

Abstract
Eagle's syndrome, also known as an elongated styloid process, is a condition that may be the source of craniofacial and cervical pain. It is infrequently reported but is probably more common than generally considered. The symptoms related to Eagle's syndrome can be confused with those attributed to a wide variety of facial neuralgia and or oral, dental, and temporomandibular joint diseases. In this paper, there are two cases, which reported to the Department of Oral Medicine, Diagnosis, and Maxillofacial Radiology, with a chief complaint of radiating pain in the preauricular region of the face. After radiographic investigation, these cases are considered as a case of Eagle's syndrome because of increase in the size of the styloid process.
Keywords: Eagle's syndrome, ossification, stylohyoid ligament, styloid process
INTRODUCTION
The term “Eagle's syndrome” or “Stylohyoid syndrome” describes a series of symptoms caused by an elongated styloid process and/or the mineralization (ossification or calcification) of a part or the entire stylohyoid ligament. The styloid process is a bony projection, situated immediately anterior to the stylomastoid foramen. It is of cylindrical form and projects downward from the inferior surface of the temporal bone toward the front, downward, and medially narrowing toward the tip. The location of the tip is particularly important, which is situated between the internal and external carotid arteries, laterally from the pharyngeal wall and immediately behind the tonsillar fossa.[1] Eagle, an otorhinolaryngologist, first described Eagle's syndrome, also known as an elongated styloid process, in 1937. It occurs in around 4% of the general population although it is usually asymptomatic, with only 4% of patients presenting with symptoms. The normal length of the styloid process varies greatly between individuals, but in the majority of people it is 20–30 mm long. It is considered elongated when it is longer than 30 mm.[2] Eagle defined the length of a normal styloid process to be 2.5–3.0 cm. Various author estimated the normal length according to Kaufman et al. (1970) styloid process to be <3 cm, 1.52–4.77 cm according to Moffat et al. (1977), <2.5 cm according to Correl et al. (1979), 2–3 cm according to Lindeman (1985), Langlais et al. (1986), and Montalbetti et al. (1995), <4 cm according to Monsour and Young (1986), Balcioglu (2009) the mean length of the styloid processes of the subjects reporting Eagle's syndrome is reported to be 40 ± 4.72.
CASE REPORTS
Case 1
A female patient of age 60 years reported to the Department of Oral Medicine, Diagnosis, and Maxillofacial Radiology, with a chief complaint of pain in left preauricular and postauricular region since 6 months. The pain was continuous, dull in the preauricular and postauricular area and it radiates superiorly to head and inferiorly to symphysis and parasymphysis region. It aggravates during right and left movements of the jaw and cervical rotation she also complains of continuous pain in the throat and sensation of the foreign body in the pharynx and relieved after taking analgesics. Temporomandibular joint (TMJ) examination revealed bilateral synchronized movement with clicking sound and tenderness on the left side, and mouth opening was 35 mm. Intraoral examination revealed bony hard protuberance on palpation near tonsillar region. Based on clinical examination and history case was provisionally diagnosed as Eagle's syndrome (left side). The differential diagnosis for this case is TMJ dysfunction syndrome, Head pain, Myofascial pain dysfunction syndrome was put forward.
The patient was subjected for cone-beam computed tomography (CBCT) scan, and it was performed with CS9300 scanner. Right and left TMJ condylar heads were concavo-convex and plano-convex in shape, respectively, with intercondylar axis measuring appropriately 139°.
In the right TMJ [Figure 1a and b], there were mild flattening of the condylar head and diffuse marrow osteopenia in the sub-articular, cancelous regions of the condylar head and sub-condylar area. Glenoid fossa floor, preglenoid plane (posterior slope of articular eminence), and articular crest appeared intact. No obvious loose bodies or osteophytosis noted in sections through right TMJ. Above findings could represent early to mild right TMJ degenerative arthropathy. Mild asymmetric thickening of the right masseter muscle was noted at the level of inferior third of right ramus or close to right angle region of the mandible.
Figure 1.
