

Abstract
Orthodontic therapies involving no compliance from patients are the mainstay of modern orthodontics. Class II division 1 malocclusions constitute the bulk of cases requiring extractions to facilitate space gain to correct it. The Pendulum Appliance is an effective and reliable method for distalizing maxillary molars. Its major advantages are minimal dependence on patient compliance, ease of fabrication, one-time activation, adjustment of the springs if necessary to correct minor transverse and vertical molar positions and patient-acceptance. Simple laboratory procedure for fabrication and relatively low cost make it an excellent appliance to be incorporated into regular practice.
Key Words: Pendulum appliance, Non-compliance, Orthodontic treatment
Introduction
James J Hilgers of California introduced the Pendulum Appliance in 1992 as a mechanism for Class II non-complaince treatment [1]. The Pendulum Appliance uses a large Nance acrylic button for palatal anchorage and 0.032” TMA springs to deliver a light, continuous force to the upper first molars without affecting the palatal button. The appliance produces a broad pendulum of force from the mid palate to the upper molars.
Fabrication
The right and left Pendulum springs, formed from 0.032” TMA wire, consist of a molar insertion wire, a small horizontal adjustment loop, a closed helix and a loop for retention in the acrylic button (Fig 1).
Fig. 1.
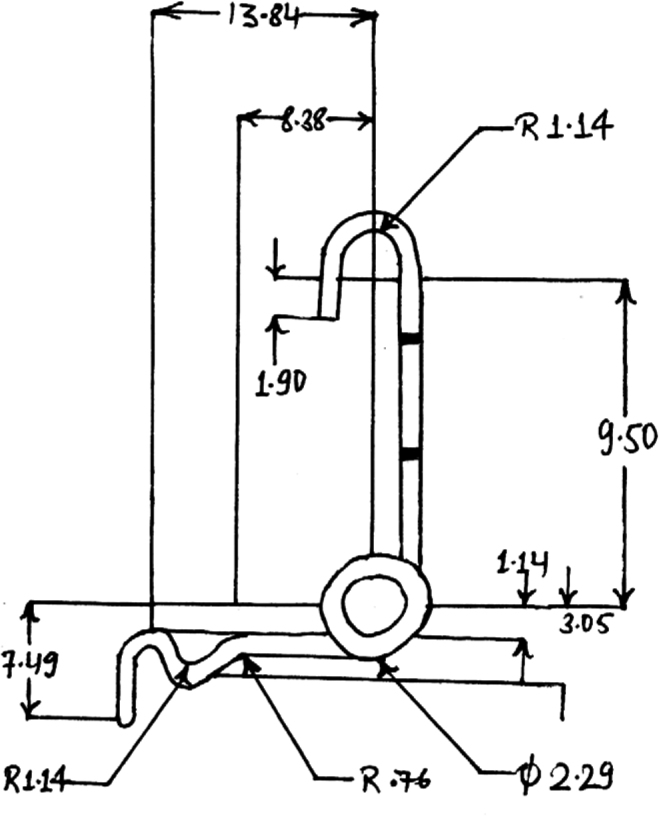
Dimensions of average pendulum spring in mm (actual span depends on palatal width).
The springs are extended close to the center of the palatal button to maximize their range of motion, allow easier insertion into the lingual sheaths and reduce forces to an acceptable range. Tongue irritation during swallowing is minimized by extending the springs distal to the button.
The anterior portion of the appliance is retained in place with occlusally bonded rests on the first and/or second bicuspids. In case, the second bicuspids are bonded then these rests can be removed later in treatment to allow the second bicuspid to drift distally (Fig 2).
Fig. 2.

