

Introduction
Descemet's membrane detachment (DMD) is an uncommon condition which has recently been reported in literature following a variety of factors like cataract surgery, trauma and corneal ectasia. However, inadvertent descemetorhexis leading to Descemet's membrane deficit is under reported and very few literature reports are available. The management of such cases warrants a conservative approach as relatively good visual outcome can be obtained over a period ranging from three to six months. We report here a case of corneal oedema following inadvertent descemetorhexis in phacoemulsification cataract surgery which underwent spontaneous resolution within four months. To our knowledge, this probably is only the fourth such case reported worldwide and second case from the Indian subcontinent.
Case Report
A 76 year-old male was seen in our out patient department (OPD) with a gradual deterioration of vision in his left eye. He had no past ocular history. His general and systemic examination was normal. On examination the visual acuity was 6/9 in the right and counting of fingers in the left. There was a grade I nuclear sclerosis in right eye and dense nuclear cataract (grade IV) in the left eye. There were no other ocular abnormalities. Patient was planned for cataract surgery of left eye.
The patient underwent phacoemulsification cataract extraction with intraocular lens implant in left eye under peribulbar anaesthesia. Scleral tunnel incision (inverted frown shaped) was made. Initial incision was made with number 11 blade and tunnel construction with a crescent knife. Entry into anterior chamber was made with a 3.2 mm keratome and while doing so, the tip of the keratome inadvertently touched the central cornea but no Descemet's detachment or flap was noticed at that time. Subsequently continuous curvilinear capsulorhexis (CCC) was made and Phaco chop technique phacoemulsification was performed using a Storz machine (STORZ, USA). Viscoelastic (Healon) was used throughout the procedure and was completely removed at the end of the procedure. As the CCC was compromised during the surgery, scleral tunnel was extended and rigid intraocular lens (six mm optic) was implanted after inflating the capsular bag with viscoelastic. Loss of Descemet's membrane in a circular area in the central cornea was realized only at the end of the surgery. Since there was no detached Descemet's membrane flap or scrolled edge, repositioning was not indicated. An air bubble was injected in the anterior chamber. Subconjunctival injection of dexamethasone and amikacin was given and the eye was covered with a plastic shield.
On the first postoperative day there was diffuse corneal oedema in the operated eye (left) and visual acuity was hand movements close to face. The patient was started on topical steroids, antibiotics, antiglaucoma agents and non-steroidal anti-inflammatory drugs (NSAIDs). Hyperosmotic eye drops were given four hourly. The patient was reviewed five days following surgery. His visual acuity was counting fingers at one foot. There were peripheral Descemet's membrane folds and the intraocular pressure was 15 mm of Hg in the right eye and 12 mm of Hg in the left eye.
The patient was subsequently seen at two weeks and at four weeks postoperative period. There was gradual clearing of cornea and his visual acuity at four weeks improved to counting finger at two feet in left eye. An oval central Descemet's membrane deficit of about 4.5 mm width and 3.5 mm height was visualized with the centre of oval area placed slightly below the pupillary margin (Fig. 1). The patient was explained about the visual prognosis of the condition and was asked to continue the same medication for another eight weeks as he was going away to his village for some personal reasons. No surgical management was contemplated at this juncture.
Fig. 1.
