearing injury among U.S. military personnel, 2003-2005. Am J Prev Med. 2010;38(Suppl):S71–7. doi: 10.1016/j.amepre.2009.10.025. [DOI] [PubMed] [Google Scholar]
- 6.Bohnker BK, Page JC, Rovig G, Betts LS, Muller JG, Sack DM. U.S. Navy and marine corps hearing conservation program, 1995-1999: Mean hearing thresholds for enlisted personnel by gender and age groups. Mil Med. 2002;167:132–5. [PubMed] [Google Scholar]
- 7.Sunde E, Irgens-Hansen K, Moen BE, Gjestland T, Koefoed VF, Oftedal G, et al. Noise and exposure of personnel aboard vessels in the Royal Norwegian Navy. Ann Occup Hyg. 2015;59:182–99. doi: 10.1093/annhyg/meu075. [DOI] [PubMed] [Google Scholar]
- 8.Mantysalo S, Vuori J. Effects of impulse noise and continuous steady state noise on hearing. Br J Ind Med. 1984;41:122–32. doi: 10.1136/oem.41.1.122. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Moen BE, Koefoed VF, Bondevik K, Haukenes I. A survey of occupational health in the Royal Norvegian Navy. Int Marit Health. 2008;59:35–44. [PubMed] [Google Scholar]
- 10.Irgens-Hansen K, Sunde E, Bråtveit M, Baste V, Oftedal G, Koefoed V, et al. Hearing loss in the Royal Norwegian Navy: A cross-sectional study. Int Arch Occup Environ Health. 2015;88:641–9. doi: 10.1007/s00420-014-0988-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Theodoroff SM, Lewis MS, Folmer RL, Henry JA, Carlson KF. Hearing impairment and tinnitus: Prevalence, risk factors, and outcomes in US service members and veterans deployed to the iraq and Afghanistan wars. Epidemiol Rev. 2015;37:71–85. doi: 10.1093/epirev/mxu005. [DOI] [PubMed] [Google Scholar]
- 12.Henselman LW, Henderson D, Shadoan J, Subramaniam M, Saunders S, Ohlin D. Effects of noise exposure, race, and years of service on hearing in U.S. Army soldiers. Ear Hear. 1995;16:382–91. doi: 10.1097/00003446-199508000-00005. [DOI] [PubMed] [Google Scholar]
- 13.Humes LE, Joellenbeck LM, Durch JS. Washington, DC: The National Academies Press; 2005. Noise and Military Service: Implications for Hearing Loss and Tinnitus. [Google Scholar]
- 14.Geneva: International Organization of Standardization; 2010. ISO 8253-1 (2010) Acoustics — Audiometric test methods — Part 1: Pure-tone air and bone conduction audiometry. [Google Scholar]
- 15.DoD Instruction Hearing Conservation Program. 2010:6055–12. [Google Scholar]
- 16.OSHA Occupational Safety and Health Standards 29 CFR 1904.10(C) [Google Scholar]
- 17.Geneva: International Organization of Standardization; 2000. ISO 7029 (2000) Acoustics — Statistical distribution of hearing thresholds as a function of age. [Google Scholar]
- 18.Wolgemuth KS, Luttrell WE, Kamhi AG, Wark DJ. The effectiveness of the Navy's hearing conservation program. Mil Med. 1995;160:219–22. [PubMed] [Google Scholar]
- 19.Bohnker BK, Page JC, Rovig G, Betts LS, Sack DM. Navy Hearing Conservation Program: Threshold shifts in enlisted personnel, 1995-1999. Mil Med. 2002;167:48–52. [PubMed] [Google Scholar]
- 20.Trost RP, Shaw GB. Statistical analysis of hearing loss among Navy personnel. Mil Med. 2007;172:426–30. doi: 10.7205/milmed.172.4.426. [DOI] [PubMed] [Google Scholar]
- 21.Muhr P, Månsson B, Hellström PA. A study of hearing changes among military conscripts in the Swedish Army. Int J Audiol. 2006;45:247–51. doi: 10.1080/14992020500190052. [DOI] [PubMed] [Google Scholar]
