

Abstract
Intraoral epidermoid cyst of buccal mucosa is generally an uncommon entity. Epidermal inclusion cyst refers sequestration of epidermal elements into the dermal and deeper tissue during the fetal period in line of fusion of embryonic process or acquired due to implantation of the epithelium due to trauma or surgery. It usually presents as slow growing asymptomatic cysts but may be symptomatic due to large size, interfering with mastication and speech or secondary infection. Surgical excision is done for removal of these cysts. We report an interesting case of multiple epidermal cysts in both sides of buccal mucosa in a 35-year-old male patient.
Keywords: Buccal mucosa, epidermoid cyst, oral cavity
INTRODUCTION
Epidermoid cysts are benign sequestration cysts in body that may be either congenital or acquired. The congenital variety is related to aberrant embryogenic ectodermal implantation during at the time of closure of neural groove or when epithelial surfaces fuse. Acquired cysts are due to traumatic iatrogenic implantation of epidermal fragments during trauma or surgery.[1] Epidermoid cysts are seen throughout the body with only 7% cases seen in oro-facial region and 1.6% within oral cavity.[2]
We herewith report a case of exceptional existence of intraoral multiple epidermoid cysts in both sides of the buccal mucosa in a 35-year-old male in the buccal cheek region. To the best of our knowledge, it is the first report in English-indexed literature.
CASE REPORT
A 35-year-old male reported to Surgical Department with the chief complaint of swelling in the both sides of buccal mucosa for 3 months, which was incidentally noticed. He had no difficulty in chewing or swallowing food. There was no history of previous surgery or trauma related to the lesion located. Intraoral examination revealed a bilateral 1.5 cm × 1.5 cm nontender swelling in lateral buccal mucosa with normal covering mucosa. Extraorally, the skin overlying the swelling did not show any indurations. There was no associated regional lymphadenopathy. A detailed case history of the patient provided no association of cheek biting with the lesion. The dental examination also revealed no relevant findings. Excision of the lesion lying immediately underlying the buccal mucosa was done under local anesthesia by giving an elliptical incision in the bilateral buccal mucosa. Both wounds were closed with sutures. The postoperative period was uneventful and healing was good. Specimen on gross examination showed gray-white to gray-brown soft-tissue pieces, altogether measuring 0.5 cm × 0.5 cm in size. Microscopically, swelling from both the sides showed three subepidermal cysts arranged in linear fashion, lined by stratified squamous epithelium and lumen partially filled with keratin [Figure 1a–d]. Surrounding stroma showed fibrocollagenous tissue with mild diffuse chronic inflammatory infiltrate comprising lymphocytes, plasma cells, and macrophages. Overlying unremarkable squamous epithelium was seen. Neither dysplasia nor malignancy was noted. A histopathological diagnosis of bilateral multiple epidermoid cysts was made.
Figure 1.
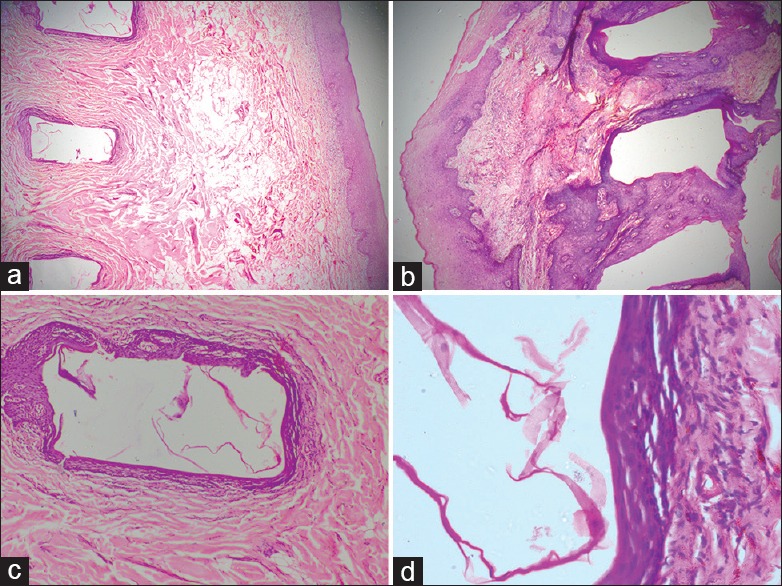
(a and b) Both right and left side linearly arranged multiple linearly arranged epidermoid cysts with overlying stratified squamous epithelial clusters (H and E, ×40); (c) Section shows cyst lined by stratified squamous epithelium with granular cell layer. No appendages are noted within the wall of cyst (H and E, ×100); (d) Cyst wall lined by orthokeratotic stratified squamous epithelium with keratin flakes in the lumen (H and E, ×400)
DISCUSSION
Roser, in 1859, described the term epidermoid cyst. These cysts are dome-shaped and occur just beneath the skin. It is commonly seen in face, neck, chest, or trunk.[3] Most of the cases are reported in between 15 and 35 years of age group.[2]
The incidence of epidermoid cysts in head and neck has been reported from 1.6% to 6.9%. Most of the intraoral cases are reported in the midline and floor of the mouth. Rare cases are reported involving tongue, lips, uvula, temporomandibular joint, intracranial, maxilla and mandible, and buccal mucosa.[4]
Intraoral epidermoid cyst often remains asymptomatic for years until they reach a size that interferes with mastication, speech, and very rarely breathing. However, they can also become acutely symptomatic if they are secondarily infected. Epidermoid cysts may be classified as congenital or acquired even if there is no difference between the two on presentation or histologically.
