

Abstract
Background:
Preeclampsia in pregnancy has been shown to be associated with low serum calcium level. Though the evidence is abundant, it is equivocal.
Objectives:
The study aimed to estimate the dietary calcium intake and serum calcium status among pregnant women, and to document the association of the dietary calcium intake and serum calcium status with incidence of preeclampsia in the 3rd trimester of pregnancy.
Materials and Methods:
A community-based cross-sectional study was conducted in the Health and Demographic Surveillance System (HDSS) site, Ballabgarh, Haryana, India. All pregnant women between 28 weeks and 36 weeks of gestation were interviewed. A semi-structured interview schedule and a 24-h dietary recall questionnaire were administered to assess the dietary calcium intake. AutoAnalyser (Biolis 24i) was used for measuring serum calcium.
Results:
We enrolled 217 pregnant women. The mean [standard deviation (SD)] dietary calcium intake was 858 (377) mg/day. The mean (SD) serum calcium level was 9.6 mg/dL (0.56). Incidence of preeclampsia was 13.4%. Preeclampsia was not associated with hypocalcemia [odds ratio (OR) = 1.2 95% confidence interval (CI); 0.27-3.98].
Conclusion:
The majority of pregnant women had inadequate dietary calcium intake. The prevalence of hypocalcemia was low. Low serum calcium level was not associated with preeclampsia. Calcium supplementation may not reduce preeclampsia in this population.
Keywords: Dietary calcium intake, pregnancy, preeclampsia, rural, serum calcium
Introduction
Ninety nine percent of the total body calcium is in the bones and the remaining 1% is in the extracellular space. The recommended dietary allowance (RDA) is 1,200 mg/day for pregnant women.(1) Pregnancy is a state of increased demand for calcium, which should be met. Calcium homeostasis is finely regulated by a complex mechanism coordinated by a variety of hormones, the chief among them being vitamin D and parathyroid hormone. However, serum calcium levels have been shown to be consistently low among pregnant women.(2,3,4,5) The most important component of the regulation cycle is dietary calcium intake. So supplementing calcium in pregnancy may result in an elevation of the serum calcium level. Several complications during pregnancy have been attributed to the lower level of calcium. They include both maternal complications such as preeclampsia and poor bone formation in the mother, and fetal complications such as low birth weight, increased neonatal mortality, and high blood pressure in the child.(2,5)
Some studies showed no effect of the serum calcium level on preeclampsia(2,6,7) while other studies showed an association of serum calcium level with preeclampsia.(8,9,10,11,12) There is limited evidence from community-based studies of rural India for serum calcium level and the incidence of preeclampsia. Therefore, the study aimed to estimate the dietary calcium intake and serum calcium status among pregnant women and to document the association between serum calcium and preeclampsia in the third trimester of pregnancy.
Materials and Methods
This community-based cross-sectional survey was conducted (from November 2012 to December 2013) at the Ballabgarh Health and Demographic Surveillance System (HDSS), which is managed by Centre for Community Medicine (CCM), All India Institute of Medical Sciences (AIIMS), New Delhi, Delhi, India. It is situated in Ballabgarh block of Faridabad district, Haryana, India. The Ballabgarh HDSS has two primary health centres (PHC) and one subdistrict hospital at Ballabgarh, Haryana, India. A detailed description of Ballabgarh HDSS is available in one of our recent publications.(13) Ethical approval was obtained from the Ethics Committee of the AIIMS, New Delhi, Delhi, India, vide their letter reference no. IESC/T-420/02/11/2012 dated November 8, 2012. All registered pregnant women with a period of gestation of more than 28 weeks were eligible for inclusion in the study. Pregnant women with known history of hypertension before 20 weeks of gestation were excluded.
We assumed the prevalence of dietary calcium insufficiency to be 66% based on the study of Darwish et al.(3) Based on relative precision of 10% and alpha error of 0.05, the required sample size was 210. Assuming a response rate of 90%, the total sample size required was 235. All pregnant women in study area were included. A total of 217 pregnant women were enrolled.
