

Introduction
Acoustic Schwannomas constitute 70-80% of cerebello-pontine angle (CP angle) tumors [1]. These tumors arise from the vestibular component of the eighth nerve [2]. The clinical presentation in these cases is usually with tinnitus followed by hearing loss [3]. They may later involve seventh, fifth and lower cranial nerves and cerebellar and brain stem compression syndromes, as the tumor grows. Hydrocephalus due to fourth ventricular distortion is a usual accompaniment of larger CP angle tumors. The surgical extirpation of these lesions was associated with a prohibitive mortality till the era of Harvey Cushing and Dandy [4], who brought down the surgical mortality from 70% to 15%. The morbidity of CP angle tumor surgery remained considerable with facial palsies, often compounded with the corneal anaesthesia due to fifth cranial nerve involvement resulting in corneal ulceration in addition to the cosmetic deformity. With refinements in technology, facial nerve conservation became a reality with many modern series claiming anatomical conservation of the facial nerve in upto 98% of cases and functional conservation in a large percentage of these cases [5]. Conservation of hearing is however rarely achieved even with all available technological innovations and monitoring techniques.
We present a case of acoustic schwannoma which presented atypically and in whom hearing could be partially conserved after resection by a retromastoid approach.
Case Report
A 35 year old male presented with features of prostatism. During urological evaluation, a radioisotope scan showed features suggestive of bony metastases, which prompted further workup including magnetic resonance imaging (MRI) of the head. Prostatic carcinoma was ruled out by further evaluation and the patient's dysuria subsided. However the MRI of the head revealed a right sided CP angle tumor which showed the characteristic ice cream cone appearance of a vestibular schwannoma (Fig. 1). It was confirmed clinically and later by audiometry where bone conduction (BC)20-40dB, and air conduction (AC) 30-50dB decibels of hearing loss was noted in the right ear. There was no feature of other cranial nerve, cerebellar or brainstem involvement clinically. There was no hydrocephalus.
Fig. 1.
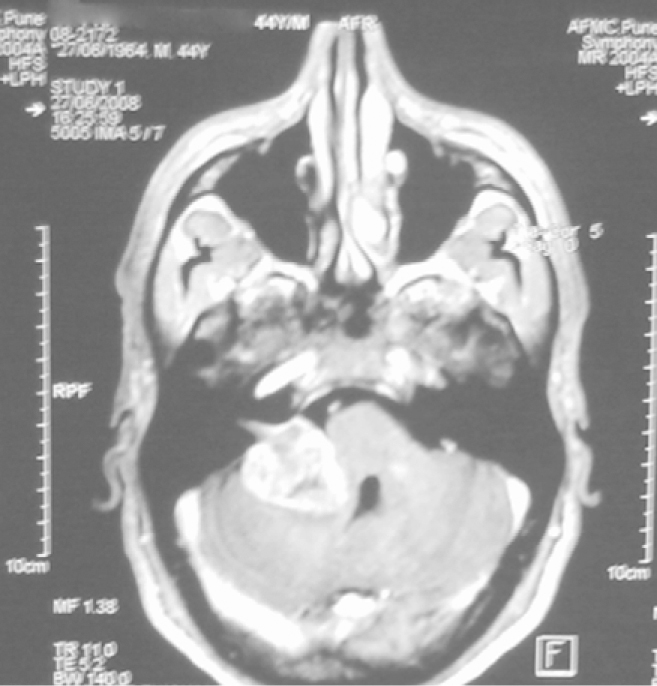
MRI of the head showing a right
The patient underwent CP angle exploration by the retromastoid approach. A yellowish 3.0 × 2.8 × 2.6 cms tumor of homogenous soft consistency was identified and surgically decompressed by a combination of intratumoral and arachnoidal plane dissection. The tumor was peeled off from the seventh-eighth nerve complex. The posterior lip of the internal auditory meatus was nibbled with a fine bone punch. The patient had an uneventful recovery from anaesthesia and surgery.
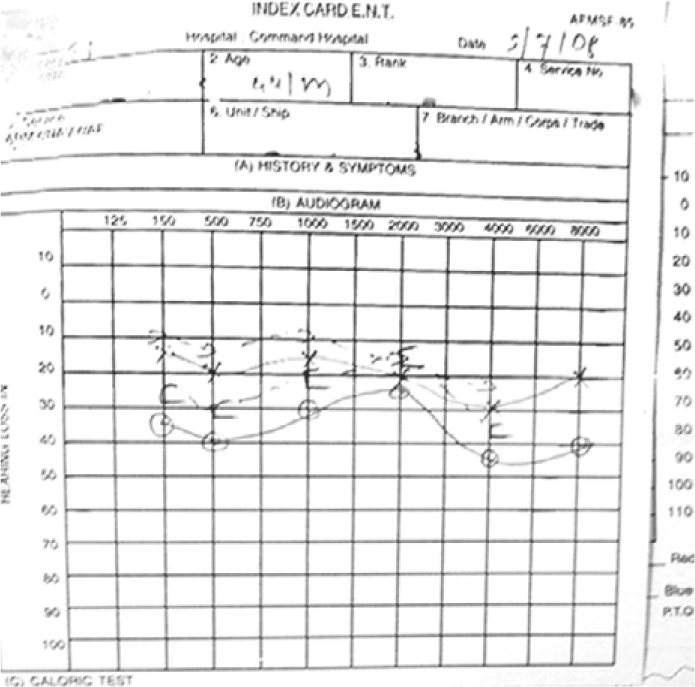
On post operative evaluation the facial nerve function was preserved (House and Brackman grade 1) (Fig. 3). Though hearing deteriorated after surgery, post operative audiogram (Fig. 4) shows functional conservation of cochlear function. Post operative computed tomography (CT) did not show evidence of gross residual tumor. Histopathological examination confirmed the tumor to be an acoustic schwannoma.