Many etiopathogenetic theories have been proposed for their development. Congenital cysts are dysembryogenetic lesions that arise from ectodermic elements entrapped during the midline fusion of the first and second branchial arches between the 3rd and 4th weeks of intrauterine life. Alternatively, they may arise from the tuberculum impar of His which, with each mandibular arch, forms the floor of the mouth and the body of the tongue. Acquired cysts derive from traumatic or iatrogenic inclusion of epithelial cells or from the occlusion of a sebaceous gland duct.[5,6,7,8] However, for formation of acquired cysts, a proper combination of events that is a history of trauma along with implanted epithelium that is capable of proliferation and coexistent minimal inflammation are needed to occur simultaneously. These events occurring bilaterally along with the linear arrangement of the cyst probably explain the rarity of this case.
Epidermoid, dermoid, and teratoid cysts are nonodontogenic cystic lesions of the oral cavity. They are rare lesions derived from germinal epithelium. While a dermoid cyst has an epidermal lining with skin adnexa such as hair follicles and sebaceous glands, the epidermoid cyst contains no such adnexa. Teratoid cysts in addition to skin appendages have tissue from other embryonal sources such as respiratory, gastrointestinal, and connective tissues such as bundles of striated muscle and distinct areas of fat.[9,10,11,12]
However, to the best of our knowledge, till now, no case has been reported as multiple epidermoid cysts in bilateral buccal mucosa. However, numerous epidermoid cysts, especially in head and neck, are associated with Gardner's syndrome.[13]
Differential diagnosis should include a variety of conditions which can be developmental, neoplastic, and infectious. Infectious conditions such as odontogenic infections are mostly symptomatic and can be ruled out in the present case as it was not associated with any clinical symptoms. Neoplastic conditions can be excluded due to benign clinical presentation and no associated lymphadenopathy. Swelling due to lipid, salivary, and vascular benign tumors should be considered. Among developmental category, an oral lymphoepithelial cyst which is seen adjacent to Waldeyers's ring should also be kept in mind.[2] The bilaterality of the lesion and confirmation on histopathology help to rule out the above pathologies.
Cases which are symptomatic and others that have undergone malignant transformation have been reported in the literature. Cortezzi and De Albuquerque[14] in 1994 reported an epidermoid cyst of the floor of the mouth that reached a huge proportion and caused a life threatening situation because of secondary infection. Basal cell carcinoma and squamous cell carcinoma arising in the wall of an otherwise conventional epidermoid cyst has been seen.[15,16,17] However, no carcinomatous transformation was noted in our case.