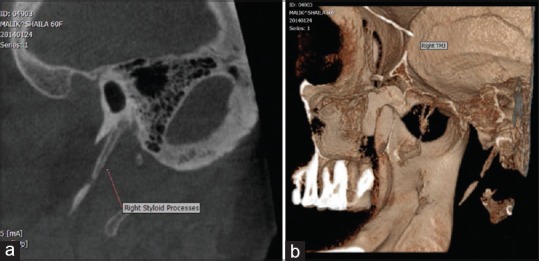
(a and b) Cone-beam computed tomography and three-dimensional computed tomography image of right temporomandibular joint there were mild flattening of condylar head and diffuse marrow osteopenia in the sub-articular, cancelous regions of condylar head and sub-condylar area. The right stylohyoid complex with maximum anteroposterior diameter approximately 2.1 mm, suggestive of Type E pattern of calcification according to MacDonald-Jankowski
In the Left TMJ, there was [Figure 2a and b] mild flattening of TMJ condylar head and small fine condensed and closely spaced trabeculae was noted in the cancelous region of the condylar head. TMJ glenoid fossa floor, preglenoid plane, and articular crest appear intact. No obvious loose bodies or osteophytosis noted in sections through left TMJ. These findings could represent early left TMJ degenerative changes.
Figure 2.
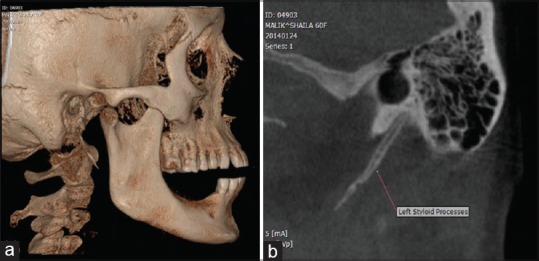
(a and b) Cone-beam computed tomography and three-dimensional computed tomography image of left temporomandibular joint there was mild flattening of temporomandibular joint condylar head and small fine condensed, closely spaced trabeculae were noted in the cancelous region of condylar head. The left stylohyoid complex with maximum anteroposterior diameter approximately 2.7 mm, suggestive of Type E pattern of calcification according to MacDonald-Jankowski
There was a mild elongation of the right and left styloid processes/calcified stylohyoid complexes, which measured approximately 32.8 mm in greatest cranio-caudal dimensions. There was contiguity of the tympanohyal, stylohyal regions of the right, and the left of the stylohyoid complex with a maximum anteroposterior diameter approximately 2.1 mm and 2.7 mm, respectively, the suggestive of Type E pattern of calcification according to MacDonald-Jankowski.
Correlating chief complaint, history, clinical examination, and investigation on final diagnosis of Eagle's syndrome (right and left side) were made. The patient was treated through conservative approach that is, steroid or lidocaine injection and tablet Nimulid-MR TDS for 5 days was given, and she was recalled after 7 days and advise for surgical excision of the styloid process and/or the mineralized ligaments.
Case 2
A male patient of age 50 years came to the department having a chief complaint of dull pain in right and left preauricular region, which radiates to the head and temporal region since 1-year. Pain is severe at the left preauricular region it aggravates during right and left movements of the jaw and relieved after taking analgesics since 1-year. TMJ examination revealed bilateral synchronized movement with clicking sound present and tenderness on the left side. Mouth opening was 40 mm. Based on the clinical examination and the history case were provisionally diagnosed as Eagle's syndrome (left side).
Panoramic image and TMJ transactional view [Figure 3a and b] revealed linear ossification extending forward from the region of the mastoid process and cross the posterior inferior aspect of the ramus toward the body of the mandible. The dimensions were measured with a caliper from the base to the apex, directly on the films. There were an elongation of the left and right styloid processes/calcified stylohyoid complexes, which measure approximately 65 and 60 mm, respectively, in greatest cranio-caudal dimensions and the suggestive of Type E pattern of calcification according to MacDonald-Jankowski. Correlating clinical examination and radiographic feature final diagnosis of Eagle's syndrome (left and right side) were made. The patient was advised for surgical excision of the styloid process and/or the mineralized ligaments.
Figure 3.
