

Abstract
Background:
Prone, supine, and side position exercises are employed to enhance core stability.
Hypothesis:
Overall core muscle activity would be greater in prone position exercises compared with supine and side position exercises.
Study Design:
Controlled laboratory study.
Methods:
Eighteen men and women between 23 and 45 years of age served as subjects. Surface electrodes were positioned over the upper and lower rectus abdominis, external and internal obliques, rectus femoris, latissimus dorsi, and lumbar paraspinals. Electromyography data were collected during 5 repetitions of 10 exercises, then normalized by maximum voluntary isometric contractions (MVIC). Differences in muscle activity were assessed using 1-way repeated-measures analysis of variance, while t tests with a Bonferroni correction were employed to assess pairwise comparisons.
Results:
Upper and lower rectus abdominis activity was generally significantly greater in the crunch, bent-knee sit-up, and prone position exercises compared with side position exercises. External oblique activity was significantly greater in the prone on ball with right hip extension, side crunch on ball, and side bridge (plank) on toes compared with the prone and side bridge (plank) on knees, the crunch, or the bent-knee sit-up positions. Internal oblique activity was significantly greater in the prone bridge (plank) on ball and prone on ball with left and right hip extension compared with the side crunch on ball and prone and side bridge (plank) on knees positions. Lumbar paraspinal activity was significantly greater in the 3 side position exercises compared with all remaining exercises. Latissimus dorsi activity was significantly greater in the prone on ball with left and right hip extension and prone bridge (plank) on ball and on toes compared with the crunch, bent-knee sit-up, and prone and side bridge (plank) on knees positions. Rectus femoris activity was significantly greater in the prone on ball with left hip extension, bent-knee sit-up, or prone bridge (plank) on toes compared with the remaining exercises.
Conclusion:
Prone position exercises are good alternatives to supine position exercises for recruiting core musculature. Side position exercises are better for oblique and lumbar paraspinal recruitment.
Clinical Relevance:
Because high core muscle activity is associated with high spinal compressive loading, muscle activation patterns should be considered when prescribing trunk exercises to those in which high spinal compressive loading may be deleterious.
Keywords: EMG, low back pain, lumbar spine, sit-up, rectus abdominis
The core musculature includes both deep and superficial muscles of the lumbopelvic-hip complex: internal oblique, transversus abdominis, transversospinalis, quadratus lumborum, psoas major and minor, rectus abdominis, external oblique, erector spinae, latissimus dorsi, gluteus maximus and medius, hamstrings, and rectus femoris.2,3,21,23 Although several studies have examined core muscle recruitment during the crunch and bent-knee sit-up exercises,9,11,35,37 it is not completely understood how core muscle recruitment compares between the supine, prone, and side positions with and without a Swiss ball. Core muscle strengthening can decrease lower extremity injury risk and enhance performance.14,28 Moreover, core muscle strengthening may also help decrease the risk of injuries to the lumbar spine by enhancing spinal stability.2
Core exercises performed in prone and side positions, with and without a Swiss ball, are increasingly popular in rehabilitation clinics and fitness facilities. Several studies examined core muscle recruitment while performing prone and side bridge exercises with and without a Swiss ball.1,5-7,12,15,17-20,27,31-34,36,38,39 During the side bridge exercise, greater internal oblique activity occurs using a Swiss ball compared with a stable-surface bench.5 Greater rectus abdominis, external oblique, and internal oblique activity occurs in the side bridge exercise compared with the crunch exercise.17 No significant difference in rectus abdominis activity occurs during prone and side bridge exercises, but significantly greater external oblique and lumbar paraspinal activity is seen in the side bridge exercise compared with the prone bridge exercise.7 The crunch and side bridge exercises are effective in activating the internal oblique and transversus abdominis,36 while the side bridge is effective in recruiting the quadratus lumborum.22 To date, prone and side bridge exercises have only been performed with body weight supported on the arms and feet, which are the most difficult positions, but not with weight supported on the knees, which is an easier position.5,7,12,17,20,27,36 While select core and lower extremity muscle activity during prone and side position exercises8 is known, studies have not examined their effects on recruiting latissimus dorsi muscle activity. The latissimus dorsi is an upper extremity muscle, but its origin into the thoracolumbar fascia helps provide core stability.
The purpose of this study was to compare core muscle activity among supine, prone, and side position exercises with and without a Swiss ball. Our hypotheses are: (1) overall core muscle activity will be greater in the prone compared with supine position, (2) rectus femoris activity will be similar between the supine bent-knee sit-up and prone exercises on ball or toes, and (3) side position exercises will produce greater internal and external oblique and lumbar paraspinal activity and less rectus abdominis activity compared with prone and supine position exercises.
Methods
Subjects
Written informed consent was in accordance with and approved by the Institutional Review Board at California State University, Sacramento. Nine men and 9 women served as subjects. Mean (SD) age, mass, and height were: 27.7 (7.7) years, 61.1 (7.8) kg, and 165.0 (7.0) cm, respectively, for women and 29.9 (6.6) years, 73.3 (7.2) kg, and 178.1 (4.3) cm, respectively, for men.
