

Abstract
The presence and absence of distortion product otoacoustic emissions (DPOAEs) as well as DPOAE amplitudes were compared between college music majors and a control group of nonmusic majors. Participants included 28 music majors and 35 nonmusic majors enrolled at a university with ages ranging from 18-25 years. DPOAEs and hearing thresholds were measured bilaterally on all the participants. DPOAE amplitudes were analyzed at the following f2 frequencies: 1,187 Hz, 1,500 Hz, 1,906 Hz, 2,531 Hz, 3,031 Hz, 3812 Hz, 4,812 Hz, and 6,031 Hz. Significantly more music majors (7/28) than nonmusic majors (0/35) exhibited absent DPOAEs for at least one frequency in at least one ear. Both groups of students reported similar histories of recreational and occupational noise exposures that were unrelated to studying music, and none of the students reported high levels of noise exposure within the previous 48 h. There were no differences in audiometric thresholds between the groups at any frequency. At DPOAE f2 frequencies from 3,031 Hz to 6,031 Hz, nonsignificantly lower amplitudes of 2-4 dB were seen in the right ears of music majors versus nonmajors, and in the right ears of music majors playing brass instruments compared to music majors playing nonbrass instruments. Given the greater prevalence of absent DPOAEs in university music majors compared to nonmusic majors, it appears that early stages of cochlear damage may be occurring in this population. Additional research, preferably longitudinal and across multiple colleges/universities, would be beneficial to more definitively determine when the music students begin to show signs of cochlear damage, and to identify whether any particular subgroups of music majors are at a greater risk of cochlear damage.
Keywords: Distortion product otoacoustic emissions (DPOAEs), hearing conservation, music-induced hearing loss, noise-induced hearing loss
Introduction
Repeated exposures to high levels of sound are known to cause hearing loss.[1,2,3] The National Institute for Occupational Safety and Health (NIOSH)[1] and the World Health Organization[2] recommend a maximum 8-h exposure level of 85 dBA. They also recommend a 3-dBA time-intensity tradeoff, which means that for every 3 dBA increase in the intensity level of the noise, the recommended exposure time is halved.[1,2] In developed and many developing countries, noise exposure in occupational/industrial settings is regulated by the government, and the exposure limits are either identical or similar to the NIOSH/WHO recommendations.[3] In recreational/leisure activities or when occupational and leisure activities overlap, however, it is difficult to impossible to fully regulate noise exposure. This is the case for amateur and professional musicians. Portions of their rehearsal and performance schedule may be for a defined time in a specific occupational environment (e.g., a professional orchestra rehearsal or scheduled performance) but the amateur and professional musicians also rehearse and perform on their own variable schedule in a range of personal/private and professional/occupational settings. Musicians, therefore, can be exposed to variable and often unregulated sound levels that may damage their hearing and reduce their ability to practice their profession or hobby. If any damage could be detected in its earliest stage, it may provide extra motivation for musicians to take preventive measures to avoid additional, and likely more disruptive, damage to their hearing.
A number of studies have found that musicians and music students are exposed to potentially dangerous sound levels. Exposure levels were measured in Chicago Symphony Orchestra musicians during rehearsals over 2 different weeks.[4] Dosimeters with microphones were placed on the musicians’ collars, and the measured 2-3-h Leq values ranged 79-99 dBA (mean of 89.3 dBA), which converted to 8-h equivalent Leq values, using the NIOSH 3 dB exchange rate of 74.7-94.7 (mean of 85.5 dBA). It was also found that the brass players had more exposure to slightly higher sound levels. In another study,[5] Leq values measured using personal dosimetry on amateur musicians in a brass band in Norway ranged 92-100 dBA, with a mean of 96 dBA, over a mean noise sampling time of 3.33 h. Additional research has been performed on college-level musicians. Of 14 music majors participating in a 50-min jazz ensemble class, all were exposed to Leq values that exceeded the daily recommended NIOSH dose.[6] The 50-min Leq values ranged 95-105.8 dBA (mean of 99.5 dBA), which represented 100.1-825% of the daily recommended dose. Sound levels ranging 105-120 dBC have also been measured from various positions at an indoor university marching band rehearsal.[7]
Potentially dangerous sound exposure levels can also occur during solitary practice sessions.[8] Using microphones pinned to the participants, Leq values were measured for eight college trumpet players during one individual 1-h practice session, and for seven trumpet players during two additional individual practice sessions. During the second of these sessions, the musicians wore E.A.R earplugs. For each session, the musicians were instructed to practice as they normally would, including brief breaks as necessary to adjust music sheets and take drinks of water. The mean Leq values across the eight players during the first practice session ranged 90.8-98.1 dBA (mean of 94.8 dBA), and the levels recorded during the second and third sessions were 93.3-98.2 dBA (mean of 96.1 dBA) and 93.0-99.0 dBA (mean of 96.0 dBA), respectively.
Exposure to these dangerous sound levels can damage the outer hair cells of the cochlea as well as other structures of the auditory system.[9] Evoked otoacoustic emissions (OAEs) are generated by the outer hair cells in response to sound presented to the ear, and they can provide objective information about the integrity of the outer hair cells.[10,11,12,13] Two types of evoked OAEs are used clinically, transient evoked otoacoustic emissions (TEOAEs) and distortion product otoacoustic emissions (DPOAEs).
