

Introduction
Airway foreign bodies continue to pose a diagnostic and therapeutic challenge for otolaryngologists. Most airway foreign body aspirations occur in patients below 15 years of age and 80-90% in children below five years of age. Vegetable matter especially peanuts, are the commonest bronchial foreign bodies. These foreign bodies become lodged in the bronchus because of their size and configuration which allows their passage through the larynx and trachea but not through the bronchi.
The usual presenting symptoms are choking, gagging followed by wheezing and respiratory distress. We report a case of bronchial foreign body with an unusual feature of subcutaneous emphysema.
Case Report
A five year old male child presented in an emergency room with complaints of respiratory distress, cough and swelling of the face of 12 hours duration. Clinical examination revealed that the child was febrile having temperature of 101° F, pulse rate was 110/minute and respiratory rate 56/minute. There was no stridor but accessory muscles of respiration were being used. He had diffuse swelling over the face, neck, suprasternal region and the chest. The swelling was soft, non tender and a definite crepitus was palpable. The examination of respiratory system revealed hyper resonance on left side of chest with tracheal shift to right. The air entry to left lung was reduced. Other systemic examination was normal. He was diagnosed as a case of pneumothorax (left) with subcutaneous surgical emphysema (Fig. 1). A water seal chest drain was placed and he was put on antibiotics.
Fig 1.
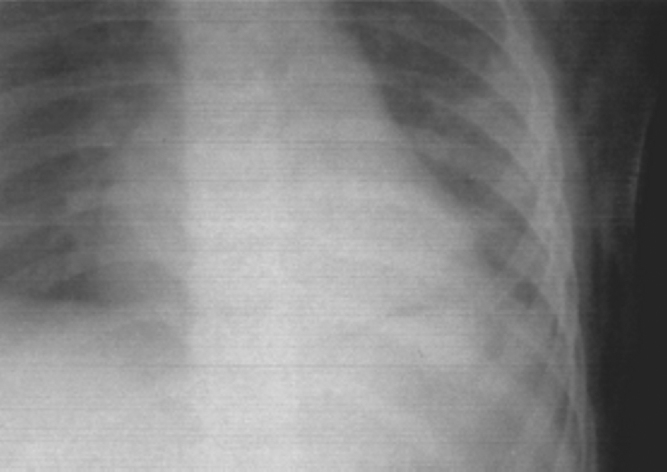
Shows subcutaneous emphysema
The rapid and sudden progression of symptoms and unusual presentation of surgical emphysema without any history of trauma suggested rupture of a hollow viscus. The child gave history of eating peanuts 7-10 days back which was followed by a bout of coughing. Thereafter he was asymptomatic until he presented with respiratory distress and emphysema. At this stage computed tomography (CT) scan of thorax was done which showed collapse of left lower lobe of lung with emphysematous expansion of left upper lobe. There was an apparent presence of intraluminal mass/ foreign body in left bronchus just beyond origin of left upper lobe bronchus (Fig. 2). The child was transferred to a referral hospital for further management. Emergency bronchoscopy at the referral hospital under general anaesthesia (GA) using rigid bronchoscope revealed pieces of vegetable foreign body (peanuts) in left main bronchus which were removed. Antibiotics and bronchodilators were continued. The patient showed good recovery and subcutaneous emphysema gradually subsided with normal lung expansion.
Fig 2.
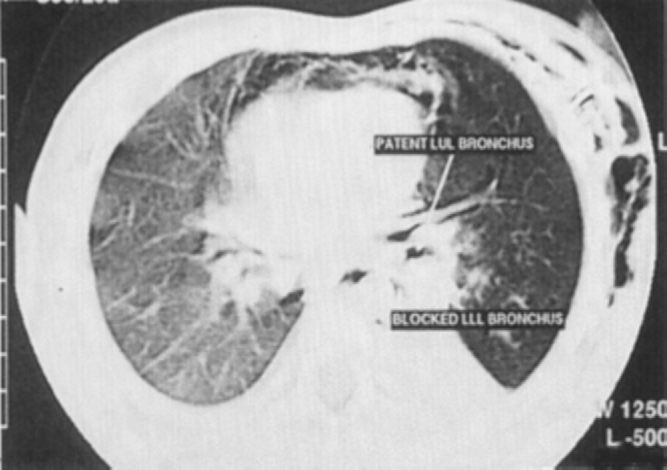
Shows blocked lower lobe bronchus (left)
Discussion
Foreign bodies in the bronchi are a common problem. These may be endogenous like blood, saliva or vomitus or exogenous of vegetable or non vegetable origin. Bronchial foreign bodies are common in children because they have difficulty in swallowing hard foodstuffs such as nuts and have an inadequately developed protective respiratory reflexes, which makes them vulnerable to inhalation of foreign bodies [1]. Foreign bodies are more common in the right bronchus due to lesser angle of divergence of right main bronchus from the tracheal axis. In children below five years of age, there is equal divergence of bronchi from tracheal axis, hence the incidence of foreign bodies is equal in both left and right bronchi [2]. In conscious patients inhalation of a foreign body is followed by choking, gagging and subsequently there may be a symptom free interval. Later cough, signs of pulmonary collapse and suppuration may follow. In case of vegetable foreign bodies ‘vegetal’ bronchitis immediately supervenes and the foreign body causes valvular obstruction. The valve effect can be of three types. A foreign body that obstructs the bronchus completely, leads to collapse of the distal lobe producing a stop valve effect, the foreign body which obstructs only on expiration causes a check valve type of effect which results in lobar emphysema and those causing obstruction both during both inspiration and expiration, produce bypass valve effect which present with features of bronchitis.
