

Abstract
Introduction:
Radiation exposure poses hazards for health-care providers as well as patients in health-care facilities (HCFs). Radiographic imaging is extremely valuable as a diagnostic tool in medicine, but ionizing radiation and computed tomography (CT) scan carry well-known potential risks. Personnel and radiation safety monitoring is an important safety precaution in the practice of radiography.
Aim:
The study aimed to assess the occupational radiation exposure and safety protection among medical staff in HCFs in the Eastern Province, Kingdom of Saudi Arabia (KSA).
Materials and Methods:
Total of 4 HCFs with radiological services were randomly selected for the study in the period from January to April 2013. The radiation survey has been carried out by the measurement of radiation in the x-ray and CT-scan room at different points of the diagnostic, imaging, and waiting rooms of different hospitals. The radiation safety was assessed by using a questionnaire
Results:
The results of our study are surprising and alarming. Data revealed that there are a significant association between the levels of radiation exposure in all selected hospitals concerning imaging and waiting X-ray and CT-scan operating room (P < 0.01). For radiation safety, most hospitals have lead aprons and thyroid shields in place, but only about 50% have lead glasses and lead shields, showing that many hospitals still lack essential equipment. Moreover, actual utilization rate of radiation dosimeters are 57.7% and 68.9%, respectively.
Conclusion:
All medical staff as well as patients are at risk of exposure to x-ray and CT-scan radiation exposure, and the levels are exceeding the standard guidelines. Many hospitals still lack safety protection tools and there is a complete absence of radiation protection equipment. Further studies should be conducted to highlight different aspects of radiation exposure dose and safety protection tools.
Keywords: Dose, medical imaging, occupational, radiation, radiographers, safety
INTRODUCTION
The characterization of medical applications, in terms of occupational exposures, is sometimes done by reporting an average annual individual dose for all exposed and/or measurably exposed workers. In practical radiation protection, this approach is, however, meaningless, as individual doses in the medical field differ substantially. During the evaluation of dosimetric data one needs information about the distribution of the yearly doses. It is important to know how many people receive doses lower than X and higher than Y? When individual monitoring is used as a tool in practical radiation protection, it is important to know if the order of magnitude of the individual dose is defined by the nature of the procedure, the individual workload, the level of radiation protection measures, or the methodology of the assessment.[1]
Occupational exposure is the result of radiation exposure at work, and personal dosimetry is an important tool to ensure compliance with regulatory or generally accepted dose limits. Radiation safety is the main health issue of concern to health-care facilities (HCFs). Ionizing radiation is a known carcinogen at high doses, and clinical symptoms are known to be associated with the chronic low-dose exposure. The use of ionizing radiations in medicine is expanding rapidly due to the introduction of new ionizing radiation oriented diagnostic and therapeutic practices. Radiographic imaging is extremely valuable as a diagnostic tool in medicine, but ionizing radiation also carries well-known potential risks.[1,2]
Within a hospital, radiologists, radiology and nuclear medicine technicians, and others involved in the performance of x-ray and computed tomography (CT)-scan examinations, have an increased risk for radiation exposure than the general hospital population.[3]
Radiation exposure poses hazards for health-care providers as well as patients, and it may have somatic and genetic effects. Monitoring of radiation doses received by staff in radiodiagnostic centers is of great importance to the radiographers in their effort to protect themselves, patients, and the general public from the untoward effect of excessive radiation.[3]
The as low as reasonably achievable (ALARA) principle, which emphasizes utilizing techniques and procedures to keep exposure to a level as low as reasonably achievable, should be followed to minimize the risk of radiation exposure to medical professionals. Personnel shielding options (e.g., two-piece wraparound aprons, thyroid shields, and eye protection) should be used to effectively attenuate scattered x-ray levels.[4]
The present study aimed to assess the occupational radiation exposure and radiation safety among medical staff in HCFs in the Eastern Province, Kingdom of Saudi Arabia (KSA).
MATERIALS AND METHODS
This cross-sectional study was carried out in selected HCFs in the Eastern Province, KSA in the period from February to June 2013. Preliminary information regarding the type, level, and location of HCFs were obtained from the website of the Ministry of Health and Population, the Government of Saudi Arabia.
