

Abstract
Renal cortical necrosis (RCN), a rare cause of renal failure in which there is death of the renal cortex but sparing of the medulla, is a catastrophic entity with high mortality. Its incidence and severity are higher in developing countries, mostly due to pregnancy-related complications. This paper presents the case of a 65-year-old woman who had bilateral renal cortical necrosis caused by bisphosphonate medication that was diagnosed by CT scan during the acute initial phase of the disease.
Background
Renal cortical necrosis (RCN) is a rare cause of acute renal failure in which there is death of the renal cortex and sparing of the medulla. This is a catastrophic entity with high mortality (1). The pathophysiology of the necrosis may be related to ischemia due to constriction of small intracortical blood vessels, whether related to toxins, circulating hormones, or neural stimuli. Its incidence and severity are higher in developing countries, mostly due to pregnancy-related complications. Nonobstetric causes of RCN include extensive burns, snake bites, sepsis, hemolytic uremic syndrome, pancreatitis, dehydration in infancy or childhood, organophosphorous poisoning, and the use of nonsteroidal anti-inflammatory drugs (2, 3, 4, 5, 6). Sepsis with septic shock is the most common (30–40%) nonobstetric cause of RCN (7, 8). A rare case of bilateral RCN diagnosed by the specific findings of a computed tomography (CT) scan during the acute initial phase of the disease is presented in this paper. Renal impairment associated with acute RCN caused by bisphosphonate has not previously been recorded in the literature.
Case report
A 65-year-old woman with no significant medical history was admitted to the hospital complaining of worsening respiratory distress and low back pain. Several hours later, she was transferred to the intensive care unit of our hospital. She took a drug containing bisphosphonate for the treatment of osteoporosis one day before admittance to the hospital.
Her blood pressure was 132/85 mmHg, and pulse rate was 145/min. The initial laboratory data included a hematocrit of 39%, white-cell count of 10,300/mm3, serum urea nitrogen of 58 mg/dl, creatinine 1.85 mg/dl, serum sodium 128 mEq/L, potassium 5 mEq/L, and chloride 101 mEq/L. Lactate dehydrogenase (LDH) was 345, serum glutamic oxaloacetic transaminase was (SGOT) 90 U/L, creatine kinase (CK) was 422 U/L, and bilirubin was 3.07 mg/dl. The abnormal coagulation profile was compatible with disseminated intravascular coagulation (DIC). Contrast-enhanced computed tomography (CT) of the abdomen was performed. In addition, CT showed a hypodense zone of the renal cortex and hyperdense medulla, suggestive of further collateral circulation to the subcapsular area and congestion in the medulla. There was no excretion of contrast media into the collecting system (Fig. 1, Fig. 2).
Fig. 1.
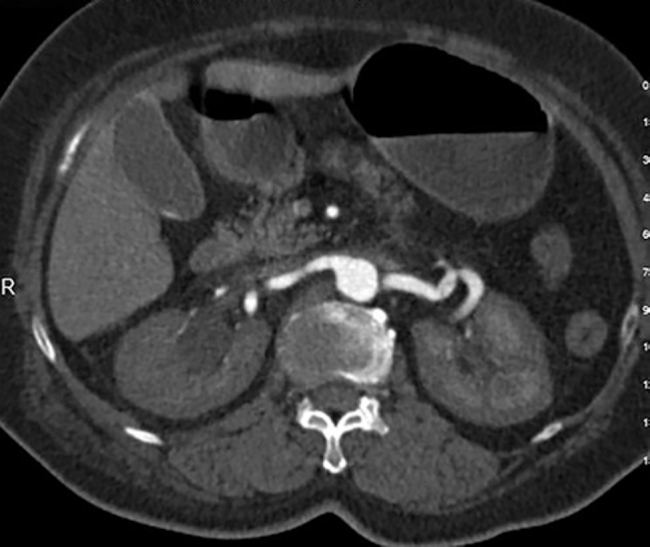
65-year-old woman with bilateral renal cortical necrosis. The bilateral renal cortex was not enhanced despite the fact that the renal arteries would normally be enhanced in the arterial phase of the CT scan (Axial CT, 140 mAs, 120 kV, 3mm slice thickness, 100ml IV contrast material).
Fig. 2.

65-year-old woman with bilateral renal cortical necrosis. The bilateral renal medulla was well enhanced in the parenchymal phase of the CT scan. However, the bilateral renal cortex was still not enhanced (Axial CT, 140 mAs, 120 kV, 3mm slice thickness, 100ml IV contrast material).
Despite hemodialysis, anticoagulation, and other supportive measures, her condition deteriorated and she died one week later.
Discussion
Diffuse acute bilateral RCN is a rare but a catastrophic and irreversible form of acute renal failure. Cortical necrosis generally results from decreased blood supply within the microcirculation of the renal cortex following septic shock or volume depletion. This is characterized by necrosis of the entire cortex apart from a thin rim of viable tissue in the subcapsular, juxtaglomerular areas, and in the medulla (Table 1). The isolated necrosis of the renal cortex is thought to be due to intravascular thrombosis of the interlobular and afferent arterioles (1). The corticomedullary junction nephrons are supplied by the arcuate arteries, while the subcapsular nephrons derive their vascular supply from a rich and extensive anastomotic network and extrarenal vascular supply. Both of these latter two regions are usually spared from infarction in acute cortical necrosis (1, 9). However, a generally accepted mechanism has not been produced yet. In one theory, RCN can be thought of as an event precipitated by underlying causes such as abruptio placentae, sepsis, toxins, burns, trauma, or hemorrhagic pancreatitis, which then interact with various physiologic determinants (involving mainly vascular and coagulation components) and result in severe renal parenchymal damage (ascribed to the release of vasoactive or cytotoxic substances) (1). The other theory explains RCN as a permanent occlusion of afferent arterioles and interlobular arteries in the cortical vasculature, either by prolonged vasospasm, with secondary thrombosis, primary vascular damage with thrombosis, or some combination of both. However, neither the vasospastic nor vascular injury theory fully explains the localization of the process to the renal cortex.
