

INRODUCTION
Primary pyomyositis, a suppurative disease caused chiefly by Staphylococcus aureus, affects predominantly large skeletal muscles of the lower limbs. Involvement of perisciatic muscles is rare and is recognised late due to rarity, ambiguity, and minimal disability caused by the ailment. Diagnosis using computerised tomography (CT), magnetic resonance imaging (MRI), and treatment by antibiotics/drainage forms the mainstay of management. We share the typical clinical presentation and CT image of a large primary obturator internus (OI) pyomyositis, and validate the efficacy of transabdominal extraperitoneal approach, hitherto unreported in the literature, for its drainage.
CASE REPORT
Previously healthy 65-year-old man presented with seven days history of fever and pain in right buttocks. There was no history of trauma. General and local examinations were unremarkable excepting pyrexia (102°F). Differential leukocyte count showed predominance of polymorphs (87%); however, other laboratory investigations, including the total leukocyte count (8,100/mm3), were normal. Chest, pelvis, and spine radiographs did not reveal any abnormality. Ultrasonography suggested collection near right hip joint. CT pelvis revealed bulky right OI, quadrates femoris, gemelli and a 5 × 3 cm2 collection within right OI indenting the urinary bladder (Figures 1A and B). Around 35 mL of thick odourless pus was drained from right OI through a transabdominal extraperitoneal approach (Figure 2), following which pain and fever subsided. Staphylococcus was isolated from the pus. Cloxacillin was added to ongoing augmentin and amikacin regimen based on antibiotic sensitivity. Patient made a remarkable recovery.
Figure 1(A, B).
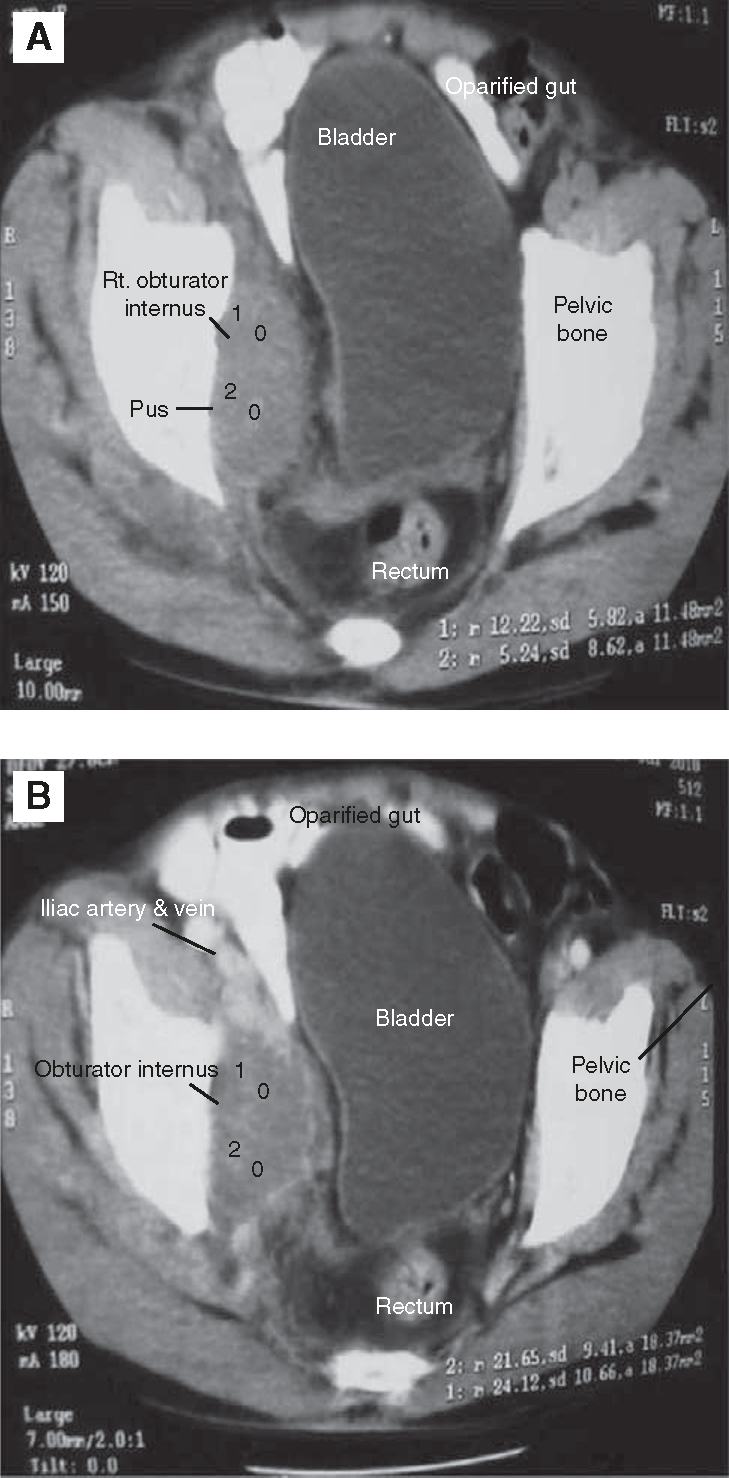
Computerised tomography pelvis showing bulky right obturator internus with a 5 × 3 cm2 collection within it.
