

Abstract
Background: There are little demographic data on finger dislocation injuries. This study examines the epidemiological characteristics of patients presenting for emergency care of finger dislocations within the United States. Methods: The National Electronic Injury Surveillance System was queried for finger dislocation injuries treated in US emergency departments between 2004 and 2008. Weighted estimates, in conjunction with Census data, were used to analyze patient demographics, injury locales, and incidence rates within and between, demographic groups. Results: During the 5-year study period, an estimated 166 561 finger dislocations were treated in 1 499 222 917 person-years: an incidence rate of 11.11 per 100 000 person-years. Males were predominantly affected (78.7%) at an incidence rate of 17.8 per 100 000. The rate in females was 4.65 per 100 000 person-years. Most dislocations occurred in the 15- to 19-year age group (38.6 dislocations per 100 000 person-years). Among racial groups, blacks (16.8) were affected more than whites (7.72) or patients characterized as “other” (4.90). In terms of injury venue, 35.9% of cases took place at a sporting or recreational facility. In addition, 44.7% of sports-related dislocations occurred while playing either basketball or football. Conclusions: In the United States, finger dislocations appear to occur most often in black males 15 to 19 years of age and among sports participants, particularly basketball and football players.
Keywords: finger dislocation, emergency care, epidemiology, NEISS database
Introduction
Dislocations of the finger joints are common hand injuries with the proximal interphalangeal (PIP) joint being the most frequently affected site.4 Whether they occur as purely ligamentous injuries or with concomitant fractures, finger joint dislocations can cause significant morbidity manifesting as residual pain and stiffness. This has the potential to be especially disabling in athletes, musicians, and others who perform tasks requiring fine motor activity.3
Although much is known about the anatomy and mechanisms of ligamentous disruptions contributing to finger dislocation, there are little data on their rates of occurrence in the United States. Several epidemiological studies have successfully identified subpopulations at risk of other musculoskeletal injuries, such as shoulder dislocations and ankles sprains.15,18 Epidemiological knowledge of specific injuries is often useful for developing and implementing injury prevention strategies; for example, characterization of ulnar collateral ligamentous injuries of the thumb led to design alterations for ski equipment that decreased the likelihood of injury.6,13 Although a 2011 review of a Taiwanese national health care database reported a rate of 4.6 finger dislocations per 100 000 person-years, it is unclear if these results can be extrapolated to patients in the United States.11 Ootes et al recently identified finger laceration as the most common upper extremity injury obliging presentation for emergency care; however, no specific demographics with regard to finger dislocation were studied.11
Given that finger dislocations are easily misdiagnosed and have the potential to result in long-term morbidity if left untreated, further investigation of the epidemiology of these injuries is warranted. As most of the extant reports on finger dislocation injuries in the United States focus on specialized populations such as professional football players, the epidemiologic characteristics of such injuries in the population at large remain unknown.8 This study examines the epidemiology of finger dislocations in patients presenting for emergency care within the United States. To this end, we used the National Electronic Injury Surveillance System (NEISS) database, which has served as a statistically validated system for extrapolating national injury rates for more than 30 years.
Materials and Methods
The NEISS encompasses a sample of hospitals in the United States and is operated by the US Consumer Product Safety Commission (CPSC).9,10,14 NEISS injury data are collected from 100 emergency departments of varying sizes and geographic locations to represent a probability sample of all US hospitals with emergency rooms. Data include the age, date, sex, race, diagnosis, disposition, location where injury took place, specific body part involved, and additional descriptive comments. In addition, the database outputs a sample weight based on the stratum into which the hospital falls. Hospitals are divided into 5 strata: 4 based on yearly number of emergency room visits and a fifth for children’s hospitals. The CPSC maintains the sample by updating the sampling frame each year. The new frame lists all hospitals in the United States and its territories that have an emergency department as well as number of patients served. After appropriate adjustments to assure that hospitals in the frame conform to the required specifications, the new sampling frame is used to ratio-adjust the statistical weights for the current NEISS hospital sample to the current total number of emergency room visits. Thus, the NEISS sample weights accurately represent the total number of emergency room visits in a given year.
For this study, the NEISS database was queried for all injuries recorded as “dislocation” and “finger” over the 5-year period from January 1, 2004, to December 31, 2008. Results were obtained in 1-year increments and then combined for overall analysis. The statistical weight estimate for each case was summed to produce an estimated total number of national cases along with 95% confidence intervals (CIs). Analyses were then repeated for specific subgroups based on demographic characteristics such as 5-year age groups, gender, and race. Activity codes were also obtained from the NEISS coding manual and applied to queries to ascertain specific activities most associated with injury.10 Data on location where the accident took place were pooled for any additional correlation.