Pretest
All subjects became familiar with all exercises during a pretest session that took place approximately 1 week prior to the testing session. All exercises were performed with a 3-second cadence: 1 second from starting position to the ending position, 1 second isometric hold at the ending position, and 1 second return back to starting position. A 1-second rest was given between repetitions. A metronome (set at 1 beat/s) was used to help ensure proper cadence. A subject was tested once they could correctly perform each exercise.
Exercise Descriptions
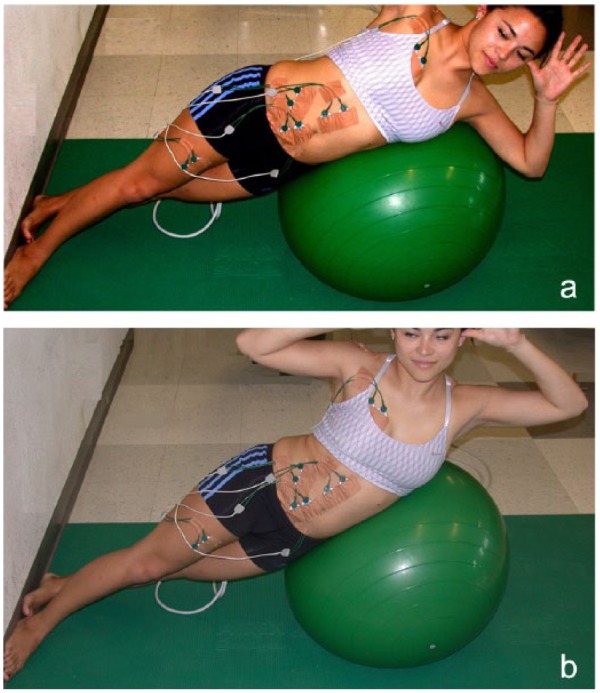
The exercises included in this test are illustrated in Figures 1 to 9: prone on ball with right hip extension (Figure 1a and 1b), prone on ball with left hip extension (Figure 1a and 1c), prone bridge (plank) on ball (Figure 2), prone bridge (plank) on toes (Figure 3), prone bridge (plank) on knees (Figure 4), side crunch on ball (Figure 5), side bridge (plank) on feet (Figure 6), side bridge (plank) on knees (Figure 7), crunch (Figure 8), and bent-knee sit-up (Figure 9).
Figure 1.
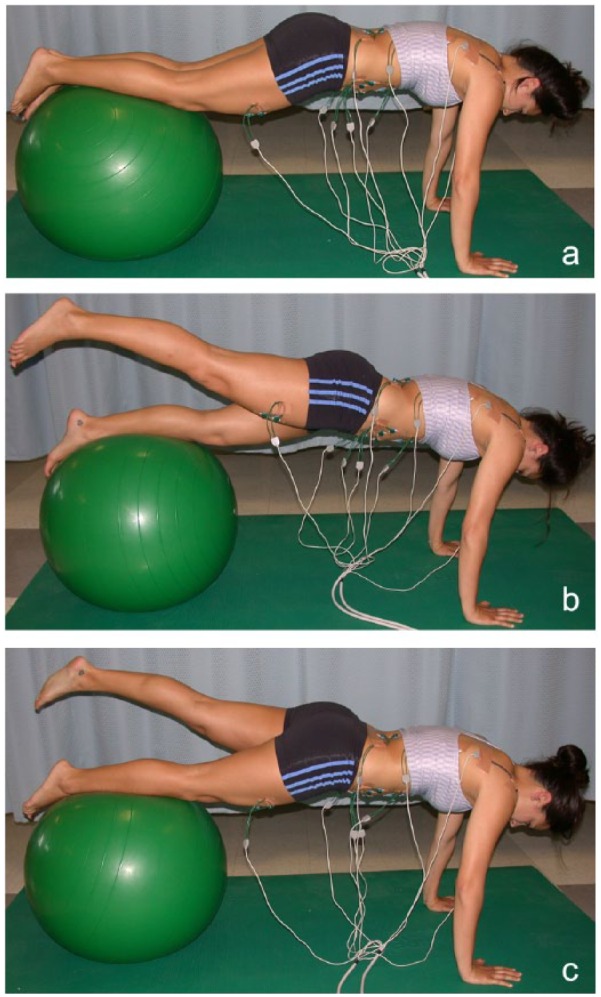
(a) Starting position for the prone on ball with right hip extension and prone on ball with left hip extension. (b) Ending position for the prone on ball with right hip extension. (c) Ending position for the prone on ball with left hip extension.
Figure 9.

Ending position for the bent-knee sit-up.
Figure 2.
