

Introduction
Intussusception is defined as invagination of one segment of the gastrointestinal tract into a subjacent one. It is the commonest cause of paediatric intestinal obstruction, where it is almost invariably idiopathic [1]. Heterotopic pancreas (HP) has been reported as an unusual cause of intestinal obstruction, with an estimated incidence of 0.2% of upper abdominal operations. HP occurs predominantly in the stomach, duodenum and proximal jejunum. Intussusception caused by ileal pancreatic heterotopia is rare [2].
We report the case of a nine year old boy with recurrent abdominal pain and acute bowel obstruction caused by an ileal intussusception secondary to heterotopic pancreas.
Case Report
A nine year old boy was brought with complaints of colicky, intense periumbilical abdominal pain of six hours duration and three episodes of non-projectile, bilious vomiting. The patient was managed conservatively by the paediatrician, but there was no relief and a surgical consultation was sought. On questioning, it was revealed that the child had been suffering from similar episodes in the last two months, which were managed conservatively with antispasmodic medication.
Clinical examination revealed exaggerated, occasionally high pitched bowel sounds mostly in the right side of abdomen. Plain erect abdominal radiograph revealed multiple air-fluid levels. Blood counts were normal. Ultrasound revealed a loop of abnormal bowel in the right iliac fossa. It contained concentric rings of high and low echogenicity, suggestive of a small bowel intussusception (Fig. 1).
Fig. 1.
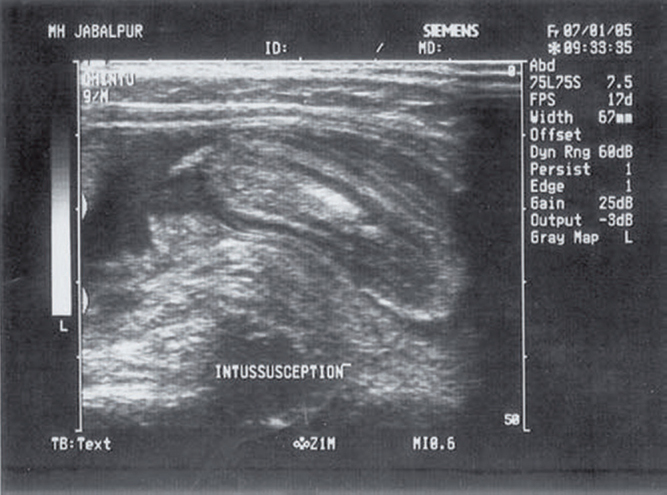
Ultrasonography shows concentric rings of variable echogenicity in right iliac fossa
Based on these findings, the boy was taken up for emergency laparotomy through a lower midline incision. There was a six centimeter segment of ileo-ileal intussusception with wet gangrene of the involved segment. Enterotomy revealed the presence of an ulcerated polyp measuring 30 × 30 × 10 mm, at the tip of the intussusceptum (Fig. 2). Gangrenous ileum including the intussusception was excised and primary end-to-end anastomosis performed. Subsequent postoperative recovery was uneventful and seven months later, the child remains asymptomatic.
Fig. 2.

Intussusception with wet gangrene and ulcerated polyp at intussusceptum
Histological examination of the ulcerated polyp revealed thick irregular strands of displaced smooth muscle tissue with embedded ductular, mucinous and pancreatic exocrine acinar tissue, suggestive of pancreatic heterotopia (Fig. 3).
Fig. 3.
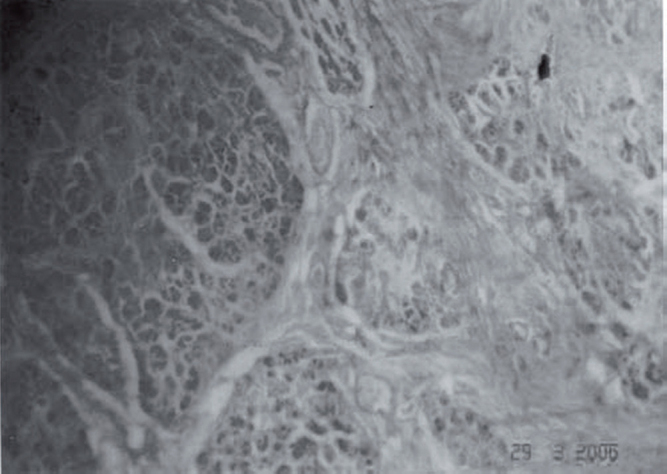
Histopathology showing embedded pancreatic acinar nests displacing smooth muscle
Discussion
Paediatric intestinal obstruction secondary to intussusception is usually idiopathic in origin [1]. Heterotopic pancreas is a rare entity commonly found incidentally during laparotomy or autopsy for another illness. It is usually found in the stomach or duodenum. Distal lesions are rare and the ileum is usually spared except in cases of Meckel's pancreatic heterotopia. Isolated ileal involvement is rare [2,3].
The pancreas is formed from several primitive endodermal evaginations of the duodenal wall. The dorsal diverticulum becomes the body and tail and the ventral portion, the head of the pancreas. Persistence of these evaginations elsewhere leads to heterotopia anywhere from the stomach (most common) to the jejunum or ileum (least common). In the latter, HP is usually associated with a Meckel's diverticulum.
Although there are conflicting reports in the literature, approximately half of cases of small bowel HP are asymptomatic. However only few cases become symptomatic. Dolan et al [4], have suggested that the significance for the nonspecific symptoms in HP is related to the size and mucosal relation of the pancreatic tissue. Lesions greater than 15 mm and closer to the mucosa are most likely to be symptomatic. Submucosal muscular wall proximity is hypothesized to aggravate bowel dysmotility. In our case there was chronicity in abdominal pain, as suggested by previous episodes, and this is possibly attributable to repeated inflammation and haemorrhagic necrosis of adjacent muscle.
Of prime importance, of course, is the relief of obstruction. If the intussusception is reducible, care must be taken to excise the entire incriminating suspect lesion in the intussusceptum, especially in the large bowel where the propensity of future malignancy is far greater.
Our case assumes special significance in the light of the fact that review of literature sparingly speaks of paediatric intussusception secondary to heterotopic pancreas and rarely with reference to ileal involvement.
Conflicts of Interest
None identified
References
- 1.Jacobz A, Nawaz A, Matta Hl, Salem Ahmed AI. Intussusception secondary to isolated heterotopic pancreas of the ileum: case report and review of the literature. Ann Saudi Med. 2002;22:3–4. doi: 10.5144/0256-4947.2002.213. [DOI] [PubMed] [Google Scholar]
- 2.Hamada Y, Yonekura Y, Tanano A. Isolated heterotopic pancreas causing intussusception. Eur J Pediatr Surg. 2000;10:197–200. doi: 10.1055/s-2008-1072357. [DOI] [PubMed] [Google Scholar]
- 3.Al-Zahem S, Arbuckle, Cohen R. Combined ileal heterotopic pancreatic and gastric tissues causing ileocolic intussusception in an infant. Pediatr Surg Int. 2006;22:297–299. doi: 10.1007/s00383-005-1566-7. [DOI] [PubMed] [Google Scholar]
- 4.Dolan RV, ReMine WH, Dockerty MB. The fate of heterotopic pancreatic tissue: A study of 212 cases. Arch Surg. 1974;109:762–765. doi: 10.1001/archsurg.1974.01360060032010. [DOI] [PubMed] [Google Scholar]