Exposure to high levels of military or industrial noise may be associated with reductions in TEOAE and/or DPOAE amplitudes, even when audiometric results remain normal or less affected.[14,15,16,17,18] This suggests that OAEs may offer an early indicator of noise-induced cochlear damage before measurable hearing loss occurs. Military service members who had been exposed to noise and had normal hearing thresholds demonstrated lower TEOAE power and reduced TEOAE response bandwidth compared to military recruits who also had normal hearing thresholds but no history of noise exposure.[14] There were also significant differences in the presence and power of TEOAEs between those with audiometric thresholds of 0 dB HL or better and those with normal but slightly more elevated thresholds between 5 dB HL and 20 dB HL, suggesting that the reduction in TEOAEs may have indicated early cochlear damage that was also causing slightly elevated audiometric thresholds. Significant decreases in DPOAE and TEOAE amplitudes have also been found, with no change in audiometric thresholds, among US marine recruits who were exposed to impulse noise from firearms.[15] In another study, many participants with documented industrial or military noise exposure had absent TEOAEs and DPOAEs despite normal pure-tone hearing sensitivity.[16] Finally, among workers exposed to industrial noise, group-averaged TEOAEs and DPOAEs showed reduced amplitudes at more frequencies than behavioral audiometry, suggesting that the OAE measures may be more sensitive to noise-induced cochlear damage.[17,18]
Music exposure can also impact OAE results. After college students participated in the classroom jazz ensemble activity, there was a significant decrease in the amplitude of their TEOAEs as well as a significant temporary threshold shift at 4,000 Hz.[6] Following trumpet players’ solitary practice sessions, they experienced significant decreases in their DPOAE amplitudes and pure-tone thresholds.[8] Their DPOAE amplitudes recovered to within less than 1 dB of preexposure levels within 40-60 min after rehearsal. On the other hand, amateur brass musicians did not experience significant changes in DPOAE amplitudes pre- versus postrehearsal.[5] Among university marching band members, no abnormalities in TEOAE amplitudes were reported; however, TEOAEs were neither tested pre- versus postexposure nor were TEOAE amplitudes compared between the marching band members and a control group.[7]
It is clear that musicians and music students experience sound exposure levels that are potentially damaging.[4,5,6,7,8] Previous studies on college music students have found some short-term reductions in OAE amplitudes within a few minutes after practice sessions or ensemble activities[6,8] but there is lack of information on longstanding or permanent effects on OAEs for college music majors as compared to a control group. OAEs may be more sensitive to noise-induced cochlear damage than audiometry, at least for military noise and industrial noise[1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18] but there is lack of information about the effectiveness of OAEs for early detection of music-induced cochlear damage. If damage can be detected early by the use of OAEs, then steps could be taken to prevent further deterioration such as reducing the amount of harmful exposure or using hearing protection devices. The purpose of the present study was to determine if there was a difference in the presence versus absence of DPOAEs and/or DPOAE amplitudes in college music majors as compared to nonmusic majors. It was hypothesized that music majors would have more absent DPOAEs and reduced DPOAE amplitudes compared to nonmusic majors because of the music majors’ regular exposure to high sound levels.
Methods
Participants
Approval for this study was granted by the Institutional Review Board for the Protection of Human Subjects at the authors’ home institution. Twenty-eight music majors (10 males, 18 females) enrolled at a university and with age ranging 18-25 years (mean age: 20.7 years) participated in the study. These participants were recruited at a department meeting of all music majors, and via flyers posted in the music building. The goal was to recruit as many participants as possible and therefore, no attempt was made to recruit students of particular instruments or of any particular emphasis within the music major. A control group of 35 nonmusic majors (2 males, 33 females) of the same age range (18-25 years, with a mean age of 21.2 years) and enrolled at the same university during the same time period also participated in the study. The control group was recruited via flyers posted around the university, announcements made in several Communicative Disorders classes, and campus-wide email announcements. Due to the potential for females to have greater DPOAE amplitudes than males,[19,20] multiple attempts were made to recruit more male nonmusic majors campus-wide; however, these attempts were unsuccessful. The impact of the sex imbalance between the groups is further analyzed and discussed in the results and discussion sections.
Noise exposure questionnaire
A questionnaire (see next page) designed to assess each participant's noise exposure was given prior to testing. In addition, each participant was asked if he or she had experienced any recent music or nonmusic noise exposure. Participants were excluded from the study if their responses revealed recent high levels of noise exposure that may have caused a temporary threshold shift at the time of data collection. “Recent” was defined as within the previous 48 h or longer than 48 h if symptoms such as ringing in the ears, fullness, hearing loss, or any other subjective abnormal perceptions were still present. High levels of noise exposure were defined as: Use of firearms, attending a concert, listening to music/iPod/mp3 player at a level that caused ringing in the ears, or other comparable exposures. Music students’ data collection sessions were rescheduled if they had been playing or rehearsing within the previous hour, based on previous research that found that DPOAE amplitudes recovered within less than 1 dB of prerehearsal levels within that timeframe.[8] It was also not possible to allow a longer interval for the music students because of the many hours per week that they spent rehearsing. Music majors were also queried regarding their primary instrument, number of years they had been playing an instrument, and approximate total hours per week spent practicing individually and in ensembles, bands, and orchestras. None of them reported using hearing protection devices during rehearsals. All the participants were counseled on hearing protection, and all were given the option of purchasing universal or custom-fit standard or musician's earplugs at a discounted rate.
Equipment and procedures
All equipment was fully calibrated by a qualified technician within the previous year, and calibration checks on the tympanometer, audiometer, earphones, and DPOAE equipment were completed daily by the same trained investigator (the same investigator collecting the data) prior to each data collection session. The tympanometer probe was checked in the manufacturer-supplied 2.0 cm3 calibration cavity to ensure a correct volume reading of 2.0 cm3. Listening checks including checks of the investigator's known hearing thresholds were completed for the audiometer and earphone output levels and frequencies as well as the audiometer attenuator linearity. The investigator also checked her own known DPOAE levels bilaterally.
All testing was completed by the same investigator. Otoscopy was performed and cerumen removed, if necessary, before the testing began. Middle ear status was assessed immediately prior to DPOAE recording using the Grason-Stadler (GSI) TympStar or the Grason-Stadler (GSI) 33 version 2 middle ear analyzer. The equipment used depended on availability at the time of testing. Participants were excluded if any outer or middle ear abnormalities were detected. Middle ear status was considered normal if the tympanometry measures were within the following ranges: Peak admittance 0.30-1.80 mL, tympanometric peak pressure -110-25 daPa, and equivalent ear canal volume 0.8-2.10 mL. These values were adapted from the 90% ranges for 20-30-year old adults.[21]
Following the tympanometric measures, DPOAE and audiometric testing was completed bilaterally, always in that order, in a double-walled sound-attenuating booth. Participants were seated in a comfortable chair for all testing. The right ear was always tested first for consistency. DPOAEs were elicited using the GSI 60 DPOAE system, an f2/f1 ratio of 1.2, and f1 and f2 levels of 65 dB SPL and 55 dB SPL, respectively. The sampling rate was 16,000 Hz. A minimum of 30 frames and a maximum of 1,200 frames were collected per ear, and the noise rejection level was 20 dB SPL. DPOAEs were considered present when the amplitude of the emission was at least 6 dB above the noise floor at the corresponding frequency. DPOAEs corresponding to the frequency of 2f1-f2 were measured at three points per octave, and results were analyzed at the following f2 frequencies: 1,187 Hz, 1,500 Hz, 1,906 Hz, 2,531 Hz, 3,031 Hz, 3,812 Hz, 4,812 Hz, and 6,031 Hz. A probe check-fit procedure was completed prior to each measurement to ensure that the primary levels were within a tolerance of ±5 dB.
Questionnaire.
Participant Number
Answer the following questions as specifically as possible. Remember, you are not being judged on your responses so try to answer them as truthfully as possible.
-
Do you participate or have you participated in any of the following recreational activities (circle all that apply)?