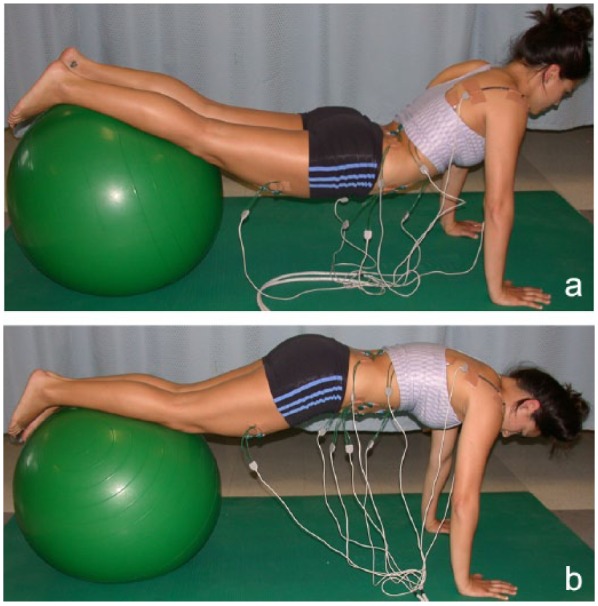
(a) Starting position for the prone bridge (plank) on ball. (b) Ending position for the prone bridge (plank) on ball.
Figure 3.
(a) Starting position for prone bridge (plank) on toes. (b) Ending position for prone bridge (plank) on toes.
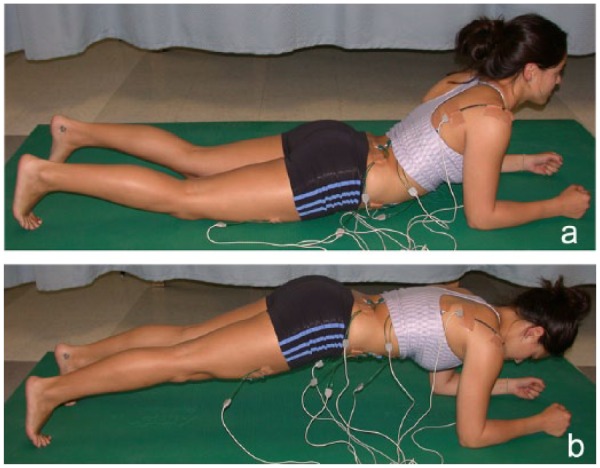
Figure 4.
(a) Starting position for prone bridge (plank) on knees. (b) Ending position for prone bridge (plank) on knees.
Figure 5.
(a) Starting position for side crunch on ball. (b) Ending position for side crunch on ball.
Figure 6.
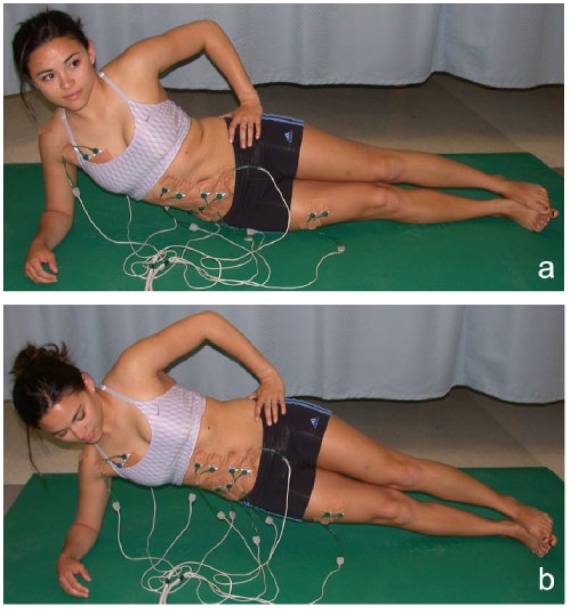
(a) Starting position for side bridge (plank) on toes. (b) Ending position for side bridge (plank) on toes.
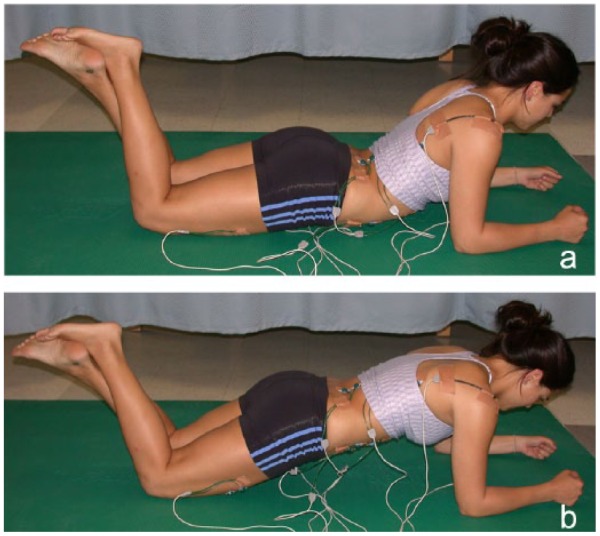
Figure 7.