All eligible pregnant women were contacted through home visits. Dietary intake was assessed by 24-h dietary recall method. Dietary calcium intake was calculated by applying the Indian Council of Medical Research (ICMR) standard nutritive value of Indian food(14) to the dietary history. Blood of 3 mL from the antecubital vein was drawn without the use of a tourniquet, under aseptic conditions. The blood was stored in previously labeled polypropylene tubes and allowed to clot spontaneously. Centrifugation at 60 rpm for 2 min was performed. Serum calcium was measured with the enzymatic method using automated spectrophotometer (Biolis 24i manufactured by Carolina Liquid Chemistries Corporation, Winston-Salem, North Carolina, United States of America). The 24-h dietary recall method was repeated on the second day and the blood report was handed over to the participant.
Blood pressure was measured at the first visit using a manual pneumatic sphygmomanometer (Industrial Electronic & Allied Products, Pune, Maharashtra, India), with the pregnant women sitting comfortably as recommended by the British Hypertension Society and the Nurses Hypertension Association. A clean-catch urine sample was tested by dipstick at the first visit for albuminuria.(15) Preeclampsia was defined as a systolic blood pressure higher than 140 mmHg and a diastolic blood pressure higher than 90 mmHg on two occasions at least 4 h apart after 20 weeks of pregnancy in a woman with previously normal blood pressure, along with proteinuria [defined as N300 mg/24 h or ≥1+ (on a clean-catch dipstick in the absence of urinary infection)].(16)
The data were entered on Epi Info version 3.5.4 (Centers for Disease Control and Prevention, Atlanta, USA). The data were then transferred to Microsoft Excel 2010. Data cleaning was done in Microsoft Excel 2010. Analysis was done in Stata 11 (StataCorp, College Station, Texas, USA). The results of descriptive analysis are presented as proportions with 95% confidence intervals (CIs) or as mean [standard deviation (SD)] wherever applicable.
Results
Sociodemographic characteristics of the participants
Through the Health Management Information System, we generated a list of 217 pregnant women who were eligible to participate in the study. All the women participated in the study. About 38.8% of the pregnant women were 21 years or below in age. Out of 217 pregnant women, 97.3% were homemakers. One-fourth pregnant women had studied till high school and the same proportion had studied till middle school [Table 1]. The mean height (SD) was 154.7 cm (6.31) and mean weight (SD) was 57.5 kg (8.1). Out of the 217 pregnant women, 76 (35%) were primigravida.
Table 1.
Distribution of pregnant women by sociodemographic status

Dietary calcium intake and serum calcium level
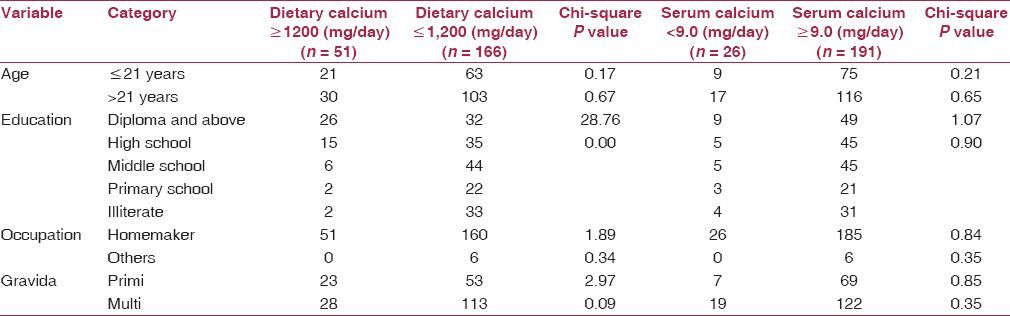
A total of 51 (23.5%) pregnant women had dietary calcium intake more than or equal to the recommended value (RDA = 1,200 mg). The mean dietary calcium intake (SD) was 858.4 (377.0) mg/day against RDA of 1,200 mg/day. However, 191 (88%) pregnant women had serum calcium level of more than 9 mg/dL. The mean serum calcium level (SD) was 9.6 (0.56) mg/dL against the normal level of 9.0 mg/dL [Table 2]. On bivariate analysis, dietary calcium intake was associated with education (P value <0.01, Table 3).
Table 2.