- Gun hunting If yes, answer question 2
- Target shooting If yes, answer question 3
- iPod or MP3 use If yes, answer question 4-6
- Attend concerts
- Other activities or work with a high noise level. Specify the activity, and approximately how many hours per week you are exposed to the noise (mowing the lawn, working with power tools, etc):
-
When you gun hunt, do you wear hearing protection and if so, how often?
- Yes, all the time
- Yes, some of the time
- No, I do not wear hearing protection
-
When you target shoot, do you wear hearing protection and if so, how often?
- Yes, all the time
- Yes, some of the time
- No, I do not wear hearing protection
-
If you listen to your music on an iPod/MP3 player, how long do you typically listen for without taking a break (break = no listening for at least 5 min)?
- Less than 30 min
- 1-2 h
- 3-4 h
- Other
-
What is an appropriate statement regarding the volume level you listen to your iPod/MP3 player at?
- I can hear conversation around me with my music on.
- I cannot hear conversation around me with my music on.
-
When I am done listening to my iPod/MP3 player, are my ears ringing?
- Yes, every time
- Yes, sometimes
- Never
-
Do you suspect you might have a hearing loss?
- Yes
- No
Pure-tone air-conduction thresholds were obtained bilaterally using a modified Hughson-Westlake 10-down, 5-up procedure, according to the guidelines of the American Speech-Language-Hearing Association.[22] The Grason-Stadler (GSI) 61 clinical audiometer or the Madsen Orbiter 922 version 2 audiometer was used, depending on the availability at the time of testing, to obtain pure-tone thresholds. Insert earphones (ER-3A) were used to deliver the stimuli.
Thresholds were obtained at the pure-tone frequencies of .5 kHz, 1 kHz, 2 kHz, 3 kHz, 4 kHz, 6 kHz, and 8 kHz.
Results
Summary of statistical analyses
Chi-square tests were used to analyze whether the proportions of music majors and nonmusic majors differed significantly on categorical variables. Specifically, these variables included exhibiting an absent DPOAE for at least one frequency in at least one ear, and self-reported no-or low-risk noise exposure. A three-way mixed model analysis of variance (ANOVA) was completed to analyze DPOAE amplitudes. The between-subjects variable was music major versus nonmusic majors, and the within-subjects variables were ear and the DPOAE f2 frequency. Post hoc pair-wise comparisons using Bonferroni corrections for multiple comparisons were completed for f2 frequency, which was the only significant variable. Finally, 95% confidence intervals for the means (t distribution) were used to analyze the following at each frequency: Hearing threshold levels (audiograms) between music and nonmusic majors, DPOAE amplitudes (DP-grams) between music and nonmusic majors, DPOAE amplitudes between male and female music majors, and DPOAE amplitudes between brass and nonbrass music majors were measured. None of these differences reached statistical significance; however, the confidence intervals displayed general trends as well as the frequencies where significance was approached.
Questionnaire
The types of noise exposures reported by both the groups are shown in Table 1. The total percentages in each group exceeded 100% because many participants reported more than one type of exposure. The same majority of participants in each group (57.1%) reported “low-risk” iPod/mp3 use and attending concerts as their only noise exposure. “Low-risk” iPod/mp3 use was defined as listening to an iPod or mp3 player for 2 h or less at a time, and at a volume that allowed the listener to hear surrounding conversation, and such that the ears never rang after using the device. Low-risk iPod/mp3 use was reported as the only noise exposure by 2/28 (7.1%) of the music majors and by 6/35 (17.1%) of the nonmusic majors. No noise exposure was reported by only one music major and none of the nonmusic majors. Thus, a total of 3/28 (10.7%) of the music majors and 6/35 (17.1%) of the nonmusic majors reported either no noise exposure or only low-risk iPod/mp3 exposure, which was not a significant difference between the groups (Χ2 = 0.525, df = 1, p > .05). In addition, the percentages of participants reporting each type of noise exposure were similar between the music majors and the nonmusic majors.
Table 1.
Types of noise exposures reported
| Type of exposure | Music majors (%) | Nonmusic majors (%) |
|---|---|---|
| Firearm use (gun hunting or target shooting) without hearing protection | 2/28=7.1 | 2/35=5.7 |
| Firearm use with regular hearing protection | 2/28=7.1 | 0/35=0 |
| “Low-risk” iPod or mp3 use: Listening to iPod or mp3 player for 2 h or less at a time at a volume that does allow the listener to hear surrounding conversation and when ears never ring after using the device | 18/28=64.3 | 23/35=65.7 |
| Listening to iPod or mp3 player for 30 min or less at a time at a volume level that does not allow the listener to hear the surrounding conversation | 3/28=10.7 | 2/35=5.7 |
| Listening to iPod or mp3 player for 1-2 h at a time at a volume level that does not allow the listener to hear the surrounding conversation | 1/28=3.6 | 6/35=17.1 |
| Ears ring “sometimes” after using an iPod or mp3 device | 2/28=7.1 | 5/35=14.2 |
| Attend concerts | 23/28=82.1 | 25/35=71.4 |
| Other work or activity with high noise level | 2: Factory or mill work 3: Lawn mowing/yard work in summer 1: Loud video games |
4: Factory or mill work 4: Lawn mowing/yard work in summer |
| Total reporting no noise exposure | 1/28=3.5 | 0/35=0 |
| Total reporting low-risk iPod/mp3 use as the only noise exposure | 2/28=7.1 | 6/35=17.1 |
| Total reporting low-risk iPod/mp3 use and concerts as the only noise exposure | 16/28=57.1 | 20/35=57.1 |
The number of participants reporting various primary instruments as well as the self-reported number of years playing the instrument and number of hours practiced per week are shown in Table 2. When a given participant reported a range of years played or hours practiced, such as 8-9 or 15-20, the mean of that participant's range was used. Although the goal of the study was to recruit as many music majors as possible regardless of the primary instrument or emphasis within the major, woodwind and brass players were heavily represented (N = 14 and 10, respectively), and none of the music majors reported playing string instruments. In addition, two played percussion instruments, one played the piano, and one focused on voice. Table 2 also shows the totals and means for nonbrass compared to brass players because the DPOAE amplitudes were compared between these groups, and will be discussed below. Note that no differences were observed between the nonbrass and brass players in the number of years played (means of 10.6 years and 10.1 years, respectively) or in hours practiced per week (means of 13.6 h and 14 h, respectively).
Table 2.