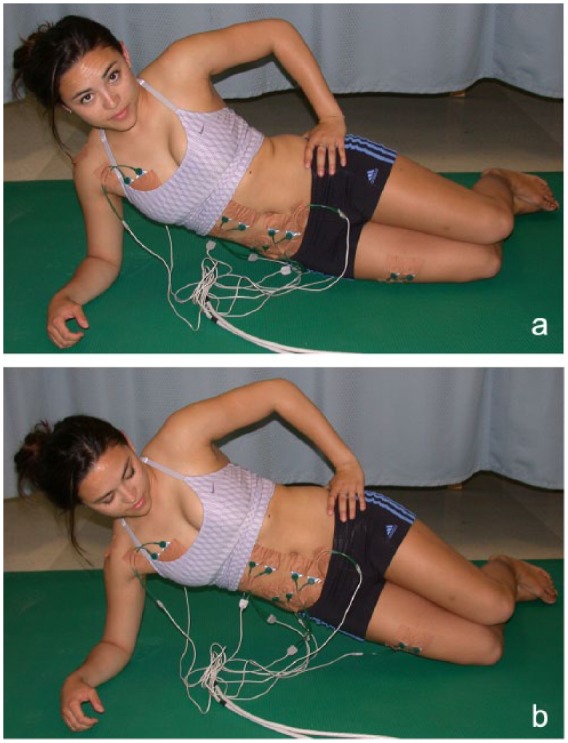
(a) Starting position for side bridge (plank) on knees. (b) Ending position for side bridge (plank) on knees.
Figure 8.

Ending position for the crunch.
Electromyographic Measurements
Eletromyographic (EMG) marker placement procedures have been previously described and were as follows4,9,11,21,30: upper rectus abdominis, lower rectus abdominis, external oblique, internal oblique,2,9-11,21,23,30 latissimus dorsi, rectus femoris, and lumbar paraspinals. A reference electrode was positioned over the skin of the right acromion process.
Data Collection
EMG data were sampled at 1000 Hz using a Noraxon Myosystem unit (Noraxon USA, Inc). The Noraxon amplifier bandwidth filtered the EMG signal from 10 to 500 Hz and is reported to have an input impedance of 20 Mohm and a common-mode rejection ratio of 130 dB.
Prior to performing the exercises, EMG data from each muscle tested were collected during two 5-second maximum voluntary isometric contractions (MVIC) to normalize the exercise EMG data, and these MVIC tests have been previously described.9,11 To classify low to high muscle activities, 0% to 20% MVIC was classified as low muscle activity, 21% to 40% MVIC moderate muscle activity, 41% to 60% MVIC high muscle activity, and greater than 60% MVIC very high muscle activity.10,39
EMG data were collected during 5 repetitions for each exercise and in a randomized order using the 3-second cadence described previously. Approximately 2 minutes of rest was given between each exercise trial.
Each subject rated each exercise using a 15-point perceived exertion rating scale where 6 was no perceived exertion; 7 was very, very light; 9 was very light; 11 was fairly light; 13 was somewhat hard; 15 was hard; 17 was very hard; 19 was very, very hard; and 20 was maximum perceived exertion.2
Data Processing
Raw EMG signals were full-wave rectified and smoothened with a 10-ms moving average window (linear envelope) for all exercise and MVIC trials. EMG signals were then averaged over the entire 3-second exercise duration of each repetition, and EMG data were normalized for each muscle and expressed as a percentage of a subject’s highest corresponding MVIC trial.9,11 Normalized EMG data were averaged over the 5 repetition trials performed for each exercise9-11 and then used in statistical analyses.
Data Analysis
One-factor repeated-measures analysis of variance (ANOVA) was employed to assess differences in normalized EMG muscle activity among exercises, while t tests with a Bonferroni correction were employed to assess pairwise comparisons. To minimize the probability of type I errors, a Bonferroni adjustment was performed (0.05/9). The adjusted level of significance employed was P = 0.006.
Results
Significant differences (P < 0.001) in muscle activity were seen between exercises in supine, prone, and side positions with and without a Swiss ball (Table 1). Compared with supine position exercises (crunch and bent-knee sit-up), prone position exercises (with hip extension, prone bridge on ball, prone bridge on toes) demonstrated similar upper and lower rectus abdominis, internal oblique, and lumbar paraspinal activity; approximately 10% to 100% more external oblique activity; approximately 110% to 160% more latissimus dorsi activity; and several times more rectus femoris activity compared with the crunch. The prone on ball with left hip extension exercise generated approximately 50% more rectus femoris activity compared with the bent-knee sit-up, while the bent-knee sit-up generated over twice as much rectus femoris activity compared with the prone bridge (plank) on ball exercise.
Table 1.