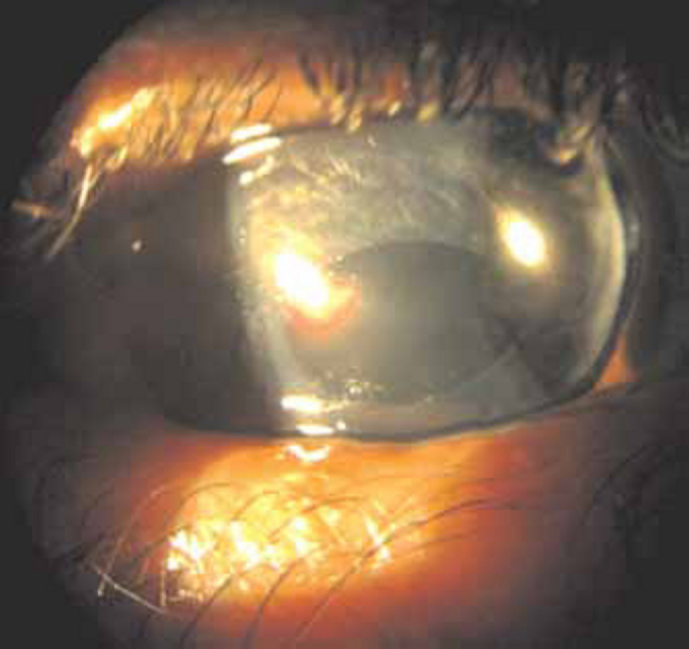
Four weeks after surgery, a slit lamp view of the left eye shows diffuse corneal oedema with slight clearing of oedema over large central oval deficit of the Descemet's membrane.
Patient was seen at 14 weeks postoperative period and his visual acuity was found to be counting finger at three feet in left eye improving to 6/36 with pinhole on further clearing of corneal oedema. The intraocular pressure was 12 mm of Hg in both eyes. Patient was further continued on topical hyperosmotics (Hypersol 5%) and low potency steroid (Fluorometholone), both six hourly for a further period of four weeks.
At 18 weeks patient had a visual acuity of 4/60 in left eye improving to 6/24 with -4.0 diopter cylinder at 110° axis. Left eye showed clear cornea above the area of Descemet's membrane deficit (Fig. 2, Fig. 3) and slight irregularity at the junction of Descemet's membrane deficit with normal posterior corneal layer (Fig. 4). Specular microscopy showed central endothelial cell count of 2344 cells/mm2 in right eye and 1222 cells/mm2 in left eye. There was evidence of polymegathism and pleomorphism in the left eye. All medications were stopped and patient was prescribed spectacles.
Fig. 2.
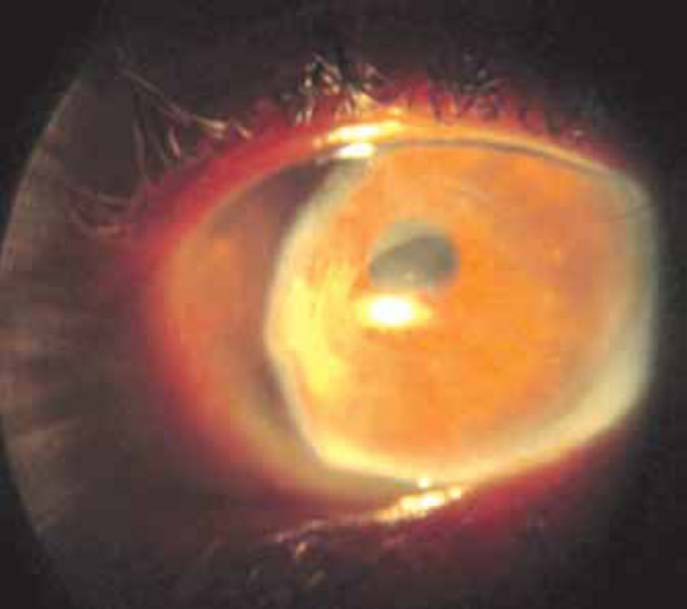
Slit lamp view of the left eye shows further clearing of corneal oedema over Descemet's membrane deficit at 18 weeks.
Fig. 3.
