

Abstract
Continuous surveillance of local antimicrobial susceptibility patterns is a must for combating emerging antimicrobial resistance. WHONET is an effective computerized microbiology laboratory data management and analysis program that can provide guidance for empiric therapy of infections, alert clinicians of trends of antimicrobial resistance, guide drug-policy decisions and preventive measures. The program facilitates sharing of data amongst different hospitals by putting each laboratory data into a common code and file format, which can be merged for national or global collaboration of antimicrobial resistance surveillance. The system can be implemented in hospital laboratories of Armed Forces at no additional cost. Cumulative analysis of surveillance data obtained from various hospitals of Armed Forces at higher centers may help in formulating health policies and control measures at various levels.
Key Words: Antimicrobial susceptibility, Surveillance, WHONET
Introduction
Antimicrobial resistance is a growing threat of global magnitude largely attributed to the extensive and often unregulated use of antibiotics. It is widely held that surveillance of antimicrobial susceptibility is fundamental to combat the emergence of resistance [1]. Susceptibility data obtained from clinical microbiology laboratory helps to formulate antibiotic policy of the hospital. The data is to be analyzed and compared periodically to monitor changes in resistance rates, detecting the emergence of new resistance traits and to measure the impact of any interventions. Further, this data can be shared between different centers at the regional, national and global levels to assess the magnitude of the resistance and for implementation of control measures.
Susceptibility test results of microbiology laboratories of Armed Forces are generally stored in registers, paper files or in computer files, which makes the task of data analysis and comparison difficult. Under Hospital Automation Plan of Armed Forces, all laboratories have been equipped with personal computers with many of them having access to networking. There is a need of computerized surveillance system to effectively use the susceptibility data generated in these laboratories. The aim of present article is to bring awareness amongst pathologists, clinicians and infection control workers about a user-friendly software for the management of microbiology laboratory data which can also be merged into regional, national and global networks for surveillance of drug resistance.
The Surveillance System
WHONET is a windows based database software package for the management of microbiology laboratory data and the analysis of antimicrobial susceptibility test results. Current version WHO5.5 can be downloaded from the internet free of charge from URL (www.who.int/drugresistance/whonetsoftware). The software can be installed easily on a personal computers. If the laboratory is already using a computerized reporting system, data conversion can be accomplished with BACLINK software, also available free of charge from WHO. The data structure is compatible with major database, spreadsheet, and statistical software programs [2]. WHONET is also being used worldwide for research studies. It has three main parts, a laboratory configuration file which can be used to customize it to the particular laboratory, an interface for data entry and a part for analysis and reporting of resistance data.
Laboratory Configuration
This program permits the user to enter and modify laboratory-specific information such as patient-care areas (OPDs or wards), selection of antibiotic panels and interpretive breakpoints for various antibiotics. In addition, one can also indicate what data fields one want included in the data files. This configuration can be modified subsequently.
Data Entry
The program supports routine entry of susceptibility test results performed by disk diffusion, MIC, and/or E-test. The majority of laboratories in the Armed forces use comparative disc diffusion techniques based on Stokes or Kirby Bauer method to determine antibiotic sensitivity. The results can be recorded as interpreted values i.e. “R” (Resistant), “I” (Intermediate) and “S” (Sensitive) or as inhibition zone diameter. Interpretation guidelines for most standardized testing methodologies are built into the system. In addition the program also permits retrieval and correction of clinical records.
WHONET has a number of “expert rules” for modifying the interpretation of susceptibility test results. For example in the case of methicillin or oxacillin resistant staphylococci (MRSA), software can change the interpretation for all beta-lactam antibiotics to resistant. It has approximately 190 pre-defined “expert rules” for alerting microbiologists and infection control staff of unlikely, unusual, and important findings. The user may also define their own “user-defined alerts”.
The authors have used this software in a subzonal and a tertiary care hospital of Armed Forces and in our experience it takes only ten to twenty minutes to enter daily susceptibility reports in the system. However, data entry can also be done at a later point of time. Further, the data can be used to generate printout of clinical reports (Fig. 1). The user may indicate which antibiotics should be included in the clinical report. The user may also specify “first-line antibiotics”, “second-line antibiotics”, and “do not print” antibiotics.
Fig. 1.
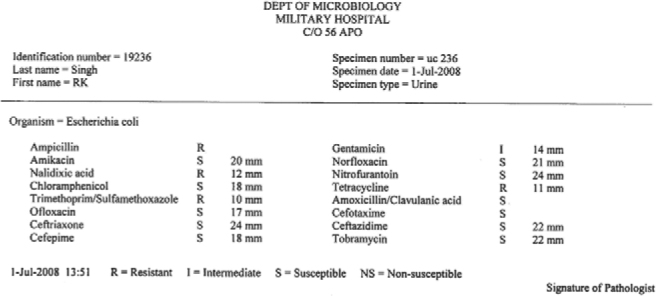
Printout of microbiology report
Data Analysis
The most attractive feature of WHONET is the ability to analyze stored data. The program has a modular configuration that allows customization of software for clinical, epidemiological, and infection control applications. From a single screen, a WHONET user can select the type of analysis to run, the species of bacteria to analyze, the subsets of isolates to include (e.g., all, isolates from urine only, and isolates resistant to gentamicin and from certain locations), and the antimicrobial agents and period to examine (Fig. 2). Type of analysis include percentage of data categorized as resistant, intermediate, or susceptible by standard or other breakpoints; distributions of test measurements (zone diameter, minimal inhibitory concentration) in the form of histograms, scatterplots and regression curves besides comparing measurements for different agents or methods for the same isolates. Line listings of isolates grouped by combinations of agents to which they are resistant (antibiotypes) to trace distinctive strains alongwith automated screening of data for unusual isolates can be done.