Mean (SD) muscle activity (electromyography) for each muscle and exercise expressed as a percentage of each muscle’s maximum isometric voluntary contraction
| Exercise | Upper Rectus Abdominis* | Lower Rectus Abdominis* | External Oblique* | Internal Oblique* | Lumbar Paraspinal* | Latissimus Dorsi* | Rectus Femoris* |
|---|---|---|---|---|---|---|---|
| Prone on ball with right hip extension | 43 (21) | 44 (11) | 56 (32) | 40 (26) | 7 (3) h , i , j | 17 (13) | 9 (5) b , d , f |
| Prone on ball with left hip extension | 41 (24) | 39 (19) | 39 (19) | 45 (25) | 6 (3) h , i , j | 21 (14) | 35 (18) |
| Prone bridge (plank) on ball | 49 (26) | 48 (9) | 42 (23) | 39 (19) | 6 (2) h , i , j | 17 (10) | 10 (7) b , d , f |
| Prone bridge (plank) on toes | 34 (15) | 40 (10) | 40 (21) | 29 (12) | 5 (2) h , i , j | 18 (12) | 20 (7) d |
| Prone bridge (plank) on knees | 27 (9) a , e | 26 (9) a , c , d , e , f | 22 (14) c , h , i | 20 (8) c , d , e | 5 (2) h , i , j | 10 (6) c , d , e , f | 7 (5) b , d , f |
| Side crunch on ball | 21 (11) a , b , c , d , e | 16 (7) a , b , c , d , e , f , g | 50 (26) | 20 (1) c , d , e | 22 (7) i | 12 (5)d | 8 (4) b , d , f |
| Side bridge (plank) on toes | 26 (15) a , e | 21 (9) a , b , c , d , e , f | 62 (37) | 28 (12) d | 29 (16) | 12 (10) d | 14 (4) b , d |
| Side bridge (plank) on knees | 17 (10) a , b , c , d , e , f | 14 (8) a , b , c , d , e , f , g | 37 (27) i | 17 (7) a , c , d , e | 18 (6) i | 10 (5) d , e , f | 10 (4) b , d , f |
| Crunch | 53 (19) | 39 (16) | 28 (17) c . i | 33 (13) | 5 (2) h , i , j | 8 (3) c , d , e , f | 6 (4) b , d , f |
| Bent-knee sit-up | 40 (13) | 35 (14) e | 36 (14) i | 31 (11) | 6 (2) h , i , j | 8 (3) c , d , e , f | 23 (12) d |
Significant difference (P < 0.001) in muscle activity among abdominal exercises based on a 1-way repeated-measures analysis of variance.
Significantly less muscle activity compared with the crunch.
Significantly less muscle activity compared with the bent-knee sit-up.
Significantly less muscle activity compared with the prone on ball with right hip extension.
Significantly less muscle activity compared with the prone on ball with left hip extension.
Significantly less muscle activity compared with the prone bridge (plank) on ball.
Significantly less muscle activity compared with the prone bridge (plank) on toes.
Significantly less muscle activity compared with the prone bridge (plank) on knees.
Significantly less muscle activity compared with the side crunch on ball.
Significantly less muscle activity compared with the side bridge (plank) on toes.
Significantly less muscle activity compared with the side bridge (plank) on knees.
Compared with supine and prone position exercises, side position exercises (side crunch on ball and side bridge on toes and knees) generally demonstrated significantly less upper and lower rectus abdominis, internal oblique, and latissimus dorsi (prone exercises only) activity as well as rectus femoris activity (except crunch and prone bridge [plank] on ball) but significantly greater lumbar paraspinal activity. Performing prone and side position exercises were perceived easiest on the knees and more difficult on the toes or feet (Table 2). The prone on ball with hip extension exercises were rated as the most difficult to perform.
Table 2.
The mean (SD) ratings of perceived exertion among exercises
| Exercise | Ratings of Perceived Exertion a |
|---|---|
| Prone on ball with right hip extension | 13.1 (1.4)—somewhat hard |
| Prone on ball with left hip extension | 13.1 (1.4)—somewhat hard |
| Prone bridge (plank) on ball | 11.8 (1.6)—fairly light |
| Prone bridge (plank) on toes | 11.9 (1.7)—fairly light |
| Prone bridge (plank) on knees | 8.9 (2.1)—very, very light |
| Side crunch on ball | 11.2 (2.2)—fairly light |
| Side bridge (plank) on toes | 11.2 (2.2)—fairly light |
| Side bridge (plank) on knees | 9.9 (2.0)—very light |
| Crunch | 10.2 (2.2)—very light |
| Bent-knee sit-up | 10.4 (2.5)—very light |
Based on the following scale: 6, no perceived exertion; 7, very, very light; 9, very light; 11, fairly light; 13, somewhat hard; 15, hard; 17, very hard; 19, very, very hard; and 20, maximum perceived exertion.
Discussion
Muscle Activity Between Prone and Supine Position Exercises
The hypothesis that overall core muscle activity would be greater in prone than supine position exercises was supported by the results. The greater effectiveness in core muscle recruitment of the prone on ball with hip extension exercises compared with the crunch and bent-knee sit-up implies that these exercises are good alternatives to the crunch and bent-knee sit-up, although they are also more difficult to perform (Table 2). Greater demand exercises, such as the hip extension and prone bridge on toes exercises, may be appropriate for higher level individuals or performed in the latter stages of a progressive abdominal strengthening program.