US Census national population data for the corresponding timeframe were obtained to calculate incidence rates in person-years as well as 95% CIs. The incidence rate was defined as the number of finger dislocations per 100 000 person-years. Census data can also be separated into demographic subgroups, which allowed for analysis based on the demographic characteristics listed previously. Incidence rate ratios, which are obtained by dividing one incidence rate by another, can be utilized to express the relative risk of injury when comparing subgroups. These analyses allowed for the determination of high-risk groups within the US population.
Results
A total of 4438 finger dislocations were recorded within the 5-year period from 2004 to 2008. Based on the NEISS extrapolation algorithms to estimate the number of cases presenting to emergency care facilities across the United States, this corresponds to approximately 35 362 finger dislocations annually and 131 199 total dislocations over the examined period.9,10
Age
The mean age at presentation was 28.4 years (range, 2-95 years; median = 21 years; mode = 16 years). More cases occurred between the ages of 15 and 19 years (24.7%, n = 1098) than any other single 5-year age stratum. Over half (51.8%) of all finger dislocations occurred in patients between the ages of 10 and 25 years (n = 2299; Figure 1). When examined by decade of life, fractures were most likely to occur in patients 10 to 19 years of age (40.7%, n = 1805) with each of the subsequent 2 decades incurring an approximate 50% reduction in the number of dislocations from the preceding decade, with a rate of 19.1% (n = 847) in persons aged 20 to 29 years, and 10.7% in those aged 30 to 39 years (n = 475).
Figure 1.
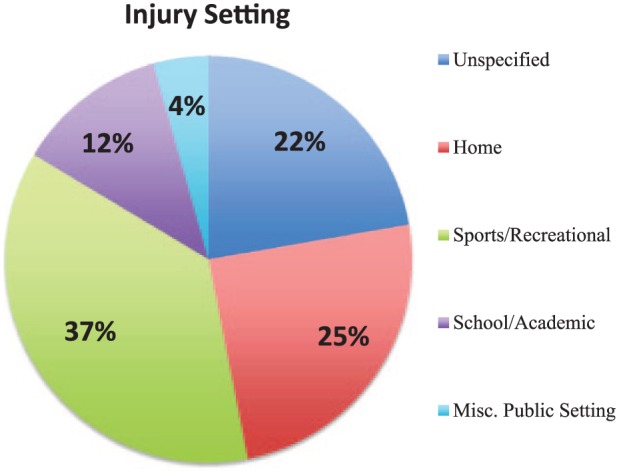
Injury setting: A Pie Chart Demonstrating the distribution of settings where finger dislocation injuries were reported to occur.
The likelihood of presenting to an emergency facility with a finger dislocation also decreased with increasing age; a steady decline in total incidence was observed between those in their fifth decade of life (6.6%, n = 147) and those in their 80s and 90s (1.4% and 0.2%, n = 64 and 12, respectively). When extrapolated to normative population values and examined in 5-year age increments, patients aged 15 to 19 years were found to be at greatest risk of finger dislocation with 38.6 dislocations per 100 000 person-years (95% CI, 33.3-43.9). Furthermore, comparing the incidence rate for this age group with the rate of 6.57 dislocations per 100 000 person-years observed in patients aged 45 to 49 yields an age-related incidence ratio of 5.87. Thus, though finger dislocations remain relatively common throughout the fourth and fifth decades of life, the incidence ratio indicates a large increase in dislocation risk among younger individuals.
Gender
Gender was described for all but one of the 4438 reported cases, revealing that 78.8% of finger dislocations occur in male patients (n = 3495) versus 21.2% in females (n = 942). When adjusted for the total US population, this represents 11.11 finger dislocations per 100 000 person-years (95% CI, 9.55-12.6). Males exhibited a computed incidence of 17.8 finger dislocations per 100 000 person-years whereas females incurred only 4.65 dislocations per 100 000 person-years. Analysis of these population estimates demonstrated an increased risk of dislocation in males, with a male-to-female incidence ratio of 3.82.
Race
Of all queried cases, race was characterized in 73.1% of total reported cases (n = 3242), revealing that 46.1% dislocations occurred in whites (n = 2045, N = 76 750), 18.5% in blacks (n = 821, N = 30 812), and 8.5% in Asian or Hispanic populations (n = 376, N = 14 111). When adjusted by incidence per total US population, Blacks sustained a disproportionately higher incidence of finger dislocations (16.8 per 100 000 person-years) compared with whites (7.72 per 100 000 person-years) or Hispanics/Asians (4.90 per 100 000 person-years). For Black patients, this results in incidence ratios of 2.17 versus whites and 3.42 versus Hispanics/Asians.
Injury Setting and Activity
A description of place or activity was included with 78.2% of dislocations recorded. Sports or recreational facilities (35.9%, n = 1593) and home (24.1%, n = 1069) constituted the most commonly reported sites. Of those dislocations described as occurring during sports activities (n = 2094), basketball was most commonly reported (25.6%, n = 1132) with football second (21.5%, n = 956). Together 47.2% of total reported cases resulted from one of these two sporting activities.