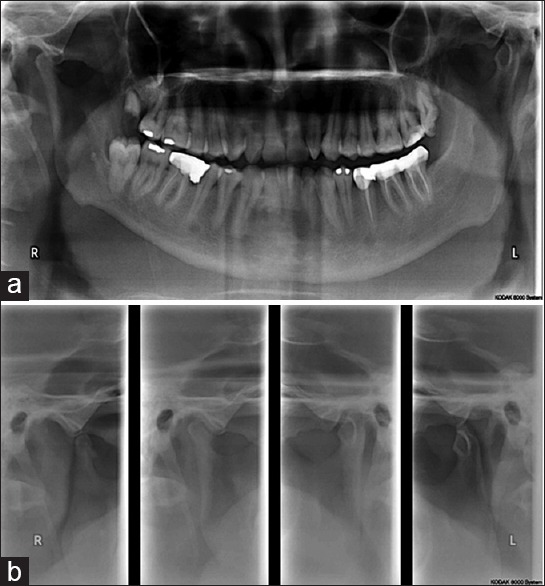
(a and b) Elongation of the left and right styloid processes/calcified stylohyoid complexes which measure approximately 65 and 60 mm, respectively, in greatest cranio-caudal dimensions and suggestive of Type E pattern of calcification according to MacDonald-Jankowski
DISCUSSION
Eagle's syndrome is defined as the symptomatic elongation of the styloid process or mineralization (ossification or calcification) of the stylohyoid ligament complex. From Eagle's early descriptions, patients were categorized into two groups: Those who had classical symptoms of a “foreign body” lodged in the throat with a palpable mass in the tonsillar region following tonsillectomy; and those with pain in the neck following the carotid artery distribution (carotid artery syndrome). Although these two types have a common etiology, their symptomatology differ.[1,3]
ETIOLOGY
The cause is considered to be a mystery (Massey and Massey, 1979; Quereshy et al., 2001; Dinkar and Amonkar, 2003; Sela et al., 2003). Steinmann (1968, 1970) proposed three different theories to explain such abnormal ossification.
A number of prevalent theories correlate anatomy, embryology, and physiology for a clear understanding of an elongated styloid process.
Theory of reactive hyperplasia suggests that if styloid process is appropriately stimulated by pharyngeal trauma, ossification may continue from its tip against stylohyoid ligament
Theory of anatomic variance suggests that styloid process and stylohyoid ligament are normally ossified, and elongation process is simply an anatomical variation
Dysendocrine theory suggests that anatomic variation may be transmitted as a genetic trait.[4] Some other theories state that persistence of cartilaginous analog of styloid may cause congenital elongation of styloid and calcification of the stylohyoid ligament by unknown mechanism and growth of osseous tissue at insertion of stylohyoid ligament may also cause its elongation.[5]
CLINICAL AND RADIOGRAPHIC PRESENTATION
Clinically, the syndrome is most commonly seen after 30 years of age. There is no significant sex predilection however symptoms are more common in females. In Eagle's syndrome, the symptoms range from mild discomfort to acute neurologic and referred pain.
These symptoms may include continuous pain in the throat even after tonsillectomy (40%), sensation of a foreign body in the pharynx (55%), dysphagia, otalgia, headache, pain along the distribution of the external and internal carotid arteries, pain on cervical rotation, facial pain, vertigo, and syncope.[6] The symptoms are characterized by pain located in the areas where the fifth, seventh, eighth, ninth, and tenth cranial nerves are distributed pain following tonsillectomy is presumably created by stretching or compressing the nerve or nerve endings of cranial nerves.
According to Pattern of calcification Langlais et al., classified three types of radiographic appearance and four patterns of calcification or mineralization.[7]
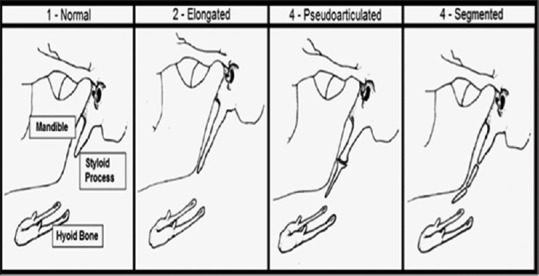
Type 1: Elongated – The radiographic appearance of this type of mineralized complex is characteristic by an uninterrupted integrity of the styloid process. The normal reported length of the styloid process ranges from 25 to 32 mm. He has accepted the normal length of 25 mm for most radiographic projection. However, if the panoramic films are studied, measurement to 28 mm may be considered within the normal range because of the inherent magnification in the most radiographs
Type 2: Pseudoarticulated – The styloid process is apparently joined to the mineralized stylohyoid or stylomandibular ligament by a single pseudoarticulated, which is usually located superior to a level tangential to the inferior border of the mandible
Type 3: Segmented – It consist of either short or long noncontinuous portions of the styloid process or interrupted segments are seen with interruptions either above or below the level of the inferior border of the mandible, or both. The overall appearance is one of the segmented mineralized stylohyoid complexes.