Strong core muscles help stabilize the core by compressing and stiffening the spine16,25,26 and have been shown to decrease injury risk and enhance performance.2,14,28 The prone bridge (plank) on toes was 2 to 3 times more effective in latissimus dorsi and rectus femoris recruitment compared with the crunch. However, because the rectus femoris attempts to anteriorly tilt the pelvis and accentuate lumbar lordosis, exercises that generate moderate or high rectus femoris activity may not be desirable, especially in individuals with weak abdominal musculature or lumbar pathology. Several studies1,6,7,19,34 reported findings similar to the current study.
During prone on ball with hip extension exercises, the pelvis and spine are stabilized and maintained in a neutral position due to isometric abdominal/oblique muscle actions. In contrast, the bent-knee sit-up and crunch actively flex the trunk by concentric muscle actions during the upward motion. The lumbar spinal flexion may be contraindicated in certain populations with lumbar disc pathologies or osteoporosis or posterolateral disc herniations. Lumbar spinal flexion is only 3° during the crunch but approximately 30° during the bent-knee sit-up.13 In addition, the bent-knee sit-up generates greater intradiscal pressure29 and lumbar compression2 compared with exercises similar to the crunch, largely due to increased lumbar flexion and hip flexor activity. The crunch may be safer than the bent-knee sit-up for individuals who need to minimize lumbar spinal flexion or compressive forces because of lumbar pathology. In contrast, individuals with facet joint pain, spondylolisthesis, and vertebral or intervertebral foramen stenosis may not benefit from prone position exercises, which maintain the spine and pelvis in a more extended position, as it may contribute to nerve root compression or facet joint pain.2,17,23,25 However, trunk flexion exercises like the crunch and bent-knee sit-up may be beneficial for some patients with facet pathology or stenosis, as trunk flexion may help relieve facet joint pain and minimize the risk of nerve root or spinal cord compression due to spinal stenosis.2,17,23,25
Muscle Activity Between Prone and Side Position Exercises
Our hypothesis that rectus abdominus activity would be greater in prone than side position exercises and oblique and lumbar paraspinal activity would be greater in side than prone position exercises was largely supported by the results of the current study as well as other studies.6-8,17,24,36,38,39 However, 1 study17 reported greater upper rectus abdominis (46% vs 26% MVIC) and internal oblique (57% vs 28% MVIC) activity but less external oblique (51% vs 62% MVIC) activity than the current study. EMG magnitudes may vary among EMG studies due to different EMG normalization methods, which is a limitation when comparing EMG studies. Moreover, EMG magnitudes may vary depending on whether the exercises were performed dynamically39 or isometrically.6,8,17 Compared with the prone bridge on toes, the side bridge on toes generates significantly greater external oblique (69% vs 47% MVIC) and lumbar paraspinal (42% vs 5% MVIC) activity, but no significant difference in upper rectus abdominis activity,7 which is similar to the current results.
The low to moderate lumbar paraspinal activity in most exercises is similar to other studies.5,7-9,11,17,20,27 Moderate to high activity from the lumbar paraspinals may be deleterious for those with weak abdominal muscles or lumbar instability because the forces generated from lumbar muscles tend to anteriorly rotate the pelvis and may increase lumbar spine lordosis. The greatest lumbar activity was in the side bridge on toes position, and lumbar and oblique activity are greatest on the side that the side bridge on toes exercise occurs on.8 High spinal L4 to L5 compressive loading (2726 N) has been reported during the side bridge on toes position, thus should be used cautiously with individuals with lumbar pathology.
Muscle Activity Within Prone Position and Within Side Position Exercises
As hypothesized, core muscle activity was different within prone position exercises and within side position exercises, with approximately 25% to 185% greater abdominal, oblique, latissimus dorsi, lumbar paraspinal, and rectus femoris activity when performed on toes compared with when performed on knees. The prone and side bridge on knees exercises were perceived to be the easiest to perform and produced the lowest amount of core muscle recruitment and produced less lumbar spine compressive loading compared with the side bridge on toes.2 Core exercises that produce relatively low core muscle activity are often least effective in core stability but more effective in minimizing spinal compressive loading.17 Therefore, performing prone and side plank exercises on knees may be appropriate to start with in the early stages of an abdominal strengthening program or for those who need to minimize spinal compressive loading due to lumbar pathology, while the more challenging prone or side plank on toes exercise can be employed in the latter stages of rehabilitation.
Conclusion
When Swiss ball and floor exercises were performed with similar movement patterns, muscle activity was similar in all or most of the core muscles examined. Core muscle activity and perceived exertion was less for prone and side position exercises performed on knees compared with on toes/feet; thus, performing prone and side position exercises on knees early in spine rehabilitation or training programs (especially in individuals with poor core strength) may be prudent, while gradually progressing these exercises on to the toes/feet and then on a Swiss ball, such as prone on ball with hip extension, which generated the highest core muscle activity and was the most difficult to perform. The prone on ball hip extension exercises produced the greatest core muscle activity, and prone exercises were as or more effective than supine position exercises (crunch and bent knee sit-up) for core muscle activity.