Primary instruments, years playing, and number of hours practiced per week
| Primary instrument | Instrument family | Number of participants | Number of years playing instrument | Number of hours practiced per week | ||
|---|---|---|---|---|---|---|
| Mean | Range | Mean | Range | |||
| Clarinet | Woodwind | 8 (6 F, 2 M) | 11 | 5-19 | 17.6 | 10-30 |
| Flute | Woodwind | 4 (4 F) | 9.25 | 5-15 | 11.25 | 8-15 |
| Saxophone | Woodwind | 1 (1 M) | 13 | 13 | 18 | 18 |
| Bassoon | Woodwind | 1 (1 F) | 8.5 | 8.5 | 8 | 8 |
| Percussion | Percussion | 2 (2 M) | 11.8 | 8.5-15 | 14 | 3-25 |
| Piano | Percussion | 1 (1 M) | 16 | 16 | 5 | 5 |
| Voice | Voice | 1 (1 F) | 5 | 5 | 3.5 | 3.5 |
| Totals for non-brass instruments | 18 (12F, 6M) | 10.6 | 5-19 | 13.6 | 3.5-30 | |
| Trumpet | Brass | 5 (2 F, 3 M) | 9.4 | 7-13 | 15.8 | 7-40 |
| Trombone | Brass | 3 (3 F) | 12.2 | 7-15 | 11.7 | 4-16 |
| Euphonium | Brass | 2 (1 F, 1 M) | 8.5 | 7-10 | 13 | 12-14 |
| Totals for brass instruments | 10 (6F, 4M) | 10.1 | 7-15 | 14 | 4-40 | |
| Totals for all music majors | 28 | 10.4 | 5-19 | 13.9 | 3-40 | |
Audiometric thresholds
All of the participants in both the groups had normal (<25 dB HL) audiometric thresholds at all frequencies tested. Figures 1 and 2 show the mean thresholds and 95% confidence intervals for the means for each group in the right and left ears, respectively. Considerable overlap was observed between the confidence intervals at each frequency, indicating no significant differences in the thresholds between the groups. For the music majors, mean audiometric thresholds ranged 3.0-7.3 dB HL, depending on the ear and frequency and for the nonmusic majors, mean audiometric thresholds ranged 2.7-6.9 dB HL.
Figure 1.
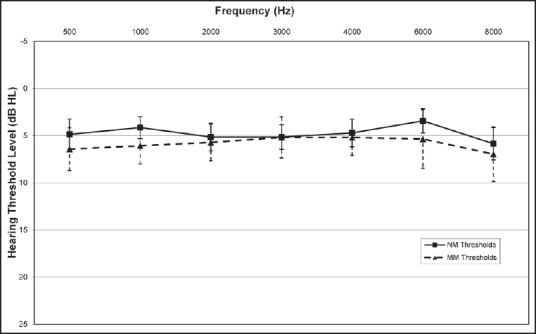
Mean audiometric thresholds for the right ears of the music majors (MM, n = 28) and nonmusic majors (NM, n = 35). Error bars indicate 95% confidence intervals of the means
Figure 2.
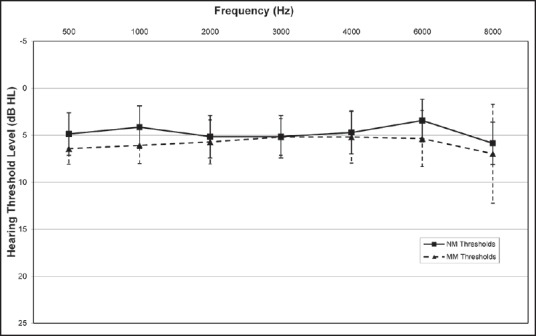
Mean audiometric thresholds for the left ears of the music majors (MM, n = 28) and nonmusic majors (NM, n = 35). Error bars indicate 95% confidence intervals of the means
Distortion product otoacoustic emissions
Six music majors (three males and three females) had an absent DPOAE for one or two frequencies in one ear, and one additional music major (female) had absent DPOAEs for at least one frequency in both ears. None of the nonmusic majors had absent DPOAEs at any frequency in either ear. The difference in the proportion of participants with absent DPOAEs between the two groups (7/28 music majors versus 0/35 nonmajors) was significantly greater than would be expected by chance (Χ2 = 9.84, df = 1, p < .005). Because the control group had a greater proportion of females (33/35) than the music major group (18/28), the absent DPOAEs were also analyzed in only the female participants. Four out of 18 female music majors had at least one absent DPOAE as compared to none of the 33 female nonmusic majors, and the difference between these proportions was also significant (Χ2 = 8.98, df = 1, p < .005).
Table 3 summarizes the characteristics of the music majors with at least one absent DPOAE. Although DPOAE absences occurred across the range of f2 frequencies, 6,031 Hz was the most common absent frequency, occurring in four out of seven participants. On an average, the participants with absent DPOAEs had played their instruments for 2.5 more years (mean of 12.9) than the entire group of music majors (mean of 10.4, from Table 2). They also reported practicing more hours per week (16.3), on an average, compared to all of the music majors (13.9, from Table 2); however, two of them practiced far fewer hours per week (3 h and 4 h), and one of them practiced quite a bit more (40 h), and so the mean value is not necessarily the best representation. The proportion of females in the group (4/7 or 57.1%) was similar to the proportion of females (18/28 or 64.3%) in the entire group of music majors. A variety of primary instruments were reported, with the proportion of instruments in each family similar to the proportion within the entire group of music majors. The other types of reported noise exposures within the absent DPOAE group were also comparable to the types and proportions reported within the entire group of music majors.
Table 3.
Characteristics of participants with at least one absent DPOAE
| Ear(s) | f2 frequency(ies) absent (Hz) | Primary instrument | Years playing instrument | Hours practiced per week | Sex | Other noise exposures reported |
|---|---|---|---|---|---|---|
| R | 3031 | Trombone | 13 | 4 | F | Low-risk iPod/mp3 use and attending concerts |
| R | 3,031, 6,031 | Drums | 15 | 3 | M | Ears ring following mp3 use |
| R | 1,500, 6,031 | Clarinet | 11 | 15 | F | Attending concerts |
| L | 6,031 | Clarinet | 19 | 25 | M | Firearm use without hearing protection, low-risk iPod/mp3 use, attending concerts |
| L | 1,187 | Flute | 15 | 11 | F | Low-risk iPod/mp3 use and attending concerts |
| L | 6,031 | Trumpet | 8.5 | 40 | M | Low-risk iPod/mp3 use, attending concerts, mowing the lawn |
| R & L | 1,187 (R & L) and 2,406 (R) | Bass trombone | 8.5 | 16 | F | Attending concerts |
| Means | 12.9 | 16.3 | ||||
| Total # of music majors | 7 | |||||
| Total # of nonmusic majors | 0 |
For the DPOAE amplitudes, a 3-way mixed model ANOVA was completed with major (music majors vs non-music majors) as the between-subjects variable, and ear and f2 frequency as within-subjects variables. The DPOAE amplitudes at the frequencies that did not meet the +6 dB SNR “presence” criteria (one to two frequencies for each of the seven participants) were included in the analysis at the amplitude that was measured since DPOAE amplitudes that were so low as to be “absent” were relevant to the analysis. See Table 4 for a summary of the ANOVA results for all main effects and interactions. The results indicated that the only statistically significant (p < .05) finding was for the main effect of f2 frequency; however, since this effect was similar for both the groups, it was not directly related to the purpose or hypothesis of this study. For general interest, the f2 frequencies with significantly different amplitudes (p < .05 with Bonferroni corrections for multiple comparisons) are shown in Table 5. In general, the DPOAE amplitudes at f2 frequencies of 1,500 Hz and 2531 Hz tended to be greater, and the amplitudes at 6,031 Hz tended to be lower than the amplitudes at many of the other f2 frequencies.