Extrapolated over the 5-year study period for all individuals with finger dislocations presenting to US emergency rooms, 69.9% (N = 116 424) dislocations are attributed to sports or recreational activities. Of these, an estimated 44.7% resulted from either basketball-related activities (N = 41 206) or football-related activities (N = 33 292), with a projected 64.0% of all sports-related finger dislocations resulting from these 2 sports alone.
Discussion
The purpose of this study was to investigate the epidemiological characteristics of US patients presenting with finger dislocations for emergency care. A review of the current literature did not yield any epidemiologic studies restricted to finger dislocation. Similar to prior studies, these data suggest that for the US population, age, gender, race, and participation in sports all constitute risk factors for incurring a finger dislocation.15,18 Our reported incidence of 11.1 dislocations per 100 000 person-years is higher than a previously reported study based on a Taiwanese population, which found an incidence of 4.6 per 100 000 person-years.17
One possible explanation for the disparity in rates of finger dislocation between these 2 populations may be secondary to differences in the types of physical activity common to each region. For instance, the second most common venue where finger dislocations were reported to occur was during participation in (American) football, a sport whose practice is largely confined to North America. However, further study into the regional prevalence of participation in different sporting activities would be needed to draw any firm conclusions.
We demonstrate that finger dislocations are more prevalent in younger patients, with the highest incidence occurring in patients between the ages of 15 and 19. This age group was also found to have between a fivefold to sixfold greater risk of sustaining a finger dislocation compared with persons aged 45 to 49. Furthermore, our data demonstrated a marked decrease in risk for dislocation with advancing age, as advancing from the first to second decades of life represented an approximate 50% reduction in the number of patients presenting to emergency care for finger dislocation. This trend continues when comparing persons presenting from 20 to 29 years of age with those aged 30 to 39 years (Figure 2). The decrease in rate of presentation with increasing age is further demonstrated by the precipitous drop in emergency room visits from those in their 40s (9.7%) to those in their 70s (2.8%).
Figure 2.

Age at the time of finger dislocation: Bar Graph depicting the percentage of recorded finger dislocations occurring within each 10-year age stratum.
The decrease in risk of finger dislocation with age suggests that younger patients may be engaged in activities that predispose them to sustaining such injuries. One likely explanation is a recently reported trend in US adolescents and teenagers devoting more hours to sport and athletic training over the last 4 decades.1,2 This trend is consistent with our projected finding of 69.9% of finger dislocations occurring during either sports or a recreational activity. Furthermore, our results suggest that certain sports place participants at greater risk of sustaining finger dislocations, as nearly half of all reported sports injuries occurred while playing either basketball or football. A National Football League review of player injuries revealed a similarly high level of finger dislocations, with PIP dislocation identified as the second most common reason for a player missing practice or a game, and finger dislocations of all types constituting 22% of reported injuries.8
Race also constituted a salient risk factor, with blacks at significantly higher risk of sustaining a finger dislocation. When compared with other predefined racial groups within the NEISS database, blacks had an incidence ratio of 2.17 versus whites and 3.42 versus Asian and Hispanic populations. Our finding of increased finger dislocation risk in black populations is consistent with previous reports detailing increased rates of extremity injuries within this population.5,12,16 Although many potential etiologies for increased injury rates have been proposed and the actual etiology is likely multifactorial, authors of previous epidemiologic studies have postulated that one such reason may be different rates of athletic exposure.15 Furthermore, it has been well demonstrated in the literature that increased participation in athletic activity correlates with an increased rate of musculoskeletal injury.7
There are several limitations to the current study. First, though a useful tool for computing population health care trends, the NEISS database only records injuries in persons presenting for emergency care.1,9,10 Therefore, patients who failed to seek medical care, or first presented to a physician in an outpatient setting, are not accounted for. Furthermore, as the NEISS database was originally created as a consumer protection device to report injuries occurring from product and equipment usage, its design may not be the ideal tool for a nationwide epidemiologic study. Last, the compiled data did not contain descriptors of the individual digit or joint involved in each dislocation event, and, in some cases, may have failed to differentiate between isolated finger dislocations and dislocations with concomitant fracture. Furthermore, the NEISS database does not distinguish between volar and dorsal dislocations, nor does it identify dislocations that required further treatment after initial presentation, information that might be useful in further identifying trends in the management of such injuries. Future studies may wish to focus on the need for secondary follow-up to further characterize the severity of finger dislocations presenting for emergency care.