Acknowledgments
We would like to acknowledge Duncan Bell, MPT, Gwen Bramble, MPT, Jason Daffron, MPT, and Steve Lambert, MPT, for all their assistance in data collection and data analysis for this project. We would also like to acknowledge the graduate students in the Department of Physical Therapy at California State University, Sacramento, for all their assistance in data collection for this project.
Footnotes
The authors report no potential conflicts of interest in the development and publication of this article.
References
- 1. Atkins SJ, Bentley I, Brooks D, Burrows MP, Hurst HT, Sinclair JK. Electromyographic response of global abdominal stabilizers in response to stable- and unstable-base isometric exercise. J Strength Cond Res. 2015;29:1609-1615. [DOI] [PubMed] [Google Scholar]
- 2. Axler CT, McGill SM. Low back loads over a variety of abdominal exercises: searching for the safest abdominal challenge. Med Sci Sports Exerc. 1997;29:804-811. [DOI] [PubMed] [Google Scholar]
- 3. Balady G, Berra K, Golding L, Gordon N, Mahler D, Myers J. Physical fitness testing and interpretation. In: ACSM’s Guidelines for Exercise Testing and Prescription. Baltimore, MD: Lippincott Williams & Wilkins; 2000:59-60. [Google Scholar]
- 4. Basmajian J, Blumenstein R. Electrode Placement in EMG Biofeedback. Baltimore, MD: Williams & Wilkins; 1980. [Google Scholar]
- 5. Behm DG, Leonard AM, Young WB, Bonsey WA, MacKinnon SN. Trunk muscle electromyographic activity with unstable and unilateral exercises. J Strength Cond Res. 2005;19:193-201. [DOI] [PubMed] [Google Scholar]
- 6. Czaprowski D, Afeltowicz A, Gebicka A, et al. Abdominal muscle EMG-activity during bridge exercises on stable and unstable surfaces. Phys Ther Sport. 2014;15:162-168. [DOI] [PubMed] [Google Scholar]
- 7. Ekstrom RA, Donatelli RA, Carp KC. Electromyographic analysis of core trunk, hip, and thigh muscles during 9 rehabilitation exercises. J Orthop Sports Phys Ther. 2007;37:754-762. [DOI] [PubMed] [Google Scholar]
- 8. Ekstrom RA, Osborn RW, Hauer PL. Surface electromyographic analysis of the low back muscles during rehabilitation exercises. J Orthop Sports Phys Ther. 2008;38:736-745. [DOI] [PubMed] [Google Scholar]
- 9. Escamilla RF, Babb E, DeWitt R, et al. Electromyographic analysis of traditional and nontraditional abdominal exercises: implications for rehabilitation and training. Phys Ther. 2006;86:656-671. [PubMed] [Google Scholar]
- 10. Escamilla RF, Lewis C, Bell D, et al. Core muscle activation during Swiss ball and traditional abdominal exercises. J Orthop Sports Phys Ther. 2010;40:265-276. [DOI] [PubMed] [Google Scholar]
- 11. Escamilla RF, McTaggart MS, Fricklas EJ, et al. An electromyographic analysis of commercial and common abdominal exercises: implications for rehabilitation and training. J Orthop Sports Phys Ther. 2006;36:45-57. [DOI] [PubMed] [Google Scholar]
- 12. Freeman S, Karpowicz A, Gray J, McGill S. Quantifying muscle patterns and spine load during various forms of the push-up. Med Sci Sports Exerc. 2006;38:570-577. [DOI] [PubMed] [Google Scholar]
- 13. Halpern AA, Bleck EE. Sit-up exercises: an electromyographic study. Clin Orthop Relat Res. 1979;(145):172-178. [PubMed] [Google Scholar]
- 14. Hewett TE, Lindenfeld TN, Riccobene JV, Noyes FR. The effect of neuromuscular training on the incidence of knee injury in female athletes. A prospective study. Am J Sports Med. 1999;27:699-706. [DOI] [PubMed] [Google Scholar]
- 15. Imai A, Kaneoka K, Okubo Y, et al. Trunk muscle activity during lumbar stabilization exercises on both a stable and unstable surface. J Orthop Sports Phys Ther. 2010;40:369-375. [DOI] [PubMed] [Google Scholar]
- 16. Juker D, McGill S, Kropf P, Steffen T. Quantitative intramuscular myoelectric activity of lumbar portions of psoas and the abdominal wall during a wide variety of tasks. Med Sci Sports Exerc. 1998;30:301-310. [DOI] [PubMed] [Google Scholar]
- 17. Kavcic N, Grenier S, McGill SM. Quantifying tissue loads and spine stability while performing commonly prescribed low back stabilization exercises. Spine (Phila Pa 1976). 2004;29:2319-2329. [DOI] [PubMed] [Google Scholar]
- 18. Lehman GJ, MacMillan B, MacIntyre I, Chivers M, Fluter M. Shoulder muscle EMG activity during push up variations on and off a Swiss ball. Dyn Med. 2006;5:7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Marshall PW, Desai I. Electromyographic analysis of upper body, lower body, and abdominal muscles during advanced Swiss ball exercises. J Strength Cond Res. 2010;24:1537-1545. [DOI] [PubMed] [Google Scholar]
