

Introduction
Similarities in the embryogenesis of breast and salivary gland and the dual epithelial myoepithelial cell differentiation in both anatomical sites account for the occurrence of salivary gland-type neoplasm in the breast [1]. Pleomorphic adenoma (PA) is one such benign neoplasm that occurs in both salivary gland and breast. In salivary gland, malignant transformation of PA is a well-recognized, albeit relatively, uncommon event. Malignant transformation can take the form of superimposed adenocarcinoma or development of a malignant mixed tumour with dual epithelial and mesenchymal elements [2]. PA, also known as benign mixed tumour, accounts for 45 to 74% of all major and minor salivary gland tumours and has been reported in other, less common sites such as the paranasal sinuses, larynx, palate, nasal septum, skin and breast [3, 4], It occurs less frequently in the human breast. Since the first case report by Lecene [4] in 1906, 68 cases of PA of the human breast have been documented in the world literature [5]. Malignant PA has been reported to occur outside of the major salivary glands but its occurrence in breast is rare. There are only three such case reports in English language literature [1]. However, there is no case of epithelial-myoepithelial carcinoma on a PA of breast reported. We describe a case of epithelial-myoepithelial carcinoma ex pleomorphic adenoma of breast diagnosed and managed at our hospital.
Case Report
A forty three year old post menopausal lady, a daily wage laborer, presented to our hospital with a slowly growing, painless lump in her right breast of four years duration. Clinically she had a firm, mobile, non tender 4 × 3 cm lump in her upper outer quadrant of right breast with no axillary lymphadenopathy. Ultrasound and Mammography was reported to be BIRADS III for right breast. FNAC and a core needle biopsy revealed a low grade epithelial lesion. With a clinical suspicion of a probable low grade epithelial malignancy involving right breast a wide local excision of the lesion was done. No axillary dissection was done. Postoperative recovery was uneventful. Histopathology examination revealed a tumour composed of both myoepithelial and epithelial components. In addition, the tumour also showed areas of PA in the form of admixture of epithelial and stromal elements. The epithelial component was of glandular nature with areas of squamous metaplasia and keratinous cysts. The stroma was of fibromyxoid quality with hyalinized areas. There was no necrosis or lymphovascular and perineural invasion (Fig. 1, Fig. 2). Immunohistochemistry (IHC) was positive for Smooth Muscle Actin (SMA) and S-100 proteins in myoepithelial area (Fig. 3). Epithelial area was positive for Cytokeratin and EMA (Fig. 4). Final histopathological diagnosis was epithelial-myoepithelial carcinoma ex pleomorphic adenoma of right breast. She was advised a three monthly follow up for first year and a six monthly follow up thereafter, no adjuvant treatment was given. She has completed two and half years of follow up.
Fig. 1.
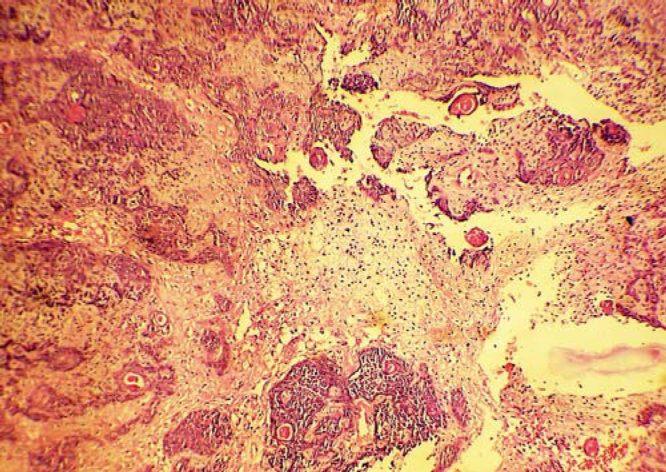
H&E stained section (100x) tumour composed of areas of myxoid stroma and epithelial components resembling pleomorphic adenoma.
Fig. 2.