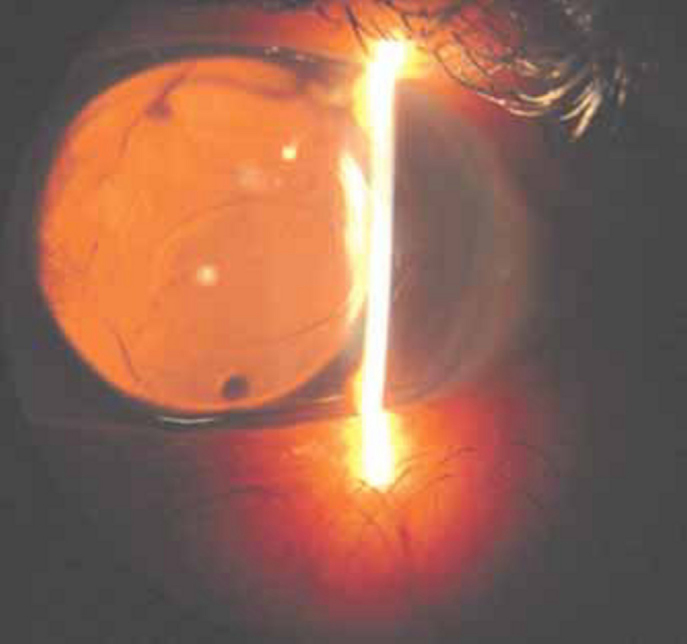
Trans-illumination view of the left eye showing clear cornea with oval Descemet's membrane deficit at 18 weeks and posterior chamber intraocular lens in situ.
Fig. 4.
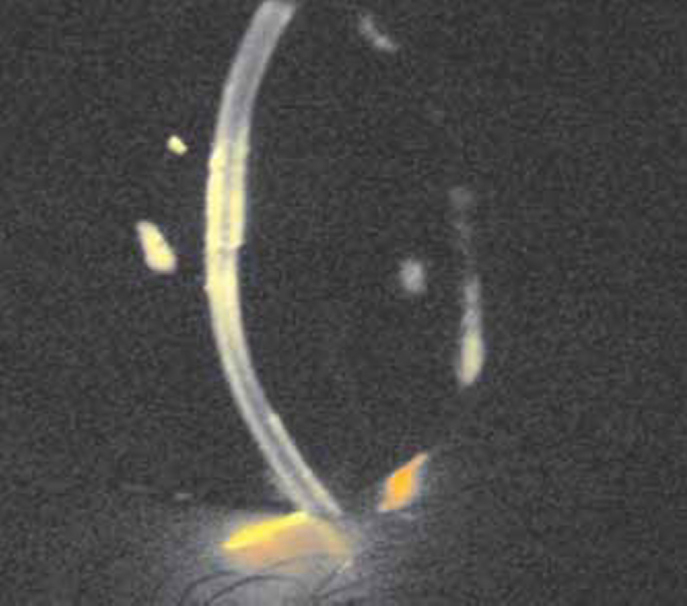
Oblique view of the cornea of left eye showing irregular posterior endothelial surface at 18 weeks.
Discussion
Descemet's membrane detachment (DMD) can be caused by surgical and non surgical factors. The surgical factors include cataract surgery (intracapsular, extracapsular, small incision cataract surgery and phacoemulsification surgery), iridectomy, keratoplasty and non-surgical factors include trauma, congenital glaucoma and corneal ectasias like keratoconus and keratoglobus.
DMD is not an uncommon complication after cataract surgery but the incidence following phacoemulsification surgery is very low (0.5%) [1]. Inadvertent descemetorhexis as a cause of DMD has been reported in only three cases worldwide [2, 3, 4].
In our case, injury to cornea occurred while entering anterior chamber. However, we are not sure about the reason of loss of Descemet's membrane. While entering the anterior chamber the tip of the keratome inadvertently touched the central cornea but no Descemet's detachment or flap was noticed at that time. The initial corneal injury accompanied by possible brushing of cornea by instruments including phaco tip, rigid intraocular lens and irrigation/aspiration probe might have led to loss of Descemet's membrane.
The management of DMD with a conservative approach gives fairly good visual outcome. Vastine et al [5] suggested surgical intervention for large planar and scrolled detachments. Walland et al [6] also recommended repair of large DMD and that an expanding gas should be used. Spontaneous resolution of such cases has been reported only in very few cases. Feys et al [7] in 2002 reported spontaneous clearing of corneal oedema after descemet's detachment in six months. Iradier et al [8] in 2002 reported late spontaneous resolution of massive detachment of Descemet's membrane after ten months. Watson et al [9] in 2006 reported late spontaneous resolution of DMD after a period of six month. In three reported cases of inadvertent descemetorhexis during phacoemulsification, cornea cleared in one month, five months and six months respectively [2, 3, 4]. Spontaneous resolution of corneal oedema in our case occurred over a period of four months (the second fastest clearing of corneal oedema in such cases).