The radiation survey has been carried out by the measurement of radiation at different points of the diagnostic, imaging, and waiting rooms of different hospitals. Radiation was measured in x-ray and CT-scan rooms of four different hospitals in the Eastern Province, KSA using a portable radiation measuring instrument MicroRem (Thermo Scientific™). The measurement was performed during daytime between 8 AM and 5 PM.
The background radiation was measured before the machines were switched on in respective rooms. Subsequently, after the exposure to the radiation, the fall out radiation was measured in four different corners of the radiation facility room of different hospitals. The unit of measurement was in count MicroRem per hour and converted in millisievert per year (mSv/year).
Information of radiation safety was assessed by using questionnaire regarding information about basic principles of radiation safety, radiation exposure in different X-ray and CT-scan, ways to minimize radiation, formal training regarding radiation safety, and utilization of personal protective equipment.
Statistical analysis
The data were entered and analyzed by using Statistical Package for the Social Sciences (SPSS) software, version 16 (SPSS-Inc., Chicago, IL).
RESULT AND DISCUSSION
The primary source of radiation for an x-ray and CT scan is scatter radiation from the patient during imaging. Modern imaging operations produce effective doses of 4-21 mSv and 9-29 mSv, respectively, and are therefore, relatively high risk in terms of radiation exposure. However, radiation safety remains an occupational concern. The ongoing trend toward more complicated interventional procedures results in greater exposure to patients and laboratory staff.[5,6]
The results of our study are surprising and alarming. Though all of the medical staff were aware of the importance of radiation safety, yet significant lapses were found in practice and knowledge in this regard. A grave concern was inadequate availability of standard radiation safety equipment imaging department in HCFs.
Personnel radiation monitoring is an important safety precaution in the practice of radiography. It does not in itself provide protection against ionizing radiations. Its main purpose is to measure radiation dose received by the radiology personnel, is to measure permitted radiation dose received, adequacy of radiation protection facilities and acceptable radiation protection techniques.[7]
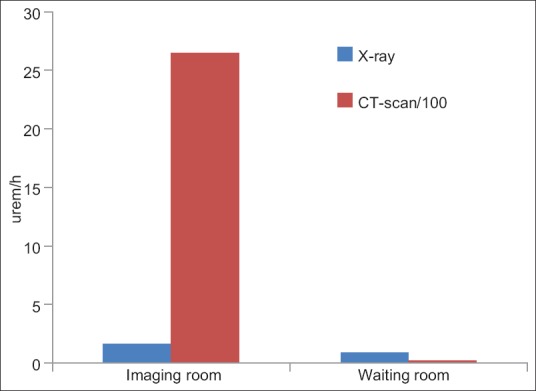
In Table 1 and Figure 1, there are a significant association in the levels of radiation exposure levels in all selected hospitals concerning imaging and waiting room operating X-ray image. Moreover, the high level of radiation exposure might occur due to the leakage of radiation through imaging room and the lack of radiation safety procedures during and after imaging.
Table 1.
Comparison between mean levels of radiation exposure in x-ray in imaging and waiting room
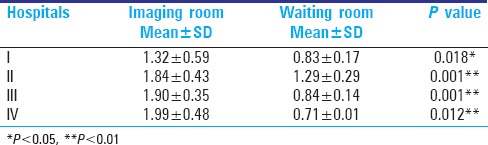
Figure 1.
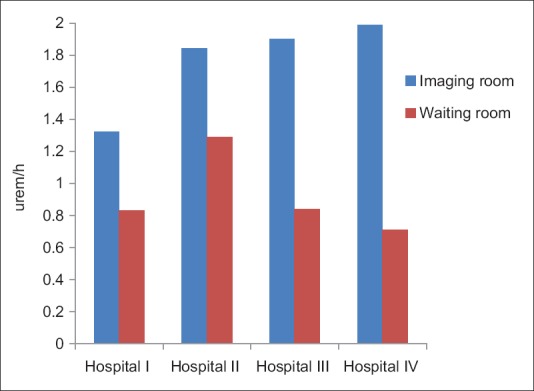
Mean levels of radiation exposure in x-ray in imaging and waiting room
In Table 2 and Figure 2, there are a significant association in the levels of radiation exposure levels in all selected hospitals concerning imaging and waiting room operating CT scan. Moreover, the high level of radiation exposure might occur due to the leakage of radiation through imaging room and the lack of radiation safety procedures during and after imaging.