Figure 2.
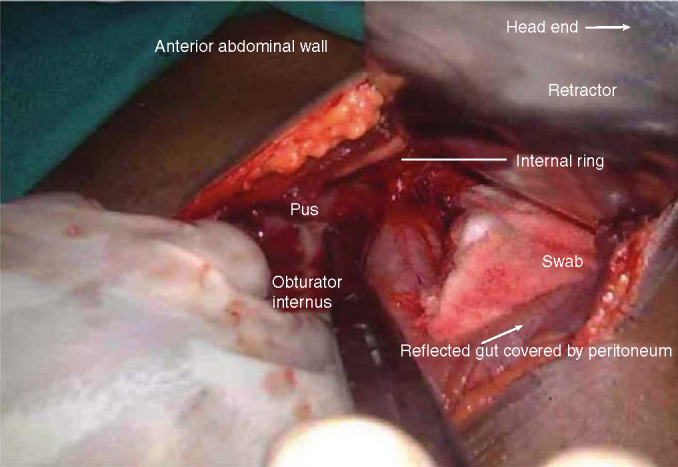
Per operative photo showing the transabdominal extraperitoneal drainage of the right obturator internus pyomyositis.
DISCUSSION
Pyomyositis, a tropical disease, affects previously healthy youth (mean age: 10 years), with slight female predominance (3F:2M).: However, no age is exempt, as evident by this case. Predilection for lower limb muscles, especially, quadriceps, iliopsoas, glutei, and hamstrings, is known.2, 3 Perisciatic muscle involvement, such as, OI is rare (< 25 documented cases).3
It is believed that small intramuscular haematomas, caused by trivial trauma, get infected by transient bacteraemia/contiguous spread from adjacent organs, resulting in pyomyositis.1, 2, 3 S. aureus is isolated in > 75% of cases.1, 2, 3 Streptococcus, Escherichia coli, Haemophilus influenzae, Citrobacter, Fusobacter, Peptostreptococcus, Gonococcus, Klebsiella, Serratia, and Yersinia enterocolitica are some of the other bacteriae involved.3 Fever and hip/groin pain are invariable presentations with a mean duration of three days.1, 2, 3 Polymorphonuclear leukocytosis and positive blood cultures provide early hint towards infective aetiology.2, 3 However, diagnosis is often delayed as clinical suspicion is blunted by the rarity, ambiguity and minimal disability caused by the disease.3
Contrast-enhanced MRI (gold standard) and CT scans have been the foundation of timely diagnosis.1, 2, 3 However, Tc99/radiolabelled WBC scans have also been useful.3 Osteomyelitis and septic arthritis are important differential diagnosis as well as complication of this disease.1, 2, 3 Other confounding diagnoses are necrotising myositis, muscle pull/contusion, and phlebothrombosis.4
Antibiotics, either singly or in combination, with open/image guided drainage, has been the main stay of management.1, 2, 3 Conservative management is likely to succeed if infection is detected early with minimal/no abscess formation.2, 3 However, large abscesses do warrant formal drainage.2, 3 Medial hip approach has been used for drainage by orthopaedic surgeons, probably owing to familiarity of approach and small sizes of abscesses.1 Nevertheless, exposure provided by this approach may be limited for an abscess as large as in this patient. We chose the transabdominal extraperitoneal approach as it combines the benefits of abundant exposure with safety of avoiding vital structures and peritoneal contamination.
CONCLUSION
Summing up, OI pyomyositis is rare. CT proves pivotal in its diagnosis and transabdominal extraperitoneal drainage proves efficacious in its management.
ACKNOWLEDGEMENT
We record our gratitude to Lt Col Ojha, Clinical & Classified Specialist (Medicine), Military Hospital Agra for handling initial management and transferring the case to us. Photography assistance of Nk/ORA Maruti is gratefully acknowledged.
CONFLICTS OF INTEREST
None identified.
REFERENCES
- 1.King RJ, Laugharne D, Kerslake RW, Holdsworth BJ. Primary obturator pyomyositis: a diagnostic challenge. J Bone Joint Surg [Br] 2003;85–B:895–898. [PubMed] [Google Scholar]
- 2.Mukhtyar C, Bradlow A. Primary obturator myositis. Rheumatology. 2005;44:408–410. doi: 10.1093/rheumatology/keh492. [DOI] [PubMed] [Google Scholar]
- 3.Nikolopoulos DD, Apostolopoulos A, Polyzois I, Liarokapis S, Michos I. Obturator internus pyomyositis in a young adult: a case report and review of the literature. Cases J. 2009;2:85–88. doi: 10.4076/1757-1626-2-8588. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Bharathi RS, Sharma V, Sood R, Chakladar A, Singh P, Raman DK. Management of necrotizing myositis in a field hospital: a case report. Scand J Trauma Resusc Emerg Med. 2009;17:20. doi: 10.1186/1757-7241-17-20. [DOI] [PMC free article] [PubMed] [Google Scholar]