In conclusion, this study provides an epidemiologic overview of finger dislocations presenting for emergency care with the United States, with age, gender, race, and sporting activity all acting as risk factors for sustaining such injuries. In particular, black teenage males engaging in sports-related activities, especially basketball and football, are at increased risk of sustaining a finger dislocation. Acknowledging that people in these demographics are more likely to sustain these injuries may inspire increased vigilance among clinicians and aid in preventing missed diagnoses or delays in treatment and the potential sequelae thereof.
Footnotes
Ethical Approval: This study was approved by our institutional review board.
Statement of Human and Animal Rights: This article does not contain any studies with human or animal subjects.
Statement of Informed Consent: The authors assert that informed consent is not applicable in this study.
Declaration of Conflicting Interests: The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The authors received no financial support for the research, authorship, and/or publication of this article.
References
- 1. Basset DR, John D, Conger SA, Fitzhugh EC, Coe DP. Trends in physical activity and sedentary behaviors of U.S. youth. J Phys Act Health. 2014;12(10):1102-1111. [DOI] [PubMed] [Google Scholar]
- 2. Birrer RB, Griesemer B, Cataletto MB. Pediatric Sports Medicine for Primary Care. Philadelphia, PA: Lippincott Williams & Wilkins; 2002. [Google Scholar]
- 3. Calfee RP, Sommerkamp TG. Fracture-dislocation about the finger joints. J Hand Surg Am. 2009;34(6):1140-1147. [DOI] [PubMed] [Google Scholar]
- 4. Chinchalkar SJ, Gan BS. Management of proximal interphalangeal joint fractures and dislocations. J Hand Ther. 2003;16(2):117-128. [DOI] [PubMed] [Google Scholar]
- 5. Davis JJ, Mason KT, Clark DA. Achilles tendon ruptures stratified by age, race, and cause of injury among active duty U.S. Military members. Mil Med. 1999;164:872-873. [PubMed] [Google Scholar]
- 6. Ganel A, Aharonson Z, Engel J. “Gamekeeper’s thumb.” Injuries of the ulnar collateral ligament of the metacarpophalangeal joint. Br J Sports Med. 1980;14(2-3):92-96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Hootman JM, Macera CA, Ainsworth BE, et al. Association among physical activity level, cardiorespiratory fitness, and risk of musculoskeletal injury. Am J Epidemiol. 2001;154:251-258. [DOI] [PubMed] [Google Scholar]
- 8. Mall NA, Carlisle JC, Matava MJ, Powell JW, Goldfarb CA. Upper extremity injuries in the National Football League: part I: hand and digital injuries. Am J Sports Med. 2008;36(10):1938-1944. [DOI] [PubMed] [Google Scholar]
- 9. The National Electronic Injury Surveillance System: a tool for researchers. U.S. Consumer Product Safety Commission Division of Hazard and Injury Data Systems. http://www.cpsc.gov/neiss/2000d015.pdf. Published March, 2000. Accessed March 2011.
- 10. NEISS coding manual. U.S. Consumer Product Safety Commission Division of Hazard and Injury Data Systems. https://www.cpsc.gov//Global/Neiss_prod/2016NonTraumaNEISSCodingManual.pdf. Published 2011. Accessed March 2011.
- 11. Ootes D, Lambers KT, Ring DC. The epidemiology of upper extremity injuries presenting to the emergency department in the United States. Hand. 2012;7(1):18-22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Owens BD, Mountcastle S, White D. Racial differences in tendon rupture incidence. Int J Sports Med. 2007;28:617-620. [DOI] [PubMed] [Google Scholar]
- 13. Scalcione RL, Pathria MN, Chung CB. The athlete’s hand: ligament and tendon injury. Semin Musculoskelet Radiol. 2012;16:338-350. [DOI] [PubMed] [Google Scholar]
- 14. Schroeder T, Ault K. The NEISS Sample (Design and Implementation) 1997 to Present. U.S. Consumer Product Safety Commission Division of Hazard and Injury Data Systems; 2001. [Google Scholar]
- 15. Waterman BR, Owens BD, Davey S, Zacchilli MA, Belmont PJ., Jr. The epidemiology of ankle sprains in the United States. J Bone Joint Surg Am. 2010;92:2279-2284. [DOI] [PubMed] [Google Scholar]
- 16. White DW, Wenke JC, Mosely DS, Mountcastle SB, Basamania CJ. Incidence of major tendon ruptures and anterior cruciate ligament tears in US Army soldiers. Am J Sports Med. 2007;35:1308-1314. [DOI] [PubMed] [Google Scholar]
- 17. Yang NP, Chen HC, Phan DV, et al. Epidemiological survey of orthopedic joint dislocations based on nationwide insurance data in Taiwan, 2000-2005. BMC Musculoskelet Disord. 2011;12:253. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Zacchilli MA, Owens BD. Epidemiology of shoulder dislocations presenting to emergency departments in the United States. J Bone Joint Surg Am. 2010;92:542-549. [DOI] [PubMed] [Google Scholar]