Table 2.
Comparison between mean levels of radiation exposure in x-ray and CT scan in imaging and waiting room
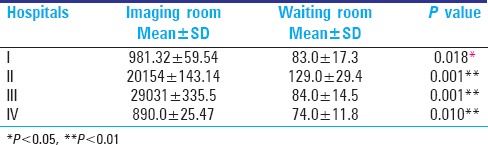
Figure 2.
Mean levels of radiation exposure in CT-scan in imaging and waiting room
The radiations measured at x-ray departments were beyond the prescribed level of 1 mSv/year. (for public exposure) in all the hospitals; the median values also surpassed the prescribed dose limit. The level noted among the hospitals ranged between 1.9 mSv/year and 1.3 mSv/year. Mean amounts of radiation found in different hospitals were greater than 1 mSv/yr. (for public exposure). The mean observed radiation compared with reference limit for public exposure was higher and the difference between the mean observed and recommended values was statistically significant (P < 0.01).
Health workers in some diagnostic and therapeutic procedures are exposed to low doses of ionizing radiation. Chronic exposure to low doses of radiation can have many negative consequences on the human health, such as cataracts and, among the most serious consequences, the increased risk of morbidity for certain types of cancer.[7,8,9]
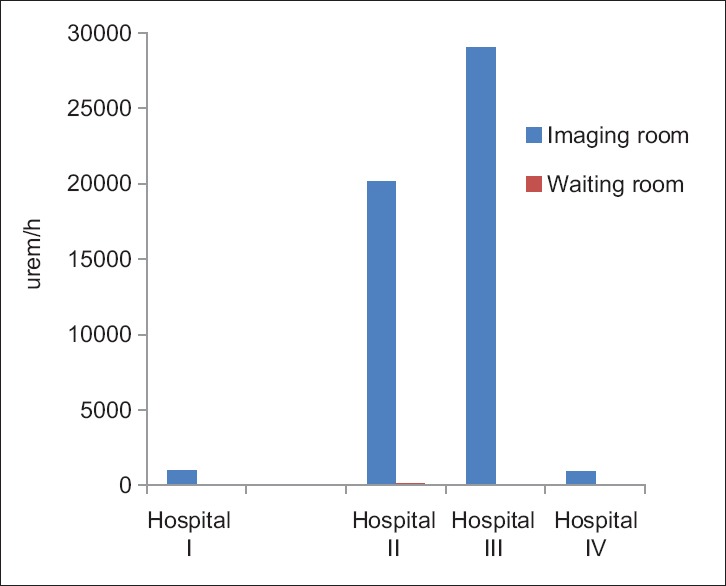
In Table 3 and Figure 3, for all hospitals, the levels of radiation exposure are significantly higher that exceed the international guidelines. Similar study found that the radiation extent of scatter CT-scan facility suggests very high exceedance compared to prescribed limit of exposure. It was about 2649.34 times beyond the limit of 1 mSv/year.
Table 3.
Comparison between mean levels of radiation exposure in x-ray and CT-scan in imaging and waiting room among all selected health-care providers
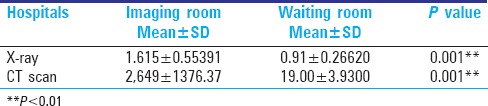
Figure 3.
Mean levels of radiation exposure in X-ray and CT-scan in imaging and waiting room among all selected health-care providers
A comparison made to the occupational exposure limit with the observed doses, it can be stated that the observed levels were much beyond the occupational exposure limit. This suggests the high risk associated to employees and maintenance staff involved in these facilities. Therefore, immediate radiation protection measures to be started to the employees (technicians, attendants, and maintenance staff) at CT-scan.
There is an obvious health risk of radiation exposure for all the exposed population visiting X-radiography department of the hospitals measured. There is however an impending risks of chronic occupational exposure to the employees, technicians, and maintenance personnel of these x-ray machines at the respective hospitals. In this scenario, there is a necessity of adequate and appropriate radiation protection at all the hospitals surveyed.