According to MacDonald-Jankowski the pattern of calcification was described according to the center of calcification involved; Region 1, tympanohyal; Region 2, stylohyal; Region 3, ceratohyal; Region 4, hypohyal [Figure 4]. The 12 patterns are derived from the pattern of calcification in the regions and whether the regions were continuous or distinct. The presence of the lesser horn of the hyoid bone was not recorded. Symmetry was determined by reference to the pattern based on the four regions. In those cases where asymmetry was present, the pattern that was most advanced was taken to define the pattern for that patient. The terms used in this report were defined as follows: Calcification was “normal” where it did not extend below the mandibular foramen (Patterns A to D). A normal styloid process was considered “classical” where it presented as a continuous radiopacity composed or Regions 1 and 2 (Pattern D). An “elongated styloid process” was defined as extending below the mandibular foramen (Pattern E). Calcification of the stylohyoid ligament was defined as occurring when calcification, which extended below the mandibular foramen did not appear to be continuous with the base of the skull (Patterns F to K).[8]
Figure 4.
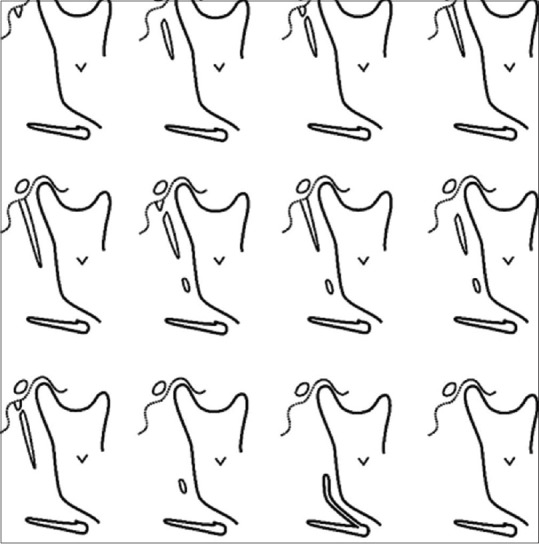
The pattern of calcification according to MacDonald-Jankowski (2001)
According to O’Carroll and Jackson classification [Figure 5] 17 of styloid process calcifications to create a classification model for grading the styloid process calcifications (SLC): (a) Type 1, SLC is higher than mandibular foramen (bilateral); (b) Type 2, SLC is aligned with mandibular foramen (bilateral); (c) Type 3, SLC is lower than mandibular foramen (bilateral); and (d) Type 4, SLC has different lengths for the left and the right sides of the patient (including all unilateral calcifications). The most useful imaging techniques that can demonstrate the styloid process include panoramic radiography, postero-anterior skull view, lateral cephalogram, lateral oblique mandible view, Towne's view, CT, and magnetic resonance scanning. However, it is not always possible to identify the different types of styloid processes on panoramic radiographs, as they are masked by other structures. Panoramic examination shows that the length of the styloid process varies owing to discrepancies of the panoramic units, usage, as well as patient positioning. Overlapping might occur posteriorly by the upper cervical vertebrae, and anteriorly by the mandible. Furthermore, misdiagnoses might also occur.[9]
Figure 5.