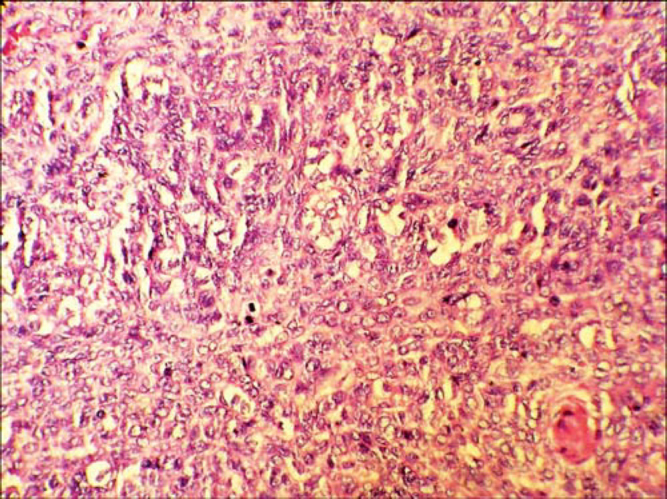
H&E (400x) sheets of myoepithelial cells with brisk mitotic activity.
Fig. 3.
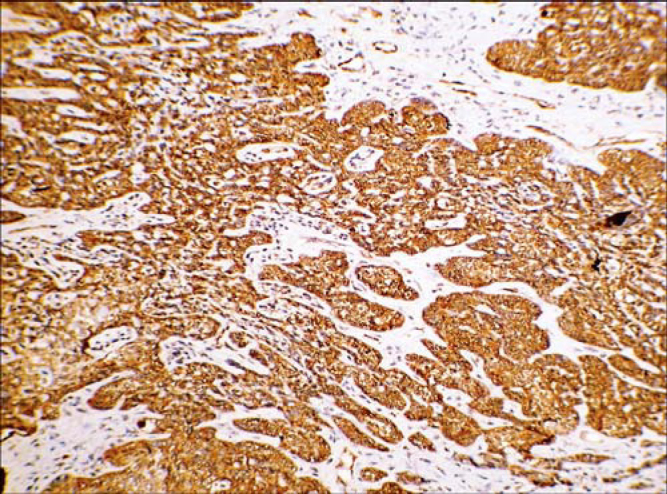
IHC positive for SMA.
Fig. 4.
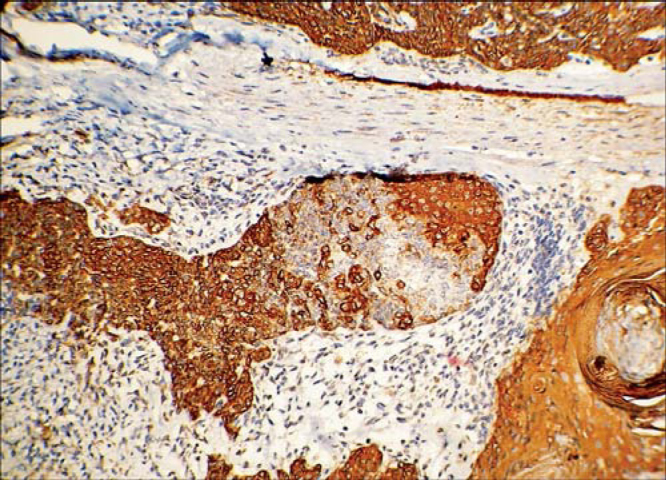
IHC positive for cytokeratin.
Discussion
Myoepithelial cells are a normal component of the breast tissue and their presence in neoplastic lesions has been considered a hallmark of benignity. However, breast neoplasms have been described that are entirely or partially composed of myoepithelial cells. Neoplasms of purely myoepithelial origin have been called myoepitheliomas and may be benign or malignant. Tumours with bicellular proliferation of both epithehal and myoepithelial cells are called adenomyoepitheliomas. Although most of these are benign, malignancy has been reported and called as malignant adenomyoepitheliomas or epithelial-myoepithelial carcinomas.