Table 4.
ANOVA results for DPOAE amplitudes
| Variable | F | df | p value |
|---|---|---|---|
| Major (music major MM vs nonmusic major NM) | .993 | 1, 61 | .323 |
| Frequency | 12.969 | 7, 427 | <.001 |
| Ear | .062 | 1, 61 | .804 |
| Major × Frequency | .838 | 7, 427 | .557 |
| Major × Ear | 1.543 | 1, 61 | .219 |
| Frequency × Ear | .407 | 7, 427 | .898 |
| Major × Frequency × Ear | .404 | 7, 427 | .900 |
Table 5.
Significant differences in DPOAE amplitudes between f2 frequencies
| f2 frequency (Hz) | 1,187 | 1,500 | 1,906 | 2,531 | 3,031 | 3,812 | 4,812 | 6,031 |
|---|---|---|---|---|---|---|---|---|
| 1,187 | ///////// | higher* | — | — | — | — | — | lower |
| 1,500 | ///////// | /////////// | lower | — | lower | lower | — | lower |
| 1,906 | ///////// | /////////// | /////////// | higher | — | — | — | lower |
| 2,531 | ///////// | /////////// | /////////// | /////////// | lower | lower | — | lower |
| 3,031 | ///////// | /////////// | /////////// | /////////// | /////////// | — | higher | — |
| 3,812 | ///////// | /////////// | /////////// | /////////// | /////////// | /////////// | — | higher |
| 4,812 | ///////// | /////////// | /////////// | /////////// | /////////// | /////////// | /////////// | lower |
| 6,031 | ///////// | /////////// | /////////// | /////////// | /////////// | /////////// | /////////// | /////////// |
*“Higher” and “lower” indicate the direction of significant (p < .05 with Bonferroni corrections) differences in amplitudes between the DPOAE at the f2 frequency in the top row versus the DPOAE at the f2 frequency in the left-hand column, e.g., the amplitude at 1,500 Hz was significantly higher than at 1,187 Hz
The mean DPOAE amplitudes and 95% confidence intervals (t distribution) for the means for the right and left ears of the two groups, music majors (MM) and nonmusic majors (NM), are shown in Figures 3 and 4, respectively. Again, the DPOAE data points that did not meet the +6 dB SNR “presence” criteria were recorded at the amplitude that was measured and included in these figures since DPOAE amplitudes that were so low as to be “absent” were relevant to the purpose and hypothesis of the study. (The figures were also created with the absent DPOAE points omitted but this did not result in any meaningful difference in the display or interpretation, and so they are not shown here). The differences in DPOAE amplitudes between the music majors and nonmusic majors were not statistically significant. In the right ear, however, the music majors’ amplitudes were 2-3 dB lower than the nonmusic majors’ amplitudes at the f2 frequencies of 3,031 Hz, 3,812 Hz, 4,812 Hz, and 6,031 Hz. Because of the greater proportion of males in the group of music majors, there was the possibility that these slightly lower DPOAE amplitudes in the right ear may have been due to a sex effect. Mean DPOAE amplitudes and 95% confidence intervals for the right ears of male and female music majors are shown in Figure 5. Of the f2 frequencies where music majors had slightly lower amplitudes than nonmusic majors (3,031 Hz, 3,812 Hz, 4,812 Hz, and 6,031 Hz), the male music majors had amplitudes 2-4 dB lower than the female music majors at 3,812 Hz, 4,812 Hz, and 6,031 Hz. The confidence intervals for the males and females overlapped, indicating that the difference between the sexes was not statistically significant. At 3,031 Hz, on the other hand, the amplitudes of male versus female music majors were nearly the same.
Figure 3.
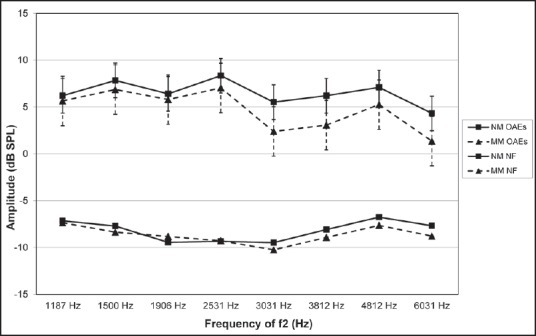
Mean DPOAE amplitudes for the right ears of music majors (MM, n = 28) and nonmusic majors (NM, n = 35), with corresponding noise floor values. Error bars indicate 95% confidence intervals of the means
Figure 4.
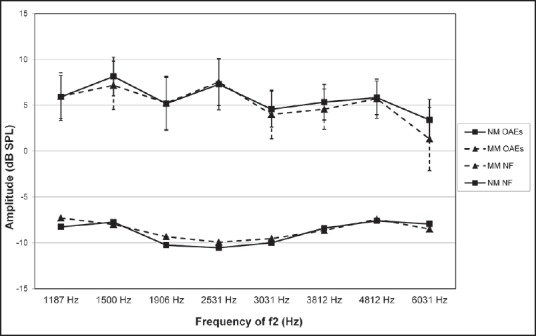
Mean DPOAE amplitudes for the left ears of music majors (MM, n = 28) and nonmusic majors (NM, n = 35), with corresponding noise floor values. Error bars indicate 95% confidence intervals of the means
Figure 5.
