

Pneumorrhachis is defined as presence of air within the spinal epidural space. A fourteen years nonsmoker and nondrug addict known asthmatic male complained of sudden onset shortness of breath, nonproductive cough and wheezing for past 48 hours. There was neither any previous history of pulmonary tuberculosis nor any recent trauma or surgery. On clinical examination, he was fully conscious and oriented but mildly dyspneic. Auscultation revealed a systolic crunching sound over the chest. Patient was afebrile and vital signs were normal. All the baseline biochemical investigations were within normal limits.
Chest radiograph confirmed the presence of extensive subcutaneous emphysema involving the cervical, thoracic and axillary regions bilaterally, without any evidence of rib fracture (Fig. 1). Also there was air in the mediastinum and pericardium. CT chest (Fig. 2) confirmed pneumorrhachis, pneumomediastinum, pneumopericardium and subcutaneous emphysema. There was no evidence of pulmonary interstitial emphysema or any bullae on HRCT. No pneumothorax was recognized. The patient was admitted and was treated with antibiotics, inhalation bronchodilators, systemic corticosteroids, high-flow oxygen and other supportive measures. Antibiotics were administered to prevent mediastinitis. His hospital course was uneventful and he showed progressive improvement.
Fig. 1.

Plain chest radiograph showing subcutaneous emphysema (white arrow) and pneumomediastinum (black arrow)
Fig. 2.
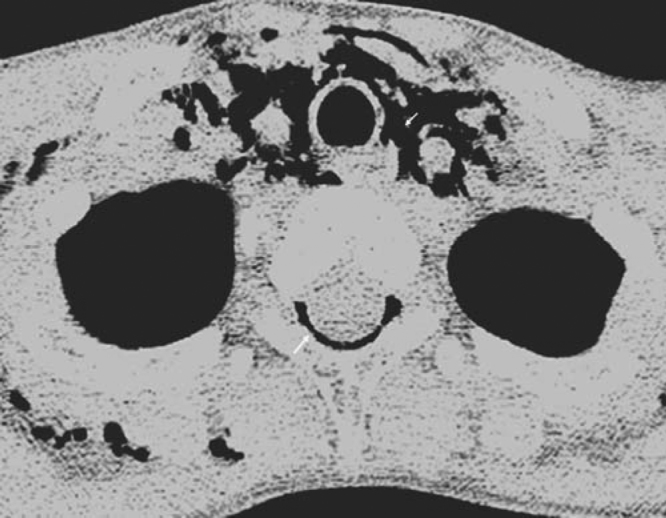
Axial CT at upper thoracic level demonstrating pneumorrhachis, pneumomediastinum and subcutaneous emphysema (arrows)
In case of bronchial asthma, violent coughing and acute increase in the intra-thoracic pressure can cause pneumorrhachis [1]. Free air in the epidural space is an uncommon phenomenon that was first reported by Gordon et al [2] in 1977. Newbold et al [3] introduced the term pneumorrhachis in 1987.
Pneumorrhachis can be classified into internal i.e. intradural (intra-spinal air within the subdural or subarachnoid space) and external i.e. extradural (intra-spinal, epidural air) [1, 2]. There are no facial barriers to prevent communication of the posterior mediastinum or the retro-pharyngeal space with the epidural space. Air communicates via the neural foramina and collects in the epidural space. There is low resistance from the loose connective tissues as compared with the rich vascular network present anteriorly, so the dissected air preferably collects in the posterior epidural space [4]. In the differential diagnosis, intra-spinal gas collection due to degenerative, malignant, inflammatory and infectious diseases caused by gas-forming organisms has to be considered.
References
- 1.Oertel NF, Korinth MC, Reinges ME, Krings T, Terbeck S, Gilsbach JM. Pathogenesis, diagnosis and management of pneumorrhachis. Bur Spine J. 2006;15:636–643. doi: 10.1007/s00586-006-0160-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Gordon IJ, Hardman DR. Thetramnatic pneumomyelogram. A previously undescribed entity. Neuroradiology. 1997;13:107–108. doi: 10.1007/BF00339843. [DOI] [PubMed] [Google Scholar]
- 3.Newbold RC, Wiener MD, Vogler JB, 3rd, Martinez S. Traumatic pneumorrhachis. AJR Am J Roentgenol. 1987;148:615–616. doi: 10.2214/ajr.148.3.615. [DOI] [PubMed] [Google Scholar]
- 4.Easa M, Kandpal H, Sharma R, Misra A. Spontaneous pneumorrhachis in bronchial asthma. Act Radiol. 2006;47:672–674. doi: 10.1080/02841850600797010. [DOI] [PubMed] [Google Scholar]