Fig. 3.

Post operative photograph of the patient
Fig. 4.
Post operative audiogram
Discussion
The cerebello-pontine angle is a space filled with cerebrospinal fluid. It has the brain stem for its medial border, the cerebellum as the roof and posterior wall and the petrous temporal bone as the lateral boundary. Containing the fifth to tenth cranial nerves and important vascular structures including the anterior inferior cerebellar artery and the petrosal vein of Dandy, the intricate surgical anatomy and the potential arachnoidal corridors make this area surgically challenging. The vast majority of vestibular schwannomas arise from the Schwann cell envelope of the superior or inferior divisions of the vestibulocochlear complex. Because the cerebello- pontine angle is relatively empty, tumors grow upto 3 cms before they come into contact with vital structures and nerves. Unilateral sensorineural hearing loss predominantly involving the higher frequencies is the commonest clinical presentation. This occurs due to direct injury to the cochlear nerve or due to interruption of the nerve's blood supply. About 10% of patients with acoustic schwannomas have useful hearing in the affected ear. Hearing conservation is rarely achieved in tumors larger than 2 cms in diameter [1].
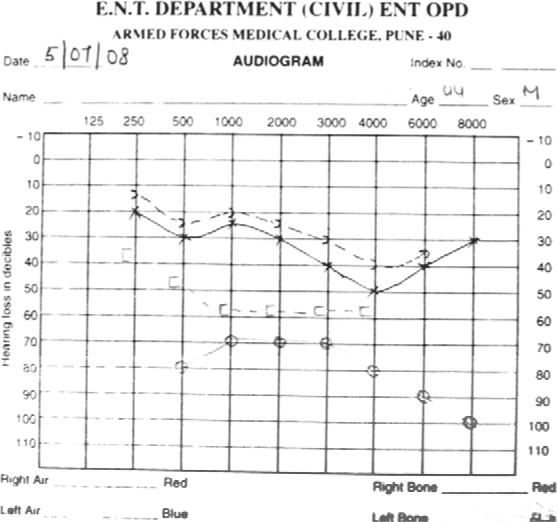
Fig. 2.
Preoperative audiogram sided CP angle tumor
Pathologically these tumors consist of spindle cells which may be arranged in orderly palisades (Antoni A) or in disorganised whorls (Antoni B). The treatment options for acoustic neuromas vary from observation in elderly induviduals with small tumors, to radio surgery and surgical excision [2].
Surgical access to the CP angle can be from the retromastoid corridor, by a translabyrinthine approach or by a middle cranial fossa route. The middle cranial fossa approach is most conducive to hearing preservation and large series where hearing preservation has been achieved in tumors smaller than 2 cms have been published [3].
Hearing conservation with tumours larger than 3 cms, from a retromastoid approach has been rarely reported [4]. Indeed, one of the so called advantages of gamma knife surgery is the potential for hearing preservation [5]. This patient had a medially located tumor. This and the soft nature of the tumor contributed to conservation of both the facial and acoustic components of the 8th nerve complex.
Conflicts of Interest
None identified
References
- 1.Resenberg SI. Natural history of acoustic neuromas. Laryngoscope. 2000;110:497–508. doi: 10.1097/00005537-200004000-00002. [DOI] [PubMed] [Google Scholar]
- 2.Snyder WE, Pritz MB, Smith RR. Suboccipital resection of a medial acoustic neuroma with hearing preservation. Surg Neuro. 1999:51. doi: 10.1016/s0090-3019(97)00528-4. [DOI] [PubMed] [Google Scholar]
- 3.Briggs RJS, Fabiny G, Kaye AH. Management of acoustic neuromas, review of surgical approaches & outcomes. J clin Neurosci. 2000;7:512–526. doi: 10.1054/jocn.2000.0728. [DOI] [PubMed] [Google Scholar]
- 4.Moffat DA, Gug MJ, Baguley DM. Hearing preservation in solitary vertibular schawannoma surgery using the retromastoid approach. Otolaryngol Head Neck surg. 1999;121:781–788. doi: 10.1053/hn.1999.v121.a91263. [DOI] [PubMed] [Google Scholar]
- 5.Kondziolka D, Lunsford LD, Flichinges JC. Acoustic radio surgery. Origins, contemporary use & future expectations. Neuro chirurgie. 2004;50:427–435. [PubMed] [Google Scholar]