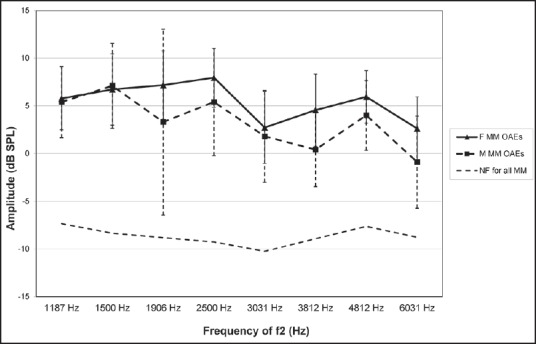
Mean DPOAE amplitudes for the right ears of female music majors (F MM, n = 18) and male music majors (M MM, n = 10), with mean noise floor values for all music majors. Error bars indicate 95% confidence intervals of the means
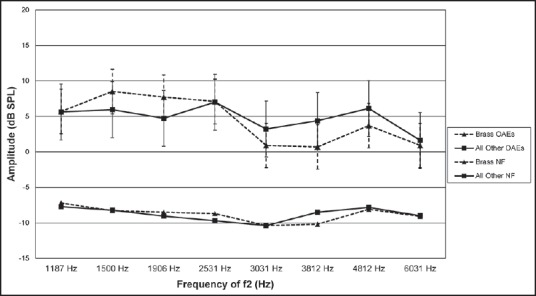
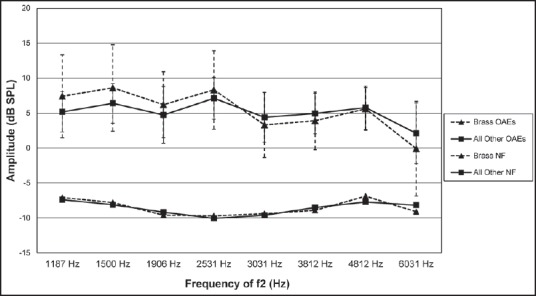
Although the goal of this study was to recruit as many music majors as possible regardless of primary instrument, brass and woodwind instruments were heavily represented, and none of the participants reported playing string instruments. Given the previous finding that brass players in an orchestra were exposed to slightly higher sound levels,[4] DPOAEs were examined between the brass and nonbrass players. Based on the data in Table 3, the proportion of brass players with at least one absent DPOAE was similar to the proportion of brass players in the entire group of music majors (3/7 or 42.9% of those with absent DPOAEs were brass players, as compared to 10/28 or 35.7% brass players in the entire group of music majors). Figures 6 and 7 show the mean DPOAE amplitudes and 95% confidence intervals (t distribution) for the right and left ears, respectively, for the brass players (N = 10; 6 females and 4 males) in comparison to players of all the other instruments (woodwind, percussion, and voice; N = 18; 12 females and 6 males). In the left ears, the mean amplitudes were similar between the groups at each frequency, and there was considerable overlap in the confidence intervals of the means. In the right ears, there were some differences in mean amplitudes between the brass and nonbrass groups but the confidence intervals still overlapped indicating no significant differences. At 3,031 Hz, 3,812 Hz, and 4,812 Hz, the DPOAE amplitudes of the brass players were 2-3 dB lower than the nonbrass players, and at 1,500 Hz and 1,906 Hz, the DPOAE amplitudes were 2-3 dB greater in the brass versus the nonbrass players.
Figure 6.
Mean DPOAE amplitudes for the right ears of music majors who play brass instruments (n = 10) and all other music majors (n = 18), with corresponding noise floor values. Error bars indicate 95% confidence intervals of the means
Figure 7.
Mean DPOAE amplitudes for the left ears of music majors who play brass instruments (n = 10) and all other music majors (n = 18), with corresponding noise floor values. Error bars indicate 95% confidence intervals of the means
Discussion
A significantly greater proportion of university music majors exhibited absent DPOAEs for at least one frequency in at least one ear, compared to nonmusic majors. Because the absent DPOAEs only occurred at one to two frequencies per ear for each participant, they did not represent widespread cochlear damage; however, they could have represented the early stages of cochlear damage. The DPOAEs were collected in a quiet, double-walled sound booth with cooperative participants, and so the measurements were not affected by the environment or the participants’ behavior. The absent DPOAEs were also unrelated to the sex of the participant because even when only females were included in the analysis, there were still significantly more music majors with absent DPOAEs compared to nonmusic majors. Self-reported noise exposure outside of studying music and primary instrument played were also unrelated to the absent DPOAEs.
Those with absent DPOAEs did, on an average, report playing their instruments for 2.5 years longer than the entire group of music majors, and so it is possible that the absent DPOAEs may have represented damage that was beginning to appear in those who had more years of music exposure. The group with absent DPOAEs also reported, on an average, practicing for 2.4 h per week longer than the entire group of music majors but this mean value was misleading due to the outliers on both ends (3-4 h for two participants, and 40 h for one). Participants were asked to approximate the average number of hours per week they currently spend practicing but it would have been useful to know how closely that value represented the hours they have practiced over a number of years. For example, it is possible that the participants reporting 3-4 h per week may have been more occupied with other responsibilities during the semester of data collection but may have practiced many more hours during previous semesters.
DPOAE amplitudes were 2-3 dB lower but not statistically significantly and so, 3,031-6,031 Hz in the right ears of music majors compared to the right ears of nonmusic majors. It is possible that this could have been due to early stages of cochlear damage in the music majors but it could also have been due to chance or to a normal sex effect since relatively more males were in the music major group than in the control group. At three of those frequencies (3,812 Hz, 4,812 Hz, and 6,031 Hz), the male music majors demonstrated DPOAE amplitudes that were 2-4 dB lower (not statistically significant) than the female music majors. At 3,031 Hz, there were no differences in amplitudes between male and female music majors, and the DPOAE amplitudes of the music majors were 3.1 dB lower than the amplitudes of the nonmusic majors.
Previous research on sex effects on DPOAE amplitudes in young adults has yielded mixed results, with some studies indicating greater amplitudes in females[19,20] and others indicating minimal to no differences between the sexes.[23,24] In one of the previous studies, equal-level primaries of 55 dB SPL and 75 dB SPL were used, and significantly greater amplitudes of 2-4 dB across f2 frequencies of approximately 2,000-6,000 Hz were found in one randomly selected ear of eight females compared to one randomly selected ear of eight males.[19] In another study that also used equal-level primaries (75 dB SPL), DPOAE amplitudes in both ears of females were 0.1-0.5 dB greater than in both the ears of males.[20] On the other hand, when the right ears of males and females were tested using f1 and f2 primary levels of 60 dB SPL and 45 dB SPL, respectively, DPOAE amplitudes were similar between males and females through 8 kHz, and greater for males at approximately 9-10 kHz.[23] Another study also found no significant differences in DPOAE amplitudes between the sexes at most frequencies, with the exception of greater amplitudes among females at an f2 of 2,000 Hz.[24] Equal-level primaries that varied 40-70 dB SPL were used in that study, and both ears were tested. Because DPOAE measurement parameters differed between all of the previous studies as well as between those studies and the current one, it is not possible to make direct comparisons or an overall conclusion about the effect of sex on DPOAE amplitudes. Despite the mixed results of previous and current research, however, there is some evidence of at least some degree of sex effect on DPOAE amplitudes.