- 22.Muhr P, Rosenhall U. The influence of military service on auditory health and the efficacy of a Hearing Conservation Program. Noise Health. 2011;13:320–7. doi: 10.4103/1463-1741.82965. [DOI] [PubMed] [Google Scholar]
- 23.Ylikoski J. Acute acoustic trauma in finnish conscripts. Etiological factors and characteristics of hearing impairment. Scand Audiol. 1989;18:161–5. doi: 10.3109/01050398909070741. [DOI] [PubMed] [Google Scholar]
- 24.Tambs K, Hoffman HJ, Borchgrevink HM, Holmen J, Engdahl B. Hearing loss induced by occupational and impulse noise: Results on threshold shifts by frequencies, age and gender from the nord-trøndelag hearing loss study. Int J Audiol. 2006;45:309–17. doi: 10.1080/14992020600582166. [DOI] [PubMed] [Google Scholar]
- 25.Nondahl DM, Cruickshanks KJ, Wiley TL, Klein R, Klein BE, Tweed TS. Recreational firearm use and hearing loss. Arch Fam Med. 2000;9:352–7. doi: 10.1001/archfami.9.4.352. [DOI] [PubMed] [Google Scholar]
- 26.Heupa AB, Gonçalves CG, Coifman H. Effects of impact noise on the hearing of military personnel. Braz J Otorhinolaryngol. 2011;77:747–53. doi: 10.1590/S1808-86942011000600011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Christiansson BA, Wintzell KA. An audiological survey of officers at an infantry regiment. Scand Audiol. 1993;22:147–52. doi: 10.3109/01050399309047460. [DOI] [PubMed] [Google Scholar]
- 28.Geneva: International Organization of Standardization; 1990. ISO 1999 (1990) Acoustics — Determination of occupational noise exposure and estimation of noise-induced hearing impairment. [Google Scholar]
- 29.Stewart M, Konkle DF, Simpson TH. The effect of recreational gunfire noise on hearing in workers exposed to occupational noise. Ear Nose Throat J. 2001;80:32. [PubMed] [Google Scholar]
- 30.Hamernik RP, Henderson D, Crossley JJ, Salvi RJ. Interaction of continuous and impulse noise: Audiometric and histological effects. J Acoust Soc Am. 1974;55:117–21. doi: 10.1121/1.1928141. [DOI] [PubMed] [Google Scholar]
- 31.Pirilä T, Jounio-Ervasti K, Sorri M. Left-right asymmetries in hearing threshold levels in three age groups of a random population. Audiology. 1992;31:150–61. doi: 10.3109/00206099209072910. [DOI] [PubMed] [Google Scholar]
- 32.Cox HJ, Ford GR. Hearing loss associated with weapons noise exposure: When to investigate an asymmetrical loss. J Laryngol Otol. 1995;109:291–5. doi: 10.1017/s0022215100129950. [DOI] [PubMed] [Google Scholar]
- 33.Kuronen P, Sorri MJ, Pääkkönen R, Muhli A. Temporary threshold shift in military pilots measured using conventional and extended high-frequency audiometry after one flight. Int J Audiol. 2003;42:29–33. doi: 10.3109/14992020309056082. [DOI] [PubMed] [Google Scholar]
- 34.Olszewski J, Mi³oñski J, Su³kowski WJ, Majak J, Olszewski S. Temporary hearing threshold shift measured by otoacoustic emissions in subjects exposed to short-term impulse noise. Int J Occup Med Environ Health. 2005;18:375–9. [PubMed] [Google Scholar]
- 35.Irgens-Hansen K, Gundersen H, Sunde E, Baste V, Harris A, Bråtveit M, et al. Noise exposure and cognitive performance: A study on personnel on board Royal Norwegian Navy vessels. Noise Health. 2015;17:320–7. doi: 10.4103/1463-1741.165057. [DOI] [PMC free article] [PubMed] [Google Scholar]