The pattern of calcification according to O’Carroll and Jackson (1979)
DIAGNOSIS AND TREATMENT
The diagnosis is based on the history of previous tonsillectomy or trauma to the cervical spine in conjunction with reproduction of symptoms during palpation of the tonsillar fossa. The elongated styloid process can be palpated by inserting a finger orally along the occlusal line posterior to the region of the tonsillar fossa. Pain is reproduced by palpation of the styloid process. Confirmation is made with radiographs showing an elongated styloid process or mineralization of the stylohyoid complex.
The carotid artery syndrome is usually not associated with a tonsillectomy. It is caused by mechanical irritation of the sympathetic nerve tissue in the walls of the internal and/or external carotid artery by the tip of the styloid process or the ossified ligament. This irritation produces referred pain in the respective area of vascularization. Hence, if the external carotid artery is affected, the patient may complain of pain in the neck on turning the head, or pain radiation to the eye, ear, angle of the mandible, soft palate, and nose. When the internal carotid artery is involved, pain over the entire head and larynx may be involved. Treatment has traditionally been surgical excision of the styloid process and/or the mineralized ligaments. However, a more conservative approach has been to attempt to decrease any muscle spasm and scar tissue around the styloid process and mineralized ligaments. However, failing this attempt, surgery remains a viable alternative. Other treatments have concentrated on steroid injections into the affected tissues with varying results.[10]
CONCLUSION
In patients presenting with a region headache or facial pain, thorough, detailed case history and physical examination of the head and neck are mandatory. The differential diagnosis of neoplasm, unerupted molars, temporomandibular dysfunction, inner ear problems, and neuralgias should be included with an elongated styloid process as sources of head and neck pain. The diagnosis of Eagle's syndrome is made with a history and finding of an elongated styloid process in the tonsillar fossa, of which palpation reproduces the symptomatology.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Kaufman SM, Elzay RP, Irish EF. Styloid process variation. Radiologic and clinical study. Arch Otolaryngol. 1970;91:460–3. doi: 10.1001/archotol.1970.00770040654013. [DOI] [PubMed] [Google Scholar]
- 2.Ilgüy M, Ilgüy D, Güler N, Bayirli G. Incidence of the type and calcification patterns in patients with elongated styloid process. J Int Med Res. 2005;33:96–102. doi: 10.1177/147323000503300110. [DOI] [PubMed] [Google Scholar]
- 3.Kim JE, Min JH, Park HR, Choi BR, Choi JW, Huh KH. Severe calcified stylohyoid complex in twins: A case report. Imaging Sci Dent. 2012;42:95–7. doi: 10.5624/isd.2012.42.2.95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Piagkou M, Anagnostopoulou S, Kouladouros K, Piagkos G. Eagle's syndrome: A review of the literature. Clin Anat. 2009;22:545–58. doi: 10.1002/ca.20804. [DOI] [PubMed] [Google Scholar]
- 5.Murtagh RD, Caracciolo JT, Fernandez G. CT findings associated with Eagle syndrome. AJNR Am J Neuroradiol. 2001;22:1401–2. [PMC free article] [PubMed] [Google Scholar]
- 6.Lahori M, Agrawal P. Eagle's syndrome. Guident. 2012;5:22–5. [Google Scholar]
- 7.Langlais RP, Miles DA, Van Dis ML. Elongated and mineralized stylohyoid ligament complex: A proposed classification and report of a case of Eagle's syndrome. Oral Surg Oral Med Oral Pathol. 1986;61:527–32. doi: 10.1016/0030-4220(86)90400-7. [DOI] [PubMed] [Google Scholar]
- 8.MacDonald-Jankowski DS. Calcification of the stylohyoid complex in Londoners and Hong Kong Chinese. Dentomaxillofac Radiol. 2001;30:35–9. doi: 10.1038/sj/dmfr/4600574. [DOI] [PubMed] [Google Scholar]
- 9.Correll RW, Jensen JL, Taylor JB, Rhyne RR. Mineralization of the stylohyoid-stylomandibular ligament complex. A radiographic incidence study. Oral Surg Oral Med Oral Pathol. 1979;48:286–91. doi: 10.1016/0030-4220(79)90025-2. [DOI] [PubMed] [Google Scholar]
- 10.Pravina P, Sayaji D, Avinash M. Calcium and its role in human body. Int J Res Pharm Biomed Sci. 2013;4:659–68. [Google Scholar]