Fig. 2.
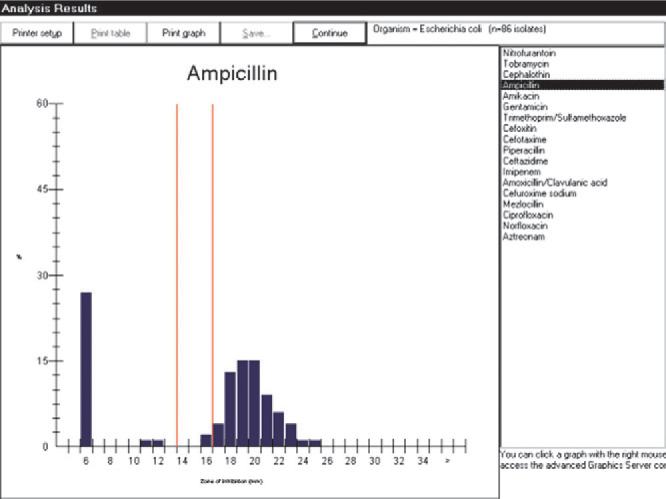
The Analysis Results screen
Data Sharing
Although test results are entered and monitored locally on software configured for a particular hospital laboratory, they are filed in a universal file format so that any copy of the program can analyze the files of any laboratory [3]. This feature may help to set up passive antibiotic susceptibility surveillance systems in Armed Forces by pooling and analyzing the data files from various peripheral and zonal hospitals at higher centers. Analysis of cumulative data at national level may help in reassessing the PVMS antibiotic formulary and implementation of various control measures.
Limitations
While the WHONET program is excellent for entry, analysis and reporting of resistant data, the software is not intended to function as a complete patient management system. In hospitals with patient management systems already installed, susceptibility data has to be entered separately into WHONET. Also in laboratories where the management of patients’ laboratory tests (i.e. receipt of specimens and laboratory forms, inscription in registers, return of test results, etcetera) is handled manually via register-books, the data must be punched into WHONET by hand. This would require additional trained manpower for data entry and analysis. Although the program performs its task very well, in a long-term perspective, a surveillance system that is integrated with a patient management system might be more sustainable [4].
Conclusion
WHONET is an effective tool which help not only in routine microbiology laboratory data management but also generate valuable information about antimicrobial susceptibility patterns over a place or time to provide the basis for and assess the effectiveness of prevention programs and policy decisions. The system can be implemented in hospital laboratories of Armed Forces at no additional cost.
Conflicts of Interest
None identified
ATTENTION SUBSCRIBERS.
Subscription rates for MJAFI are :-
| ATTENTION SUBSCRIBERS | ||
| Subscription rates for MJAFI are :- | ||
| (i) | Serving AMC/AD Corps officers (through AFMS (O)) | - Rs. 300/- per year |
| (ii) | Life Membership (Initial for five years) Renewal after five years | - Rs. 1500/- |
| - Rs. 500/- | ||
| (iii) | Annual subscription (Individual) | - Rs. 300/- |
| (iv) | Annual subscription (Institutional) | - Rs. 500/- |
| (V) | Annual subscription (Foreign countries) | - US $ 120/- |
| Note | 1. Please make your cheques or bank drafts in favour of Medical Journal Armed Forces India, payable at Pune. For outstation cheques add Rs. 50/- as bank commission. | |
| 2. Intimate non-reciept of issue within three months from the month of publication. | ||
References
- 1.Stamm W, Grayson ML, Nicolle L, Powell M. WHO Global Strategy for Containment of Antimicrobial Resistance (Document no: WHO/CDS/CSR/DRS/2001.2) World Health Organization; Geneva: 2001. [Google Scholar]
- 2.WHONET 5.4 Update notes, June 2006. Available from http://www.who.int/drugresistance/whonetsoftware (Accessed 31 Jul 2008).
- 3.O'Brien TF, Stelling JM. WHONET: An information system for monitoring antimicrobial resistance. Emerg Infect Dis. 1995;1:66. doi: 10.3201/eid0102.950209. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Blomberg B, Mwakagile DS, Urassa WK, Maselle SY, Mashurano M, Digranes A. Surveillance of antimicrobial resistance at a tertiary hospital in Tanzania. BMC Public Health. 2004;4:45. doi: 10.1186/1471-2458-4-45. [DOI] [PMC free article] [PubMed] [Google Scholar]