Mean DPOAE amplitudes in the right ears of music majors who reported a primary instrument in the brass family (N = 10, 6 females and 4 males) differed but not significantly from the amplitudes in the right ears of music majors who reported a primary instrument in the woodwind, percussion, or voice family (N = 18, 12 females and 6 males). For the brass players, DPOAE amplitudes were 2-3 dB greater at 1,500 Hz and 1,906 Hz, and 2-3 dB lower at 3,031 Hz, 3,812 Hz, and 4,812 Hz than nonbrass players. These amplitude differences were not due to sex, differences in noise exposure, years playing the instrument, or hours practicing per week, as all of these variables were similar between the brass and nonbrass groups. It is possible that brass players may experience cochlear damage sooner than other instrumentalists, given the previous finding that brass players in an orchestra were most frequently exposed to sound levels approximately 3 dB greater than the most frequent exposure levels of woodwind and percussion players.[4] That same study neither found any difference in the hearing thresholds between the brass and nonbrass players nor did they find any difference in the interaural exposure levels or interaural thresholds among the musicians in either group. They did not measure OAEs. In recruiting participants for the current study, the goal was to include as many music majors as possible without regard for the instrument played; however, it may be helpful for future research to include a larger sample of participants from each instrument family in order to more definitively determine if some instrumentalists are at a greater risk of cochlear damage than others. If certain instrumentalists are more vulnerable to hearing damage, then those musicians or music students could be monitored more closely and/or stronger hearing conservation efforts could be directed toward them.
One method that could potentially help elucidate whether differences in cochlear function exist between music and nonmusic majors or between certain subgroups of music majors is the DPOAE input/output (i/o) function. DPOAE i/o functions display the amplitude of the 2f1-f2 DPOAE as a function of the level of one of the primaries.[25,26,27] The shape of these functions mimics the shape of the i/o function of the basilar membrane; when cochlear function is normal, the i/o functions are more linear at low input levels, compressive at moderate input levels, and linear to expansive at higher input levels.[25,26] When auditory thresholds are elevated to even a slight degree (e.g., 20-25 dB HL), the DPOAE i/o function is also altered, displaying elevated DPOAE thresholds and a more linear and less compressive response at the moderate input levels.[26,27] Additionally, when DPOAE i/o functions were measured at 3 kHz in humans following exposure to narrowband noise, the DPOAE response was reduced for the lower input levels.[28] Thus, DPOAE i/o functions could potentially be used in future research to further explore whether differences in cochlear function exist between music and nonmusic majors or between particular subgroups of music majors.
In contrast to previous research that focused on OAEs in college music students within several minutes after music exposure, the current study attempted to measure more longstanding effects on hearing thresholds and/or DPOAEs in comparison to a control group. It has previously been found that specific sessions of music exposure led to reductions in college music students’ OAE amplitudes when measured within 2-10 min after the exposure.[6,8] In another previous study, however, no abnormalities in TEOAE amplitudes were found among university marching band members.[7] None of these previous studies included a control group to determine whether the music students’ OAEs differed from those of nonmusic students. In contrast, the current study excluded participants with such recent music exposure and included a control group, and found significantly more absent DPOAEs as well as some nonsignificantly lower DPOAE amplitudes in music majors compared to nonmusic majors.
Sound exposure levels of the music majors were not measured in the current study since previous research has established that musicians and music majors do experience harmful exposure levels.[4,5,6,7,8] Furthermore, the goal of this study was to evaluate whether music majors, on an average, had evidence of reduced cochlear function due to their cumulative exposure over time rather than to measure the levels of specific instances of exposure. It is obviously difficult, and perhaps even impossible, to accurately measure cumulative exposure over a period of many years or even over months. The previous research has focused on measuring clearly defined, limited instances of exposure, most likely due to the practical difficulties involved in measuring the variety of cumulative exposures. Nevertheless, it may be useful to attempt to measure cumulative exposure on a more limited basis such as total weekly exposures of music students and to determine whether these exposure levels are correlated to any differences in OAE amplitudes.
One limitation of the current study was its reliance on participants’ self-report of exposure to potentially hazardous noise levels that were unrelated to being a music major; however, it is impossible to truly accurately measure these noise exposures over months or years. The noise questionnaire was designed to ask specific and clearly defined questions about the common types of exposures among 18-25-year-olds in the geographic area of the study. An open-ended question about “other” exposures was also included, with some possible examples given to help participants understand and recollect other potentially hazardous noise exposures. Similar proportions of music majors and nonmusic majors reported similar types of noise exposures (unrelated to the activities of being a music major), which suggests that noise exposure was not a confounding variable in the differences between the two groups. There is still a possibility, however, that certain participants could have remembered and reported noise exposures more or less accurately than other participants.
Given the greater prevalence of absent DPOAEs in university music majors compared to nonmusic majors, it appears that the early stages of cochlear damage may be occurring in the music majors. Additional research is needed, preferably across multiple colleges/universities to maximize generalizability to further explore early indications of cochlear damage in music majors. Ideally, this research would be longitudinal in order to more definitively determine when the music students begin to exhibit any signs of cochlear damage. It would also be beneficial to identify whether any particular subgroups of music majors, such as those playing instruments from particular families, are at a greater risk of earlier cochlear damage. If longitudinal changes in DPOAEs are observed for music majors or particular subgroups of music majors, it may provide extra motivation for them to utilize hearing protection devices in order to prevent additional, and likely more noticeable, damage.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Atlanta (GA): National Institute for Occupational Safety and Health; 1998. [Last accessed on 2015 Sep 03]. Criteria for a Recommended Standard: Occupational Noise Exposure (DHHS Publication No. 98-126) Available from: http://www.cdc.gov/niosh/docs/98-126/ [Google Scholar]