Distribution of pregnant women by serum calcium level and dietary calcium intake
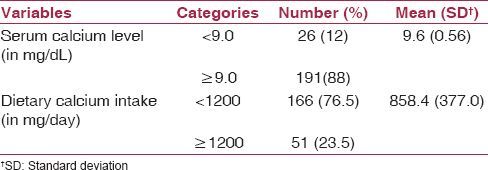
Table 3.
Distribution of serum calcium level and dietary calcium intake among pregnant women by various variables
Association of preeclampsia with serum calcium level and dietary calcium intake
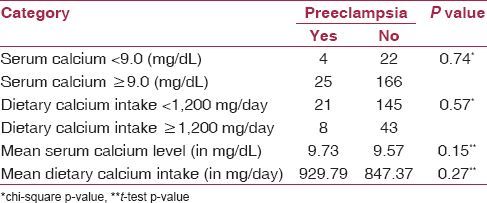
A total of 29 (13.4%) pregnant women developed preeclampsia. Serum calcium level was not associated with preeclampsia, odds ratio (OR) 1.2 (95% CI 0.27-3.98). There was no significant difference in the mean serum calcium level between those who developed preeclampsia and those who did not [Table 4].
Table 4.
Distribution of preeclampsia among pregnant women by serum calcium level and dietary calcium intake
Discussion
This study provided information about the dietary calcium intake and serum calcium level and its association with preeclampsia among pregnant women in a community setting. There were no teenage pregnancies, which is an independent risk factor for preeclampsia. The mean dietary calcium intake was 858.4 mg/day with SD of 377 mg/day. The mean dietary intake was lower than the RDA of 1,200 mg/day.
The mean serum calcium level was 9.6 mg/dL with SD of 0.56 mg/dL. The mean serum calcium level was near the normal value of 9 mg/dL.(17) Other studies had reported a lower level of mean serum calcium.(2,3,4,18,19,20) The reported lower level of serum calcium level could be explained by the fact that these studies were conducted in a hospital setting. Hence, the pregnant women were more likely to have deranged biochemical parameters. Kumar et al.(2) reported that the urban pregnant women were less exposed to sunlight. Rural women working outdoors are more likely to be exposed to sunlight for a longer period of time. Though most of the pregnant women in our study were homemakers, they also worked outside the confines of the house. Thus, they were likely to have received greater exposure to sunlight resulting in increased vitamin D production. This increase in vitamin D could lead to increase in serum calcium level. High phyate content in the diet hinders the absorption of calcium in the diet. We did not measure the phyate content of the diet. Hence, we are unable to comment on the role of dietary phyates on the findings related to serum calcium level.
The dietary calcium intake was not related to serum calcium level in the pregnant woman. It is therefore, possible that there are factors other than dietary intake that regulate the serum calcium level. Therefore, simply increasing dietary calcium intake during pregnancy may not necessarily result in an increase in the serum calcium level.
The incidence of preeclampsia in the third trimester in pregnant women was 13.4%. There was no significant association between serum calcium level and the occurrence of preeclampsia in our study. However, many studies(6,7,8,9,10,11,12) have shown an association of preeclampsia with low serum calcium levels. Preeclampsia etiology is complex and depends on a number of factors. It has been shown that the main risk factor for preeclampsia is chronic hypertension. In our study, none of the pregnant women were diagnosed with chronic hypertension. Other studies were hospital-based and the severity of preeclampsia was likely to be higher in pregnant women visiting a hospital than those diagnosed in the community. The overall incidence of preeclampsia could have been underestimated in our study because we had visited the pregnant women only once between 28 weeks and 36 weeks. There was a possibility of the pregnant women developing preeclampsia after the visit. We made a concurrent measurement of the serum calcium level and incidence of preeclampsia at the time of the visit. Therefore, the findings are valid at the time of measurement. However, it is possible that some more pregnant women might have developed preeclampsia later on, which was not recorded. We had collected the serum for estimating the calcium level among pregnant women with 28-36 weeks of gestation. Other studies had estimated the serum calcium level at the time of delivery. It has been shown that serum calcium level decreases with increasing months of gestation.(21) Therefore, the serum calcium level would be lower at the time of delivery as compared to the level at 28-36 weeks of gestation. Therefore, a lower level of serum calcium and the occurrence of preeclampsia were concomitant and might not be etiologically associated. Other studies had recruited patients who were diagnosed cases of preeclampsia. The time of onset of preeclampsia was not known. So it cannot be inferred that a low level of calcium in the serum leads to preeclampsia.
