

Introduction
Appendectomy is a common surgery and incisional hernia following appendectomy is uncommon, occurring in less than 0.12% of patients [1]. Post appendectomy interstitial incisional hernia is extremely rare [2].
In 1911, Hoguet first called attention to the occurrence of right inguinal hernia following appendectomy with drained wounds. Many of these had not only a right inguinal hernia but also an associated postoperative hernia at the site of the appendectomy scar. Hoguet and Watson attributed the occurrence of the inguinal hernia to a weakening of the abdominal wall following injury to the ilio-inguinal and ilio-hypogastric nerves [3].
A case of post appendectomy interstitial hernia is reported for the rarity of the condition and review of literature.
Case Report
A 32 year old male presented with pain and a bulge in the right lower quadrant of abdomen of three years duration. He had undergone an appendectomy for perforated appendicitis three years back. The postoperative period was complicated by surgical site infection which was managed conservatively. The bulge was visible only on standing and the pain aggravated on doing strenuous activity. There were no associated bowel symptoms. Physical examination revealed a well-healed appendectomy scar with a diffuse swelling visible centered over the scar on standing (Fig. 1). This bulge increased in size on coughing and disappeared on lying down. The muscular tone of the rest of the abdomen was good. Ultrasound examination of the abdomen showed a hernial sac containing bowel just under the scar; under the cover of the external oblique (Fig. 2). A diagnosis of post appendectomy interstitial incisional hernia was made and the patient was scheduled for surgery.
Fig. 1.

Pre-operative photograph of patient showing the hernial bulge centered over the appendectomy scar.
Fig. 2.

Pre-operative ultrasound image showing the interstitial incisional hernial sac (red arrows) under the cover of external oblique (green arrows, M1). M: Internal oblique muscle, B: Bowel loop, C: Campers fascia.
A 5 cm transverse incision was made starting from the scar in its upper part and extending medially. The external oblique aponeurosis was divided in the line of incision. The attenuated internal oblique fibres were split to reveal the hernial sac containing bowel (Fig. 3). The hernial sac was dissected from its place between external and internal oblique muscles and reduced. Preperitoneal space was then developed and a 15×15 cm mesh placed. The muscles were closed over it with 1-0 vicryl. The external oblique aponeurosis was sutured with 1-0 prolene.
Fig. 3.
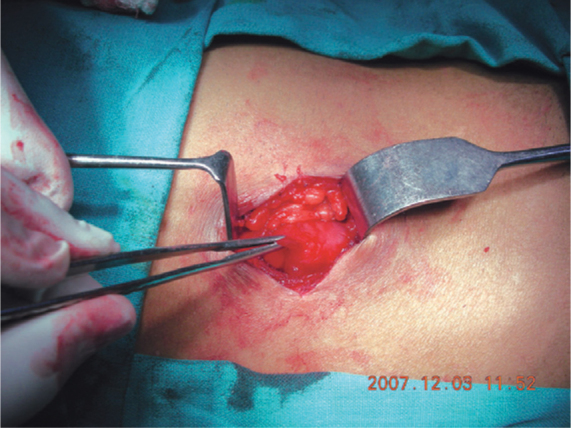
Per-operative photograph showing the hernial sac after division of the external oblique aponeurosis.
The postoperative course was uneventful. He was discharged on the 10th post operative day after suture removal. He was reviewed at one and six months after surgery wherein he was asymptomatic, without recurrence of hernia (Fig. 4).
Fig. 4.

Ultrasound image at six months (post operative) shows no recurrence. M: Muscle.
Discussion
Despite developments in surgical techniques, operative devices and materials, incisional hernia remains a significant problem in abdominal surgery [4]. The reported incidence of incisional hernias following abdominal surgeries is about 10 % [5]. Abdominal wall defects occur within the first 5 years after the surgical incision is made, but many develop later [6]. The incidence depends on a number of factors including patient factors like old age, male sex, obesity, smoking, diabetes, steroid use and some surgical factors like emergency surgery, bowel surgery, suture type and technique, chest infection, abdominal distension and wound infection. In our case, the contributing factors were male sex, emergency surgery and post-operative wound infection.
Hernia following appendectomy through a gridiron muscle-splitting incision is usually the result of infection of wound in advanced appendicitis, with or without perforation, and is associated with local purulent peritonitis [7]. Other common causes are placing a drain through the incision and tying sutures too tightly in the fleshy internal oblique and transverse abdominis muscles leading to necrosis of the muscle [2].
Two types of hernias occur. In the more common type, the hernia passes through all the layers of the abdominal wall. Less common is the interstitial type in which the hernia passes through a defect in the transverses abdominis and internal oblique muscles, but not through the intact aponeurosis of the external oblique [2]. This type can be missed easily. In patients suspected of this condition, ultrasound scanning or computed tomography should confirm the diagnosis [8].
Repair of post appendectomy incisional hernias can be undertaken in the form of anatomical repair. When the tissues are thin and atrophic, an overlap type of repair may be used for the two inner muscles but these cases are best treated with a sheet of polypropylene mesh, with a margin measuring at least 6-8 cm beyond the periphery of the defect, placed between the peritoneum and transverses abdominis muscle [9]. In our case, the patient underwent a pre-peritoneal mesh repair because of the attenuated tissues.
This case assumes significance since it is the rare interstitial type of post appendectomy incisional hernia, and not many cases find mention in review of literature.
Conflicts of Interest
None identified
References
- 1.Kostantakos AK, Zollinger RM., Jr Repair of Mc Burney incisional hernia after open appendicectomy. Current Surgery. 2000;57:79–80. doi: 10.1016/s0149-7944(00)00164-1. [DOI] [PubMed] [Google Scholar]
- 2.Abrahamson J. Hernias. In: Zinner MJ, Schwartz SI, Ellis H, editors. Maingot's Abdominal Operations. 10th ed. Appleton & Lange; Connecticut: 1997. pp. 479–580. [Google Scholar]
- 3.Fisher HC. Post appendicectomy Interstitial Inguinal Hernia. Ann Surg. 1946;123:419–426. [PubMed] [Google Scholar]
- 4.Feliciano DV. Incisional hernias as emergencies. In: Bendavid R, Abrahamson J, Arregui M, Flament JB, Phillips ED, editors. Emergency surgery. Abdominal wall hernias. Springer-Verlag Inc; New York: 2001. pp. 582–587. [Google Scholar]
- 5.Popovic JR, Hall MJ. 1999 National hospital discharge survey. Adv Data. 2001;3:1–20. [PubMed] [Google Scholar]
- 6.Chowbey PK, Sharma A, Mehrotra M, Khullar R, Soni V, Baijal M. Laparoscopic repair of ventral/incisional hernias. J Min Access Surg. 2006;2:192–198. doi: 10.4103/0972-9941.27737. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Abou-Nukta F, Bakhos C, Arroyo K. Effects of delaying appendectomy for acute appendicitis for 12 to 24 hours. Arch Surg. 2006;141:504–506. doi: 10.1001/archsurg.141.5.504. [DOI] [PubMed] [Google Scholar]
- 8.Toms AP, Dixon AK, Murphy JM, Jamieson NV. Illustrated review of new imaging techniques in the diagnosis of abdominal wall hernias. Br J Surj. 1999;86:1243–1249. doi: 10.1046/j.1365-2168.1999.01211.x. [DOI] [PubMed] [Google Scholar]
- 9.Duce AM, Lozano O, Villeta R. Incisional hernia following appendectomy. Surgical experience. Hernia. 1998;4:169–171. [Google Scholar]