- 2.Geneva,Switzerland: World Health Organization; 2015. [Last accessed on 2015 Sep 10]. Hearing Loss Due to Recreational Exposure to Loud Sounds: A Review. Available from: http://apps.who.int/iris/bitstream/10665/154589/1/9789241508513_engpdfua=1&ua=1 . [Google Scholar]
- 3.Geneva, Switzerland: World Health Organization; 2004. [Last accessed on 2015 Sep 10]. Occupational Noise: Assessing the Burden of Disease from Work-Related Hearing Impairment At National and Local Levels. Available from: http://www.who.int/quantifying_ehimpacts/publications/en/ebd9.pdf . [Google Scholar]
- 4.Royster JD, Royster LH, Killion MC. Sound exposures and hearing thresholds of symphony orchestra musicians. J Acoust Soc Am. 1991;89:2793–803. doi: 10.1121/1.400719. [DOI] [PubMed] [Google Scholar]
- 5.Møllerløkken OJ, Magerøy N, Bråtveit M, Lind O, Moen BE. Forte fortissimo for amateur musicians: No effect on otoacoustic emissions. Med Probl Perform Art. 2013;28:3–8. [PubMed] [Google Scholar]
- 6.Gopal KV, Chesky K, Beschoner EA, Nelson PD, Stewart BJ. Auditory risk assessment of college music students in jazz band-based instructional activity. Noise Health. 2013;15:246–52. doi: 10.4103/1463-1741.113520. [DOI] [PubMed] [Google Scholar]
- 7.Jin SH, Nelson PB, Schlauch RS, Carney E. Hearing conservation program for marching band members: A risk for noise-induced hearing loss? Am J Audiol. 2013;22:26–39. doi: 10.1044/1059-0889(2012/11-0030). [DOI] [PubMed] [Google Scholar]
- 8.Poissant SF, Freyman RL, MacDonald AJ, Nunes HA. Characteristics of noise exposure during solitary trumpet playing: Immediate impact on distortion-product otoacoustic emissions and long-term implications for hearing. Ear Hear. 2012;33:543–553. doi: 10.1097/AUD.0b013e31824c0935. [DOI] [PubMed] [Google Scholar]
- 9.Lapsley Miller JA, Marshall L, Heller LM. A longitudinal study of changes in evoked otoacoustic emissions and pure-tone thresholds as measured in a hearing conservation program. Int J Audiol. 2004;43:307–22. doi: 10.1080/14992020400050040. [DOI] [PubMed] [Google Scholar]
- 10.Prieve BA, Fitzgerald TS. Otoacoustic emissions. In: Katz J, Chasin M, English K, Hood LJ, Tillery KL, editors. Handbook of Clinical Audiology. 7th ed. Philadelphia: Wolters Kluwer Health; 2015. pp. 357–79. [Google Scholar]
- 11.Lonsbury-Martin BL, Whitehead ML, Martin GK. Clinical applications of otoacoustic emissions. J Speech Hear Res. 1991;34:964–81. doi: 10.1044/jshr.3405.964. [DOI] [PubMed] [Google Scholar]
- 12.Ceranic B. The value of otoacoustic emissions in the investigation of noise damage. Audiol Med. 2007;5:10–24. [Google Scholar]
- 13.Lonsbury-Martin BL, Martin GK. Distortion-product otoacoustic emissions in populations with normal hearing sensitivity. In: Robinette M, Glattke T, editors. Otoacoustic Emissions: Clinical Applications. 3rd ed. New York: Thieme Medical Publishers; 2007. pp. 107–30. [Google Scholar]
- 14.Attias J, Furst M, Furman V, Reshef I, Horowitz G, Bresloff I. Noise-induced otoacoustic emission loss with or without hearing loss. Ear Hear. 1995;16:612–8. doi: 10.1097/00003446-199512000-00007. [DOI] [PubMed] [Google Scholar]
- 15.Marshall L, Lapsley Miller JA, Heller LM, Wolgemuth KS, Hughes LM, Smith SD, et al. Detecting incipient inner-ear damage from impulse noise with otoacoustic emissions. J Acoust Soc Am. 2008;125:995–1013. doi: 10.1121/1.3050304. [DOI] [PubMed] [Google Scholar]
- 16.Attias J, Horovitz G, El-Hatib N, Nageris B. Detection and clinical diagnosis of noise-induced hearing loss by otoacoustic emissions. Noise Health. 2001;3:19–31. [PubMed] [Google Scholar]
- 17.Helleman HW, Jansen EJ, Dreschler WA. Otoacoustic emissions in a hearing conservation program: General applicability in longitudinal monitoring and the relation to changes in pure-tone thresholds. Int J Audiol. 2010;49:410–9. doi: 10.3109/14992020903527616. [DOI] [PubMed] [Google Scholar]
- 18.Korres GS, Balatsouras DG, Tzagaroulakis A, Kandiloros D, Ferekidou E, Korres S. Distortion product otoacoustic emissions in an industrial setting. Noise Health. 2009;11:103–10. doi: 10.4103/1463-1741.50695. [DOI] [PubMed] [Google Scholar]
- 19.Cacace AT, McClelland WA, Weiner J, McFarland DJ. Individual differences and the reliability of 2F1-F2 distortion-product otoacoustic emissions: Effects of time-of-day, stimulus variables, and gender. J Speech Hear Res. 1996;39:1138–48. doi: 10.1044/jshr.3906.1138. [DOI] [PubMed] [Google Scholar]
- 20.McFadden D, Martin GK, Stagner BB, Maloney MM. Sex differences in distortion-product and transient-evoked otoacoustic emissions compared. J Acoust Soc Am. 2009;125:239–46. doi: 10.1121/1.3037231. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Roup CM, Wiley TL, Safady SH, Stoppenbach DT. Tympanometric screening norms for adults. Am J Audiol. 1998;7:55–60. doi: 10.1044/1059-0889(1998/014). [DOI] [PubMed] [Google Scholar]
- 22.Rockville, MD: The American Speech-Language-Hearing Association; 2005. [Last accessed on 2015 Sep 03]. Guidelines for Manual Pure-Tone Threshold Audiometry. Available from: http://www.asha.org/policy/GL2005-00014.htm . [Google Scholar]
- 23.Dunckley KT, Dreisbach LE. Gender effects on high frequency distortion product otoacoustic emissions in humans. Ear Hear. 2004;25:554–64. doi: 10.1097/00003446-200412000-00004. [DOI] [PubMed] [Google Scholar]
- 24.Moulin A, Collet L, Veuillet E, Morgon A. Interrelations between transiently evoked otoacoustic emissions, spontaneous otoacoustic emissions and acoustic distortion products in normally hearing subjects. Hear Res. 1993;65:216–33. doi: 10.1016/0378-5955(93)90215-m. [DOI] [PubMed] [Google Scholar]
- 25.Bhagat SP. Modeling DPOAE input/output function compression: Comparisons with hearing thresholds. J Am Acad Audiol. 2014;25:746–59. doi: 10.3766/jaaa.25.8.5. [DOI] [PubMed] [Google Scholar]
- 26.Dorn PA, Konrad-Martin D, Neely ST, Keefe DH, Cyr E, Gorga MP. Distortion product otoacoustic emission input/output functions in normal-hearing and hearing-impaired human ears. J Acoust Soc Am. 2001;110:3119–31. doi: 10.1121/1.1417524. [DOI] [PubMed] [Google Scholar]
- 27.Neely ST, Johnson TA, Kopun J, Dierking DM, Gorga MP. Distortion product otoacoustic emission input/output characteristics in normal-hearing and hearing-impaired human ears. J Acoust Soc Am. 2009;126:728–738. doi: 10.1121/1.3158859. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Engdahl B, Kemp DT. The effect of noise exposure on the details of distortion product otoacoustic emissions in humans. J Acoust Soc Am. 1996;99:1573–87. doi: 10.1121/1.414733. [DOI] [PubMed] [Google Scholar]