Pleomorphic adenoma is the most common tumour of glandular origin in the head and neck [6] but its occurrence in breast is rare. Carcinoma ex pleomorphic adenoma is a carcinoma involving any component of the benign mixed tumour and is characterized by rapid growth and pain. In our case it had involved both the epithelial and myoepithelial component of the breast tissue. Epithelial-myoepithelial carcinoma of the breast, a lesion composed of malignant epithelial and myoepithelial cells, remains a rarely reported phenomenon. Epithelial-myoepithelial carcinomas arising from a PA of salivary glands have been reported in literature; however those arising from the breast have not been reported so far [7]. While the histologic, immunohistochemical and even ultrastructural features have been well described, a definite diagnosis of epithelial-myoepithelial carcinoma based on cytology alone remains challenging [8] as was seen in our case where a repeated FNAC and core needle biopsy could not reveal the malignancy.
From the available literature it appears that epithelial-myoepithelial carcinoma is a low-grade malignancy. They are however known to have local recurrences after excision and lung metastasis, though rare, are the most frequent sites of distant metastases [8, 9]. The prognosis of carcinoma ex pleomorphic adenoma post wide local excision is favourable. Prognosis of epithelial-myoepithelial carcinoma of breast is unpredictable as it can take a natural course similar to or even worse than an adenocarcinoma of breast and largely depends on the histological features such as mitotic counts, cellularity and their pleomorphism, necrosis and invasion of the surrounding tissue. The recurrence rate is lowered following WLE of such malignancies as the predominance of epithelial component in these tumours is considered as a favourable factor.
Epithelial-myoepithelial carcinoma ex pleomorphic adenoma of breast is an exotic rarity and we report the first case in English literature, which was managed successfully at our centre.
Conflicts of Interest
None identified.
References
- 1.Malcolm MH, David L, Christophe G, Del Vecchio Marina, Vincenzo E. Carcinoma ex-pleomorphic adenoma of the breast. Report of three cases suggesting a relationship to metaplastic carcinoma of matrix-producing type. Virchows Arch. 2005;446:142–149. doi: 10.1007/s00428-004-1137-7. [DOI] [PubMed] [Google Scholar]
- 2.Sauer T. Cytologic findings in malignant myoepithelioma: a case report and review of the literature. Cytojournal. 2007;4:3. doi: 10.1186/1742-6413-4-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Rosai J. Pleomorphic adenoma of the salivary gland and breast. In: Rosai J, editor. Ackerman's Surgical Pathology. Mosby-Year Book Inc; St Louis: 1996. [Google Scholar]
- 4.Lecene AL. Observation d'un cas de tumour “mixte” du sein. Rev Chir (Paris) 1906;33:434–468. [Google Scholar]
- 5.Nicholosan MR, Bleiwiss I, Pace B, Azueta V, Jaffer S. Pleomorphic Adenoma of the Breast: A case report and distinction from mucinous carcinoma. Archives of Pathology and Laboratory Medicine. 2002;127:474–477. doi: 10.5858/2003-127-0474-PAOTB. [DOI] [PubMed] [Google Scholar]
- 6.Gnepp DR, Wenig BM. In: Surgical Pathology of the Salivary Gland in Oral and Maxillofacial Pathology. Allen CM, Auclair PL, Ellis GL, Gnepp DR, Wenig BM, Janney GG, editors. WB Sounders; Philadelphia: 1991. pp. 350–368. [Google Scholar]
- 7.Yahya D, Shahrzad N, Bijan K, Khosrow D. Epithelial myoepithelial carcinoma of the parotid gland with malignant ductal and myoepithelial components arising in a pleomorphic adenoma: A case report with cytologic, histologic and immunohistochemical correlation. Acta Cytol. 2007;51:807–813. doi: 10.1159/000325847. [DOI] [PubMed] [Google Scholar]
- 8.Daniel L, Yayan C, Kiyoe K, Kamani L. Infiltrating myoepithelial carcinoma of the breast a case report and cytologic-histologic correlation. Diagnostic Pathology. 2008;3:7. doi: 10.1186/1746-1596-3-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Maria P, Foschini VE. Carcinomas of the breast showing myoepithelial cell differentiation — A review of the literature. Virchows Arch. 1998;432:303–310. doi: 10.1007/s004280050170. [DOI] [PubMed] [Google Scholar]