Pendulum appliance at start of treatment
Preactivation and placement
The molar bands are cemented without the springs engaged. Once the appliance is in place, Pendulum springs are seated in the lingual sheath with the help of Weingart pliers.
Reactivation and stabilization
The patient should be seen every three weeks to monitor the spring pressure. The spring may be reactivated to the desired extent, if needed.
Once the molars have been moved distally (Fig 3), they are stabilized in their new position. It is imperative to move the buccal segments into a Class I relationship to harness the full advantage of the appliance. The upper molar bands are utilized to place a transpalatal bar or Nance appliance immediately after removal of the pendulum.
Fig. 3.

Pendulum appliance after distalisation of molars
The molars can be stabilized in any of the following ways:
-
1.
An upper utility arch holds the molars back with the incisors as anchorage. The buccal segments are then retracted, usually with elastomeric chain. A Nance button is used to augment anchorage.
-
2.
The second bicuspids, first bicuspids and cuspids are serially bonded. A 0.016” stainless steel arch wire is passed buccally with an open coil spring to apply reciprocal force to push the bicuspids (second then first) and the cuspids. Finally the anterior segment is bonded and the incisors are retracted with loop mechanics and the arch is consolidated (Fig 4).
Fig. 4.

Maxillary arch after retraction of cuspids
Diagnostic criteria
Since the Pendulum appliance drives the upper molars distally (with slight lingual tipping) quite rapidly, there is a tendency for the anterior bite to open. This open bite generally corrects itself in brachyfacial patients, but it can be a problem in dolichofacial types, especially those with tongue-thrust habits. It is still recommended to treat vertical growth patterns conservatively with extractions, directional headgears and transpalatal bars [2]. The bite-opening tendency can be encouraged in brachyfacial patients by bonding the Nance portion of the appliance to the occlusal surfaces of the bicuspids or deciduous molars.
Distal movement of the molars appear to be most efficient before the upper second molars have erupted. Unilateral Class II patients also benefit greatly from Pendulum therapy. There are some cases where forward positioning of one molar due to early loss of deciduous teeth and mesial drifting of the molar is the root cause of the malocclusion. A Pendulum spring on one side can regain space without putting undue strain on other parts of the upper arch.
A fixed rapid palatal expander with incorporated Pendulum appliance can accomplish dual purpose of rapid maxillary expansion and molar distalisation [3].
Limitations of Pendulum Appliance [4]
-
(a)
Torquing or rotation of molars: If the helix loop is not adjusted correctly, the pendulum spring can be distorted and can result in undesirable rotation or torquing of the molars.
-
(b)Tissue Irritation:
-
iFood and plaque accumulation under the palatal acrylic cause slight tissue inflammation. This does not limit the use of this appliance.
-
iiThe activated helix loop of the Pendulum springs cause anterior reciprocal forces to be generated against the palatal acrylic and the palate. With a larger palatal acrylic, the generated forces are spread over a wider area with minimal palatal irritation.
-
i
Conclusion
Patient tolerance of the Pendulum appliance is excellent. It is a very efficient technique to correct Class II malocclusion without resorting to extractions and with minimal patient compliance. It is simple and easy to fabricate, with minimal laboratory support. The cost of a Pendulum appliance is a fraction of the cost of commercially available molar distalization appliances. It may be routinely used in busy clinical practice.
References
- 1.Hilgers JJ. The Pendulum Appliance for Class II non-complaince therapy. J Clin Orthod. 1992;26:706–714. [PubMed] [Google Scholar]
- 2.Sfondrini MF, Cacciafesta V, Sfondrini G. Upper molar distalisation: a critical analysis. Orthodontics and Craniofacial Research. 2002;5(2):114–126. doi: 10.1034/j.1600-0544.2002.01155.x. [DOI] [PubMed] [Google Scholar]
- 3.Snodgrass David J. A Fixed Appliance for Maxillary Expansion, Molar Rotation and Molar Distalisation. J Clin Orthod. 1996;30:156–159. [PubMed] [Google Scholar]
- 4.Rondeau Brock HM. Pendulum Appliance. The Functional Orthodontist. 1994;14:4–10. [Google Scholar]