There was no statistically significant association between dietary calcium intake and preeclampsia. It is hypothesized that low calcium intake may cause high blood pressure by stimulating the release of parathyroid hormone and/or renin, thereby increasing intracellular calcium concentration in vascular smooth muscle cells and causing vasoconstriction.(22) A possible explanation for the mode of action of calcium supplementation is that it reduces parathyroid calcium release and intracellular calcium concentration, thereby reducing smooth muscle contractility and promoting vasodilatation.(23) But all these effects are exerted by the serum calcium level, which we have shown is independent of the dietary calcium intake. Thus, calcium supplementation is unlikely to have an effect on the incidence of preeclampsia. The dietary calcium intake only replenishes the stores and the serum calcium levels are maintained in a tight range. Knowledge regarding calcium intake and serum calcium level in community settings can help us better frame the policies and guidelines regarding calcium supplementation.
Ours was a community-based study; therefore, extrapolation of results to the community can be made. Adequate sample size and high participation rate (100%) give us confidence about the validity of the study findings. All the samples were tested in one laboratory, which was housed in a reputed medical institution. Interobserver variation was avoided since the data were collected by a single investigator. The overall incidence of preeclampsia could have been underestimated in our study because we had visited the pregnant women only once between 28 weeks and 36 weeks. There was a possibility of the pregnant women developing preeclampsia after the visit.
In conclusion, the mean dietary calcium intake of pregnant women residing in the rural part of North India was less than the RDA. The serum calcium level was however, normal. Thus, even though the dietary calcium intake was low, the serum calcium level was normal. The incidence of preeclampsia was not associated with serum calcium level. Calcium supplementation may not reduce preeclampsia in this population. We feel that a larger study with a multicentric site is needed to document the serum calcium level among pregnant women residing in the rural areas of India.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Peacock M. Calcium metabolism in health and diseases. Clin J Am Soc Nephrol. 2010;5(Suppl 1):S23–30. doi: 10.2215/CJN.05910809. [DOI] [PubMed] [Google Scholar]
- 2.Kumar A, Agarwal K, Devi SG, Gupta RK, Batra S. Hypocalcemia in pregnant women. Biol Trace Elem Res. 2010;136:26–32. doi: 10.1007/s12011-009-8523-6. [DOI] [PubMed] [Google Scholar]
- 3.Darwish AM, Mohamad SN, Gamal Al-Din HR, Elsayed YA, Ahmad SI. Prevalence and predictors of deficient dietary calcium intake during the third trimester of pregnancy: The experience of a developing country. J Obstet Gynaecol Res. 2009;35:106–12. doi: 10.1111/j.1447-0756.2008.00879.x. [DOI] [PubMed] [Google Scholar]
- 4.Bhalala U, Desai M, Parekh P, Mokal R, Chheda B. Subclinical hypovitaminosis D among exclusively breastfed young infants. Indian Pediatr. 2007;44:897–901. [PubMed] [Google Scholar]
- 5.Sachan A, Gupta R, Das V, Agarwal A, Awasthi PK, Bhatia V. High prevalence of vitamin D deficiency among pregnant women and their newborns in northern India. Am J Clin Nutr. 2005;81:1060–4. doi: 10.1093/ajcn/81.5.1060. [DOI] [PubMed] [Google Scholar]
