

Introduction
Faun tail nevus is an abnormal lumbar hypertrichosis represented by tufts of coarse terminal hair, several inches long usually manifesting as a lozenge or triangular patch in the lumbosacral area and may overlie an occult spinal abnormality [1]. Fine soft non-terminal or lanugo hair in a similar distribution represents “Silky down” [2].
The cases describe this rare neurocutaneous marker.
Case 1
A 17 year old girl presented with a large congenital hypertrichotic area in the lumbosacral region, for a ‘cosmetic treatment'. The parents had noticed the ‘hairy’ patch with dark coarse hair at birth over the spine. There was no history of back pains, urinary incontinence, paraesthesias or weakness of the lower limbs. There was no family history of a similar lesion and she was born out of a non consanguineous marriage.
Dermatological examination revealed a 25 × 20 cm circumscribed area of hypertrichosis (Fig. 1), with coarse dark terminal hair overlying the lumbar spine on an apparently normal skin. The neurological examination was essentially normal. The patient exhibited a normal gait, normal deep tendon jerks, and grade V power in all muscle groups in the lower limbs. She could perceive all modalities of sensations. Radiograph of lumbosacral spine revealed failure of fusion of posterior arch of 3rd and 4th lumbar vertebra (Fig. 2).
Fig. 1.

Lozenge shaped hypertrichosis lumbosacral spine of Faun tail nevus
Fig. 2.

Radiograph lumbosacral spine : Failure of fusion of posterior arch 3rd and 4th lumbar vertebra
Case 2
A one and a half year old girl was brought by parents for cosmetic improvement of a large area of coarse dark hair overlying the lumbosacral area. The child was unable to walk.
Dermatological examination revealed a large lozenge shaped hypertrichotic area of coarse terminal hair overlying the lumbar spine (Fig. 3).
Fig. 3.

Faun tail nevus in 2nd case
Magnetic resonance imaging spine showed, a congenital block vertebra of L1-L2 and a long septate dorsolumbar syrinx with duct ectasia (Fig. 4).
Fig. 4.
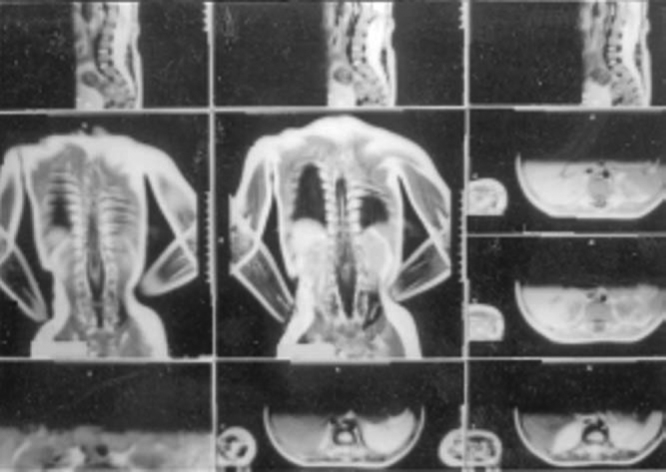
MRI spine shows congenital block vertebra of L1-L2, long septate dorsolumbar syinx with duct ectasia
Discussion
Hypertrichosis in the lumbosacral region may be normal, especially in certain racial groups such as African American, Asian, and Hispanic [3].
Abnormal lumbar hypertrichosis may present as ‘Silky down’ or a ‘Faun tail'. When this occurs away from the spine it is known as simple nevoid hypertrichosis. Silky down presents as soft non- terminal hair, while a faun tail is a wide patch of coarse terminal hair, several inches long. More than half of reported cases of spinal dysraphism have associated dermatologic findings, with one-third of those cases showing hypertrichosis [2].
Patients with well localized paraspinal hypertrichosis must undergo a neurological and radiological assessment to exclude spinal abnormalities [1]. Faun tail nevus is known to be associated with diastematomyelia, meningocele, myelomeningocele, myeloschisis, occult spina bifida, diplomyelia, tethered conus, intraspinal lipoma, lipomyelomeningocele and dermoid cyst.
Our first patient had been to various out patient departments, but no neurological or radiological assessment was done and she was referred for hair removal. The patient was unaware of any underlying spinal abnormality and was asymptomatic with no clinico-neurological markers to suggest so. She was advised an MRI spine, but was lost to follow up.
The second case had been investigated for an underlying spinal abnormality, however the parents brought the patient for a cosmetic treatment and defaulted on followup of definitive neurological treatment. The child was unable to walk with motor involvement of both lower limbs. The two cases reveal a spectrum of neurological involvement which can be associated with an innocuous cutaneous marker.
A literature search revealed only few cases of this disorder [4, 5, 6]. The case is reported to highlight the importance of a thorough clinical and radiological assessment in such apparently normal individuals [7] and those with a definitive neurological abnormality, with a neurocutaneous marker. Such cutaneous markers present the physician with a unique opportunity to detect and initiate appropriate management in these cases to prevent irreversible neurological damage [8].
Conflicts of Interest
None identified
References
- 1.Thursfield WR, Ross AA. Faun tail (sacral hirsuties) and diastematomyelia. Br J Dermatol. 1961;73:328–336. doi: 10.1111/j.1365-2133.1961.tb14457.x. [DOI] [PubMed] [Google Scholar]
- 2.Tavafoghi V, Ghandchi A, Hambrick GW, Udverhelyi GB. Cutaneous signs of spinal dysraphism. Arch Dermatol. 1978;114:573–577. doi: 10.1001/archderm.114.4.573. [DOI] [PubMed] [Google Scholar]
- 3.Drolet BA. Cutaneous signs of neural tube dysraphism. Pediatr Clin North Am. 2000;47:813–823. doi: 10.1016/s0031-3955(05)70241-8. [DOI] [PubMed] [Google Scholar]
- 4.Dhar S. Fauntail Naevus. Indian J Dermatol. 1994;60:47–48. [Google Scholar]
- 5.Birol A, Bademci G. Faun tail: diagnosis of occult spinal dysraphism with a rare cutaneous marker. J Dermatol. 2004;31:251–252. doi: 10.1111/j.1346-8138.2004.tb00667.x. [DOI] [PubMed] [Google Scholar]
- 6.Kaya TI, Kokturk A, Guleryuz A, Bagdatoglu C, Ikizoglu G. Faun tail: a rare cutaneous stigma of spinal dysraphism. Int J Dermatol. 2002;41:119–120. doi: 10.1046/j.1365-4362.2002.01422.x. [DOI] [PubMed] [Google Scholar]
- 7.Basak P, Kanwar AJ, Kaur S, Dhar S. Faun-tail nevus—a case report. Indian J Dermatol. 1989;34:66–68. [PubMed] [Google Scholar]
- 8.Antony FC, Holden CA. Diffuse hypertrichosis and faun-tail naevus as cutaneous markers of spinal dysraphism. Clin Exp Dermatol. 2002;27:645–648. doi: 10.1046/j.1365-2230.2002.01091.x. [DOI] [PubMed] [Google Scholar]