There have been very few reports in literature of bronchial foreign body presenting as subcutaneous surgical emphysema. Ramodan et al [3] and Valdorino et al [4], have both reported a single case of a two years old child who presented with pneumomediastinum and subcutaneous emphysema following foreign body aspiration. The exact mechanism of surgical emphysema is not known, but a possible explanation for this would be initial occurrence of lobar emphysema following check valve type of obstruction of left upper lobe bronchus. Increased pressure in the alveolus may have caused an air leak towards the mediastinum through the broncho vascular plane. As the mediastinal pressure increased, decompression would have occurred in subcutaneous and cervical spaces leading to subcutaneous emphysema [5]. Pleural rupture due to mediastinal emphysema may have resulted in pneumothorax. Merchant et al [1], have reported a large series of foreign bodies in the bronchus with varied presentations, yet there was none presenting with subcutaneous emphysema, even though 77 of their 132 cases had features of obstructive emphysema on chest radiography. They reported one death due to massive pneumothorax on the side of foreign body.
Findlay et al [6], have stated that pneumomediastinum is uncommon in paediatric practice outside the neonatal period, and asthma or respiratory infections are the commonest underlying causes, it is important to consider the possibility of foreign body aspiration in such cases.
Chapelon et al [7], reported a case of intra bronchial seed immigration where the aspirated particle after causing pneumonia, crossed the pleura and gave rise to a subcutaneous swelling. The commonest radiological finding is obstructive emphysema, however the chest radiograph may be normal in 20% cases[1]. Since emphysema is the commonest finding, inspiratory and expiratory films should be taken to demonstrate trapping of air [8]. Computed tomography (CT) plays an important role in localiastion of the forgein body and it's management.
Conflicts of Interest
None identified
References
- 1.Merchant SV. Foreign bodies in the bronchi. J Postgrad Med. 1984;20:219–223. [PubMed] [Google Scholar]
- 2.Hassan A. Changes in tracheobronchial angles as a function of age. Ind J Otolayngol H & N Surg. 2000;2:1–6. [Google Scholar]
- 3.Ramodan Management of an Unusual Presentation of Foreign Body Aspiration. J Laryngol Otol. 1992;106:751–752. doi: 10.1017/s0022215100120791. [DOI] [PubMed] [Google Scholar]
- 4.Valdorino M. A two year old child with acute respiratory difficulty. An Esp Pediatr. 1998;49:841–842. [PubMed] [Google Scholar]
- 5.Maunder RJ, Pierson DJ, Hudson LD. Subcutaneous and Mediastinal Emphysema, Pathophysiology, Diagnosis and Management. Arch Int Med. 1984;144:1447–1453. [PubMed] [Google Scholar]
- 6.Findlay CA, Morissey S, Paton JY. Subcutaneous emphysema secondary to Foreign Body Aspiration. J Paedtr Pulmonl. 2003;36:81. doi: 10.1002/ppul.10295. [DOI] [PubMed] [Google Scholar]
- 7.Chapelon C, Gudicelli J, Louis D, Andre C. Intrabronchial inhaled seed migration. Value of ultrasonography in the diagnosis of pleurocutaneous fistula. Rev Med respire. 2001;134:428–429. [PubMed] [Google Scholar]
- 8.Alan D, Murray M, Holinger L. Foreign Bodies of the airway and oesophagus. In: Cummings Charles W, Krause Charles, Schuler David., editors. Otoloaryngology Head and Neck Surgery. 3rd ed. Mosby; St Louis Missouri: 1998. pp. 377–384. [Google Scholar]