Endothelial cell layer reforms itself by migration and increase in size of remaining endothelial cells [2]. Corneas with preexisting endothelial polymegathism show a slower return to preoperative pachymetry [10]. Previous studies found that in case of a previously diseased endothelium, postoperative corneal edema is greater than those with a healthy endothelium [3]. In our case the good endothelial cell count in the right eye suggests a similar good preoperative count in the left eye which may be one of the reasons of faster recovery.
In summary, inadvertent descemetorhexis leading to corneal oedema during cataract surgery can be treated conservatively with topical hyperosmotics, steroids, antiglaucoma agents, NSAIDs and antibiotics. This case highlights that a healthy endothelium can undergo pleomorphism and polymegathism leading to reversal of corneal oedema despite a low endothelial count.
Conflicts of Interest
None identified
References
- 1.Khng CY, Voon LW, Yeo KT. Causes and management of Descemet's membrane detachment associated with cataract surgery - not always a benign problem. Ann Acad Med Singapore. 2001;30:532–535. [PubMed] [Google Scholar]
- 2.Pan JC, Au Eong KG. Spontaneous resolution of corneal oedema after inadvertent descemetorhexis during cataract surgery. Clin Experiment Ophthalmol. 2006;34:896–897. doi: 10.1111/j.1442-9071.2006.01360.x. [DOI] [PubMed] [Google Scholar]
- 3.Aggarwal A, Jacob S, Aggarwal S. Iatrogenic descemetorhexis as a complication of phacoemulsification. J Cataract Refract Surg. 2006;32:895–897. doi: 10.1016/j.jcrs.2006.01.070. [DOI] [PubMed] [Google Scholar]
- 4.Braunstein RE, Airiani S, Chang MA. Corneal oedema resolution after descemetorhexis. J Cataract Refract Surg. 2003;29:1436–1439. doi: 10.1016/s0886-3350(02)01984-3. [DOI] [PubMed] [Google Scholar]
- 5.Vastine DW, Weinberg RS, Sugar J, Binder PS. Stripping of Descemet's membrane associated with intraocular lens implantation. Arch Ophthalmol. 1983;101:1042–1045. doi: 10.1001/archopht.1983.01040020044006. [DOI] [PubMed] [Google Scholar]
- 6.Walland MJ, Stevens JD, Steele AD. Repair of Descemet's membrane detachment after intraocular surgery. J Cataract Refract Surg. 1995;21:250–253. doi: 10.1016/s0886-3350(13)80127-7. [DOI] [PubMed] [Google Scholar]
- 7.Feys J, Mohand-Said M, Nodarian M. Spontaneous clearing of the cornea with detachment of Descemet's membrane. J Fr Ophthalmol. 2002;25:502–504. [PubMed] [Google Scholar]
- 8.Iradier MT, Moreno E, Aranguez C. Late spontaneous resolution of a massive detachment of Descemet's membrane after phacoemulsification. J Cataract refract Surg. 2002;28:1071–1073. doi: 10.1016/s0886-3350(01)01220-2. [DOI] [PubMed] [Google Scholar]
- 9.Watson SL, Abiad G, Coroneo MT. Spontaneous resolution of corneal oedema following Descemet's detachment. Clin Experiment Ophthalmol. 2006;34:797–799. doi: 10.1111/j.1442-9071.2006.01319.x. [DOI] [PubMed] [Google Scholar]
- 10.Rao GN, Shaw EL, Arthur EJ. Endothelial cell morphology and corneal deturgescence. Ann Ophthalmol. 1979;1:885–899. [PubMed] [Google Scholar]