- 20. Marshall PW, Murphy BA. Core stability exercises on and off a Swiss ball. Arch Phys Med Rehabil. 2005;86:242-249. [DOI] [PubMed] [Google Scholar]
- 21. McGill S, Juker D, Kropf P. Appropriately placed surface EMG electrodes reflect deep muscle activity (psoas, quadratus lumborum, abdominal wall) in the lumbar spine. J Biomech. 1996;29:1503-1507. [DOI] [PubMed] [Google Scholar]
- 22. McGill S, Juker D, Kropf P. Quantitative intramuscular myoelectric activity of quadratus lumborum during a wide variety of tasks. Clin Biomech (Bristol, Avon). 1996;11:170-172. [DOI] [PubMed] [Google Scholar]
- 23. McGill SM. Distribution of tissue loads in the low back during a variety of daily and rehabilitation tasks. J Rehabil Res Dev. 1997;34:448-458. [PubMed] [Google Scholar]
- 24. McGill SM. Low back exercises: evidence for improving exercise regimens. Phys Ther. 1998;78:754-765. [DOI] [PubMed] [Google Scholar]
- 25. McGill SM. Low back stability: from formal description to issues for performance and rehabilitation. Exerc Sport Sci Rev. 2001;29:26-31. [DOI] [PubMed] [Google Scholar]
- 26. McGill SM, Grenier S, Kavcic N, Cholewicki J. Coordination of muscle activity to assure stability of the lumbar spine. J Electromyogr Kinesiol. 2003;13:353-359. [DOI] [PubMed] [Google Scholar]
- 27. Mori A. Electromyographic activity of selected trunk muscles during stabilization exercises using a gym ball. Electromyogr Clin Neurophysiol. 2004;44:57-64. [PubMed] [Google Scholar]
- 28. Myer GD, Chu DA, Brent JL, Hewett TE. Trunk and hip control neuromuscular training for the prevention of knee joint injury. Clin Sports Med. 2008;27:425-448. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Nachemson A. The lumbar spine: an orthopaedic challenge. Spine. 1976;1:59-71. [Google Scholar]
- 30. Ng JK, Kippers V, Richardson CA. Muscle fibre orientation of abdominal muscles and suggested surface EMG electrode positions. Electromyogr Clin Neurophysiol. 1998;38:51-58. [PubMed] [Google Scholar]
- 31. Norwood JT, Anderson GS, Gaetz MB, Twist PW. Electromyographic activity of the trunk stabilizers during stable and unstable bench press. J Strength Cond Res. 2007;21:343-347. [DOI] [PubMed] [Google Scholar]
- 32. Oh JS, Cynn HS, Won JH, Kwon OY, Yi CH. Effects of performing an abdominal drawing-in maneuver during prone hip extension exercises on hip and back extensor muscle activity and amount of anterior pelvic tilt. J Orthop Sports Phys Ther. 2007;37:320-324. [DOI] [PubMed] [Google Scholar]
- 33. Schoenfeld BJ, Contreras B, Tiryaki-Sonmez G, Willardson JM, Fontana F. An electromyographic comparison of a modified version of the plank with a long lever and posterior tilt versus the traditional plank exercise. Sports Biomech. 2014;13:296-306. [DOI] [PubMed] [Google Scholar]
- 34. Snarr RL, Esco MR. Electromyographical comparison of plank variations performed with and without instability devices. J Strength Cond Res. 2014;28:3298-305. [DOI] [PubMed] [Google Scholar]
- 35. Sternlicht E, Rugg S, Fujii LL, Tomomitsu KF, Seki MM. Electromyographic comparison of a stability ball crunch with a traditional crunch. J Strength Cond Res. 2007;21:506-509. [DOI] [PubMed] [Google Scholar]
- 36. Teyhen DS, Rieger JL, Westrick RB, Miller AC, Molloy JM, Childs JD. Changes in deep abdominal muscle thickness during common trunk-strengthening exercises using ultrasound imaging. J Orthop Sports Phys Ther. 2008;38:596-605. [DOI] [PubMed] [Google Scholar]
- 37. Vera-Garcia FJ, Grenier SG, McGill SM. Abdominal muscle response during curl-ups on both stable and labile surfaces. Phys Ther. 2000;80:564-569. [PubMed] [Google Scholar]
- 38. Willardson JM, Behm DG, Huang SY, Rehg MD, Kattenbraker MS, Fontana FE. A comparison of trunk muscle activation: Ab Circle vs. traditional modalities. J Strength Cond Res. 2010;24:3415-3421. [DOI] [PubMed] [Google Scholar]
- 39. Youdas JW, Boor MM, Darfler AL, Koenig MK, Mills KM, Hollman JH. Surface electromyographic analysis of core trunk and hip muscles during selected rehabilitation exercises in the side-bridge to neutral spine position. Sports Health. 2014;6:416-421. [DOI] [PMC free article] [PubMed] [Google Scholar]