Table 1.
Summary of renal cortical necrosis
| Category | Description |
|---|---|
| Etiology | Pregnancy, sepsis, trauma, toxins, pancreatitis, snakebites, drug-induced toxicity |
| Incidence | Rare |
| Gender ratio | Predominantly female (mostly pregnancy-related cases) |
| Age predilection | Second and third decade |
| Risk factors | Hypotension, advanced age |
| Treatment | Dialysis, intensive care |
| Prognosis | High mortality and morbidity |
| Imaging findings | CT: characteristic finding is the lack of renal cortical enhancement apart from a thin rim of viable tissue in the subcapsular, juxtamedullary areas, and in the medulla |
Acute RCN must be differentiated from acute tubular necrosis and renal arterial thromboembolism or occlusion. See Table 2 for details on each condition.
Table 2.
Differential diagnosis considerations for renal cortical necrosis
| Diagnosis | Notes |
|---|---|
| Renal cortical necrosis | CT scans show the lack of renal cortical enhancement apart from a thin rim of viable tissue in the subcapsular, juxtamedullary areas, and in the medulla. Renal arteries are patent. |
| Renal arterial occlusion | CT scan in the arterial phase shows occlusion of renal arteries and nephrographic defects in the peripheral renal cortex. |
| Renal arterial thromboembolism | CT scan shows wedge-shaped defects in the renal cortex. |
| Renal tubular necrosis | Kidneys have a mottled appearance containing multiple areas of high-density striations ("striated nephrogram"). |
Renal biopsy has been considered the gold standard for diagnosis. However, percutaneous renal biopsy is occasionally not possible due to a patient's unstable condition or persistent abnormal clotting. The diagnosis is best made by CT scan, especially during the initial phase of the disease.
No specific therapy has been shown to be effective in acute RCN. Patients require intensive care and dialysis to compensate for the function of their kidneys. Although these medications help, the prognosis for patients with RCN is poor.
| Symptoms and findings | |
|---|---|
| Renal cortical necrosis | CT scans show the lack of renal cortical enhancement apart from a thin rim of viable tissue in the subcapsular, juxtamedullary areas, and in the medulla. Renal arteries are patent. |
| Renal arterial occlusion | CT scan in the arterial phase shows occlusion of renal arteries and nephrographic defects in the peripheral renal cortex. |
| Renal arterial thromboembolism | CT scan shows wedge-shaped defects in the renal cortex. |
| Renal tubular necrosis | Kidneys have a mottled appearance containing multiple areas of high-density striations ("striated nephrogram"). |
References
- 1.Matlin RA, Gary NE. Acute cortical necrosis:case report and review of the literature. Am J Med. 1974;56:110–118. doi: 10.1016/0002-9343(74)90756-6. [PubMed] [DOI] [PubMed] [Google Scholar]
- 2.Oram S, Ross G, Pell L, Winteler J. Renal cortical calcification after snake bite. Br Med J. 1963;1:1647–1648. doi: 10.1136/bmj.1.5346.1642-a. [PubMed] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Van Geet C, Proesmans W, Arnout J, Vermylen J, Declerck PJ. Activation of both coagulation and fibrinolysis in childhood hemolytic uremic syndrome. Kidney Int. 1998;54:1324–1330. doi: 10.1046/j.1523-1755.1998.00103.x. [PubMed] [DOI] [PubMed] [Google Scholar]
- 4.Campbell AC, Henderson JL. Symmetrical cortical necrosis of kidneys in infancy and childhood. Arch Dis Childhood. 1949;24:269–285. doi: 10.1136/adc.24.120.269. [PubMed] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Groshong TD, Taylor AA, Nolph KD, Esterly J, Maher JF. Renal function following cortical necrosis in childhood. J Pediatr. 1971;79:267–275. doi: 10.1016/s0022-3476(71)80112-9. [PubMed] [DOI] [PubMed] [Google Scholar]
- 6.Palapattu GS, Barbaric Z, Rajfer J. Acute bilateral cortical necrosis as a cause of post operative renal failure. Urology. 2001;58:281–282. doi: 10.1016/s0090-4295(01)01146-3. [PubMed] [DOI] [PubMed] [Google Scholar]
- 7.Prakash J, Tripathi K, Pandey LK, Gadela SR, Usha Renal cortical necrosis in pregnancy-related acute renal failure. J Indian Med Assoc. 1996;94:227–229. [PubMed] [PubMed] [Google Scholar]
- 8.Chugh KS, Singhal PC, Sharma BK, Pal Y, Mathew MT, Dhall K. Acute renal failure of obstetric origin. Obstet Gynecol. 1976;48:642–646. [PubMed] [PubMed] [Google Scholar]
- 9.Madias NE, Harrington JT. Postischemic acute renal failure. In: Brenner FM, Lazarus JM, editors. Acute renal failure. W.B. Saunders; Philadelphia: 1983. pp. 235–251. [Google Scholar]