Ionizing radiation is extensively used in medical practices. Most medical radiation procedures use well-established technologies. However, there is always an intension to apply new technologies, in which both patient and occupational exposures need to be reconsidered. Routine monitoring of occupational exposures is carried out for several reasons. The most obvious reason is to verify and demonstrate compliance with the regulatory dose limits. It can help to identify new exposure pathways or risks and in the framework of the ALARA principle, and routine personal dosimetry is also one of the most important tools to achieve or demonstrate an appropriate level of radiation protection.[1,10]
All were of opinion that radiation safety is extremely important. Majority (99%) of medical staff always used lead aprons, 60% used lead shield, 37% used lead glasses, and 42% used thyroid shield. The percentage of using radiation dosimeter for monitoring radiation exposure represents 80% [Figure 4].[11]
Figure 4.
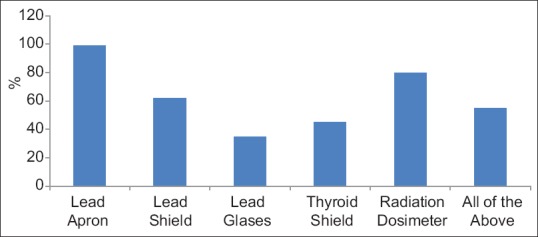
The actual utilization rate of protective equipment
Protective equipment is essential to reduce radiation exposure. During an imaging procedure, a lead apron, a thyroid shield, and lead glasses must be worn, whereas portable lead shields, lead gloves, and lead caps may be optional.
Our survey found that most hospitals have lead aprons and thyroid shields in place, but only about 50% have lead glasses and lead shields, showing that many hospitals still lack essential equipment. Regarding each form of protective equipment, first, a lead apron is the most essential piece of equipment to reduce radiation exposure. Our survey showed that most health-care providers wear lead aprons (99%).Concerning facility management, leaded wall represent a total of (70%) and fire safety adequacy measures (75%).
However, the electrical safety constitutes 82%, whereas maintenance represents 70%. The percentage of using periodic monitoring for radiation exposure represents 20% and training medical staff constitute about 40% [Figure 5]. Second, a thyroid shield is also considered an important protective equipment that reduces wholebody exposure as well as thyroid exposure. A study reported that wearing thyroid shields can reduce the annual effective dose of radiation exposure by 46%. Our survey showed that most hospitals have thyroid shields available. Although thyroid shields are not considered as important as lead aprons, most health-care providers still do not wear thyroid shields (40%). Third, lead glasses provide protection against cataracts arising from radiation exposure. However, lead glasses are less frequently worn than lead aprons or thyroid shields. Our survey showed that less than half of respondents have lead glasses in place and many respondents do not wear them often in 38.2% of cases. The common reason for not wearing protective equipment is that it is bothersome.[11,12,13,14]
Figure 5.
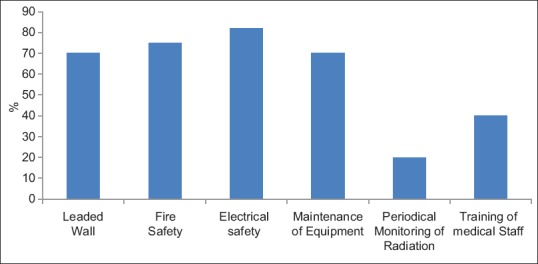
Hospitals radiation safety protection measures
More attention needs to be paid to lead shields as well as lead glasses. Finally, radiation dosimeters do not provide protection against radiation, but tend to reduce radiation exposure because they are a crucial tool in drawing attention to radiation hazards. Survey found that the preparation and actual utilization rate of radiation dosimeters are 57.7% and 68.9%, respectively, indicating low interest in radiation exposure monitoring.
CONCLUSION
All medical staff as well as patients are at risk of exposure to x-ray and CT-scan radiation exposure, and the levels are exceeding the standard guidelines. Therefore, immediate radiation protection measures needs to be initiated to the employees (technicians, attendants, and maintenance staff) at x-ray and CT-scan department.