CONCLUSION
Epidermoid cysts are found to exist in rare site which emphasize the need for further research into the etiopathogenesis of the cysts. The present case shows no variation from the normal histopathology, but they prove to be significant because of its variation in their anatomical presentation that is buccal mucosa, multiplicity, and bilaterality. More importantly, if ever malignancy is confirmed in such cases, appropriate evaluation is need to be carried out followed by definitive management.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Goldsmith LA, Katz SI, Gilchrest BA, Paller AS, Leffell DJ, Wolff . Filzpatrick's Dermatology in General Medicine. 8th ed. New York: McGraw-Hill; 2012. [Google Scholar]
- 2.Kini YK, Kharkar VR, Rudagi BM, Kalburge JV. An unusual occurrence of epidermoid cyst in the buccal mucosa: A case report with review of literature. J Maxillofac Oral Surg. 2013;12:90–3. doi: 10.1007/s12663-011-0188-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Kothandaraman S, Thiagarajan B. A cheesy affair! Report of a case of an epidermoid cyst of parotid. Otolaryngol Online J. 2013;3:1–12. [Google Scholar]
- 4.Ozan F, Polat HB, Ay S, Goze F. Epidermoid cyst of the buccal mucosa: A case report. J Contemp Dent Pract. 2007;8:90–6. [PubMed] [Google Scholar]
- 5.Howell CJ. The sublingual dermoid cyst. Report of five cases and review of the literature. Oral Surg Oral Med Oral Pathol. 1985;59:578–80. doi: 10.1016/0030-4220(85)90184-7. [DOI] [PubMed] [Google Scholar]
- 6.Longo F, Maremonti P, Mangone GM, De Maria G, Califano L. Midline (dermoid) cysts of the floor of the mouth: Report of 16 cases and review of surgical techniques. Plast Reconstr Surg. 2003;112:1560–5. doi: 10.1097/01.PRS.0000086735.56187.22. [DOI] [PubMed] [Google Scholar]
- 7.Walstad WR, Solomon JM, Schow SR, Ochs MW. Midline cystic lesion of the floor of the mouth. J Oral Maxillofac Surg. 1998;56:70–4. doi: 10.1016/s0278-2391(98)90919-3. [DOI] [PubMed] [Google Scholar]
- 8.De Ponte FS, Brunelli A, Marchetti E, Bottini DJ. Sublingual epidermoid cyst. J Craniofac Surg. 2002;13:308–10. doi: 10.1097/00001665-200203000-00024. [DOI] [PubMed] [Google Scholar]
- 9.Rajayogeswaran V, Eveson JW. Epidermoid cyst of the buccal mucosa. Oral Surg Oral Med Oral Pathol. 1989;67:181–4. doi: 10.1016/0030-4220(89)90326-5. [DOI] [PubMed] [Google Scholar]
- 10.Worley CM, Laskin DM. Coincidental sublingual and submental epidermoid cysts. J Oral Maxillofac Surg. 1993;51:787–90. doi: 10.1016/s0278-2391(10)80424-0. [DOI] [PubMed] [Google Scholar]
- 11.Zachariades N, Skoura-Kafoussia C. A life-threatening epidermoid cyst of the floor of the mouth: Report of a case. J Oral Maxillofac Surg. 1990;48:400–3. doi: 10.1016/0278-2391(90)90440-d. [DOI] [PubMed] [Google Scholar]
- 12.Calderon S, Kaplan I. Concomitant sublingual and submental epidermoid cysts: A case report. J Oral Maxillofac Surg. 1993;51:790–2. doi: 10.1016/s0278-2391(10)80425-2. [DOI] [PubMed] [Google Scholar]
- 13.Shafer WG, Hine MK, Levy BM. A Textbook of Oral Pathology. 4th ed. Philadelphia: WB Saunders; 1983. pp. 78–9. [Google Scholar]
- 14.Cortezzi W, De Albuquerque EB. Secondarily infected epidermoid cyst in the floor of the mouth causing a life-threatening situation: Report of a case. J Oral Maxillofac Surg. 1994;52:762–4. doi: 10.1016/0278-2391(94)90496-0. [DOI] [PubMed] [Google Scholar]
- 15.Ikeda I, Ono T. Basal cell carcinoma originating from an epidermoid cyst. J Dermatol. 1990;17:643–6. doi: 10.1111/j.1346-8138.1990.tb01709.x. [DOI] [PubMed] [Google Scholar]
- 16.López-Ríos F, Rodríguez-Peralto JL, Castaño E, Benito A. Squamous cell carcinoma arising in a cutaneous epidermal cyst: Case report and literature review. Am J Dermatopathol. 1999;21:174–7. doi: 10.1097/00000372-199904000-00012. [DOI] [PubMed] [Google Scholar]
- 17.Devine JC, Jones DC. Carcinomatous transformation of a sublingual dermoid cyst. A case report. Int J Oral Maxillofac Surg. 2000;29:126–7. [PubMed] [Google Scholar]