- 6.Punthumapol C, Kittichotpanich B. Serum calcium, magnesium and uric acid in preeclampsia and normal pregnancy. J Med Assoc Thai. 2008;91:968–73. [PubMed] [Google Scholar]
- 7.Jafrin W, Paul SK, Sultana S, Rabeya S, Hoque MR, Muttalib MA. Serum calcium level among normal pregnant and pre-eclamptic women in a sub urban area of Bangladesh. Mymensingh Med J. 2013;22:418–22. [PubMed] [Google Scholar]
- 8.Sukonpan K, Phupong V. Serum calcium and serum magnesium in normal and preeclamptic pregnancy. Arch Gynecol Obstet. 2005;273:12–6. doi: 10.1007/s00404-004-0672-4. [DOI] [PubMed] [Google Scholar]
- 9.Mohieldein AH, Dokem AA, Osman YH, Idris HM. Serum calcium levels as a marker of pregnancy-induced hypertension. Sudan J Med Sci. 2007;2:245–8. [Google Scholar]
- 10.Kim J, Kim YJ, Lee R, Moon JH, Jo I. Serum levels of zinc, calcium, and iron are associated with the risk of preeclampsia in pregnant women. Nutr Res. 2012;32:764–9. doi: 10.1016/j.nutres.2012.09.007. [DOI] [PubMed] [Google Scholar]
- 11.Jain S, Sharma P, Kulshreshtha S, Mohan G, Singh S. The role of calcium, magnesium, and zinc in pre-eclampsia. Biol Trace Elem Res. 2010;133:162–70. doi: 10.1007/s12011-009-8423-9. [DOI] [PubMed] [Google Scholar]
- 12.Patel A, Singh B, Patel A, Sharma M. Serum calcium level in pregnancy induced hypertension. Int J Biol Med Res. 2012;3:1914–8. [Google Scholar]
- 13.Kant S, Misra P, Gupta S, Goswami K, Krishnan A, Nongkynrih B, et al. The Ballabgarh Health and Demographic Surveillance System (CRHSP-AIIMS) Int J Epidemiol. 2013;42:758–68. doi: 10.1093/ije/dyt055. [DOI] [PubMed] [Google Scholar]
- 14.Gopalan C, Rama Sastri BV, Balasubramanian SC. Nutritive Value of Indian foods. Hyderabad, India: National Institute of Nutrition, Indian Council of Medical Research; 2004. pp. 47–58. [Google Scholar]
- 15.Report of the National High Blood Pressure Education Program Working Group on High Blood Pressure in Pregnancy. Am J Obstet Gynecol. 2000;183:S1–22. [PubMed] [Google Scholar]
- 16.ACOG Committee on Practice Bulletins — Obstetrics. ACOG practice bulletin. Diagnosis and management of preeclampsia and eclampsia. Number 33, January 2002. Obstet Gynecol. 2002;99:159–67. doi: 10.1016/s0029-7844(01)01747-1. [DOI] [PubMed] [Google Scholar]
- 17.Murphy E, Williams GR. Hypocalcemia. Medicine. 2009;37:465–8. [Google Scholar]
- 18.Hassan TJ, Ibrahim K, Jafarey SN. Dietary and serum calcium in pregnant women. J Pak Med Assoc. 1991;41:278–9. [PubMed] [Google Scholar]
- 19.Sanchez PA, Idrisa A, Bobzom DN, Airede A, Hollis BW, Liston DE, et al. Calcium and vitamin D status of pregnant teenagers in Maiduguri, Nigeria. J Natl Med Assoc. 1997;89:805–11. [PMC free article] [PubMed] [Google Scholar]
- 20.Tabrizi FM, Pakdel FG. Serum level of some minerals during three trimesters of pregnancy in Iranian women and their newborns: A longitudinal study. Indian J Clin Biochem. 2014;29:174–80. doi: 10.1007/s12291-013-0336-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Kumar A, Devi SG, Batra S, Singh C, Shukla DK. Calcium supplementation for the prevention of pre-eclampsia. Int J Gynaecol Obstet. 2009;104:32–6. doi: 10.1016/j.ijgo.2008.08.027. [DOI] [PubMed] [Google Scholar]
- 22.Belizan JM, Villar J, Repke J. The relationship between calcium intake and pregnancy-induced hypertension: Up-to-date evidence. Am J Obstet Gynecol. 1988;158:898–902. doi: 10.1016/0002-9378(88)90091-9. [DOI] [PubMed] [Google Scholar]
- 23.Villar J, Repke J, Belizan J. Relationship of blood pressure, calcium intake, and parathyroid hormone. Am J Clin Nutr. 1989;49:183–4. doi: 10.1093/ajcn/49.1.183. [DOI] [PubMed] [Google Scholar]