Many hospitals still lack lead shields and lead glasses, and the actual utilization rate of lead glasses, especially, is low. Future efforts should include minimizing radiation exposure during imaging procedures, and more interest in wearing and preparing protective equipment is needed. Also, hospitals should provide continuous education and supervision for the radiation protection.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Covens P, Berus D, Buls N, Clerinx P, Vanhavere F. Personal dose monitoring in hospitals: Global assessment, critical applications and future needs. Radiat Prot Dosimetry. 2007;124:250–9. doi: 10.1093/rpd/ncm418. [DOI] [PubMed] [Google Scholar]
- 2.Mettler FA, Jr, Kelsey CA, Ricks RC. Medical Management of Radiation Accidents. Boca Raton, FL: CRC Press; 1990. pp. 1–16. [Google Scholar]
- 3.No. RS-G-1.5 Safety Guide: Radiological protection for Medical Exposure to Ionizing Radiation. Vienna: IAEA; 2002. p. 76. [Google Scholar]
- 4.Greenlee C, Burmeister LA, Butler RS, Edinboro CH, Morrison SM, Milas M. Current safety practices relating to I- 131 administered for diseases of the thyroid: A survey of physicians and allied practioners. Thyroid. 2011;21:51–160. doi: 10.1089/thy.2010.0090. [DOI] [PubMed] [Google Scholar]
- 5.Kronenberg A. Radiation-induced genomic instability. Int J Radiat Biol. 1994;66:603–9. doi: 10.1080/09553009414551691. [DOI] [PubMed] [Google Scholar]
- 6.Charles M. Source and effects of ionizing radiation. J Radiol Prot. 2001;21:83–6. doi: 10.1088/0952-4746/21/1/609. [DOI] [PubMed] [Google Scholar]
- 7.Goske MJ, Applegate KE, Boylan J, Butler PF, Callahan MJ, Coley BD, et al. The ‘Image Gently’ campaign: Increasing CT radiation dose awareness through a national education and awareness program. Pediatr Radiol. 2008;38:265–9. doi: 10.1007/s00247-007-0743-3. [DOI] [PubMed] [Google Scholar]
- 8.Donnelly LF. Lessons from history. Pediatr Radiol. 2002;32:287–92. doi: 10.1007/s00247-002-0683-x. [DOI] [PubMed] [Google Scholar]
- 9.Goans RE, Waselenko JK. Medical management of radiological casualties. Health Phys. 2005;89:505–12. doi: 10.1097/01.hp.0000172144.94491.84. [DOI] [PubMed] [Google Scholar]
- 10.McCusker MW, de Blacam C, Keogan M, McDermott R, Beddy P. Survey of medical students and junior house doctors on the effects of medical radiation: Is medical education deficient? Ir J Med Sci. 2009;178:479–83. doi: 10.1007/s11845-009-0341-5. [DOI] [PubMed] [Google Scholar]
- 11.Son BK, Lee KT, Kim JS, Lee SO. Lack of radiation protection for endoscopists performing endoscopic retrograde cholangiopancreatography. Korean J Gastroenterol. 2011;58:93–9. doi: 10.4166/kjg.2011.58.2.93. [DOI] [PubMed] [Google Scholar]
- 12.Piwowarska-Bilska H, Birkenfeld B, Listewnik M, Zorga P. Long-term monitoring of radiation exposure of employees in the Department of Nuclear Medicine (Szczecin, Poland) in the years 1991-2007. Radiat Prot Dosimetry. 2010;140:304–7. doi: 10.1093/rpd/ncq117. [DOI] [PubMed] [Google Scholar]
- 13.Valuckas KP, Atkocius V, Samerdokiene V. Occupational exposure of medical radiation workers in Lithuania, 1991-2003. Acta Med Lituanica. 2007;14:155–9. [Google Scholar]
- 14.Jabeen A, Munir M, Khalil A, Masood M, Akhter P. Occupational exposure from external radiation used in medical practices in Pakistan by film badge dosimetry. Radiat Prot Dosimetry. 2010;140:396–401. doi: 10.1093/rpd/ncq134. [DOI] [PubMed] [Google Scholar]