

Abstract
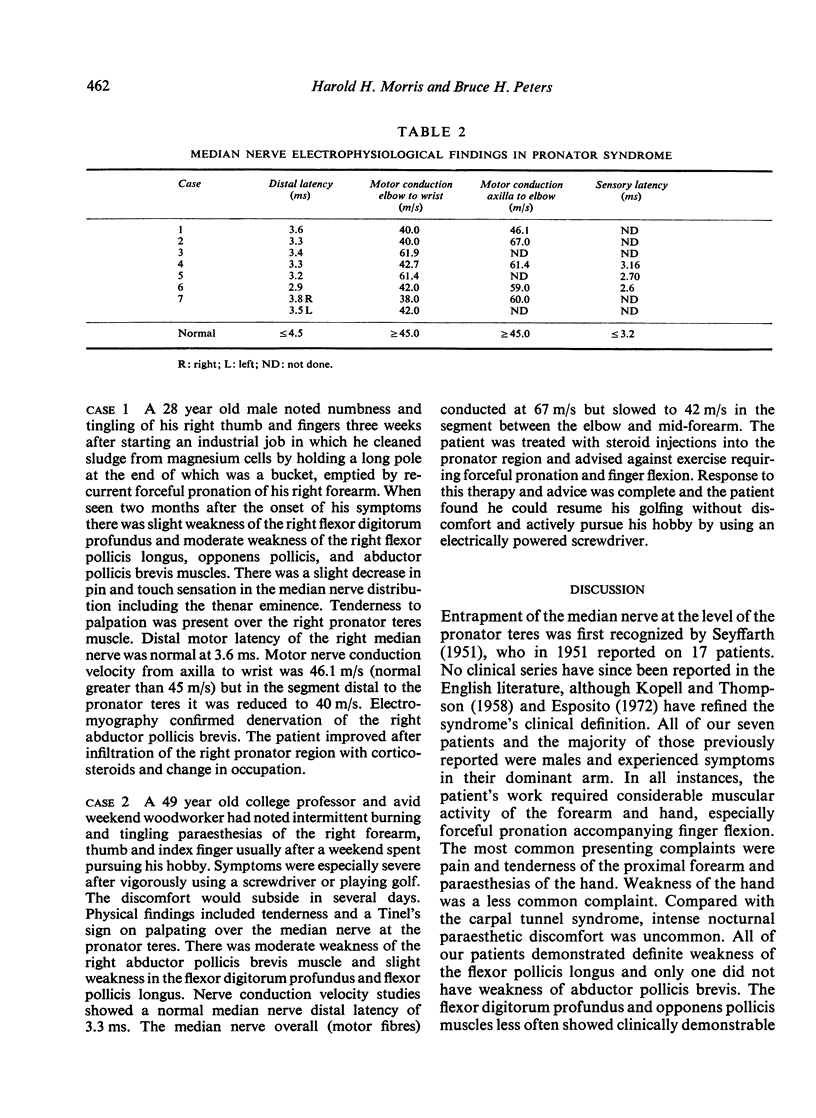
The clinical and electrophysiological picture of seven patients with the pronator syndrome is contrasted with other causes of median nerve neuropathy. In general, these patients have tenderness over the pronator teres and weakness of flexor pollicis longus as well as abductor pollicis brevis. Conduction velocity of the median nerve in the proximal forearm is usually slow but the distal latency and sensory nerve action potential at the wrist are normal. Injection of corticosteroids into the pronator teres has produced relief of symptoms in a majority of patients.
Full text
PDF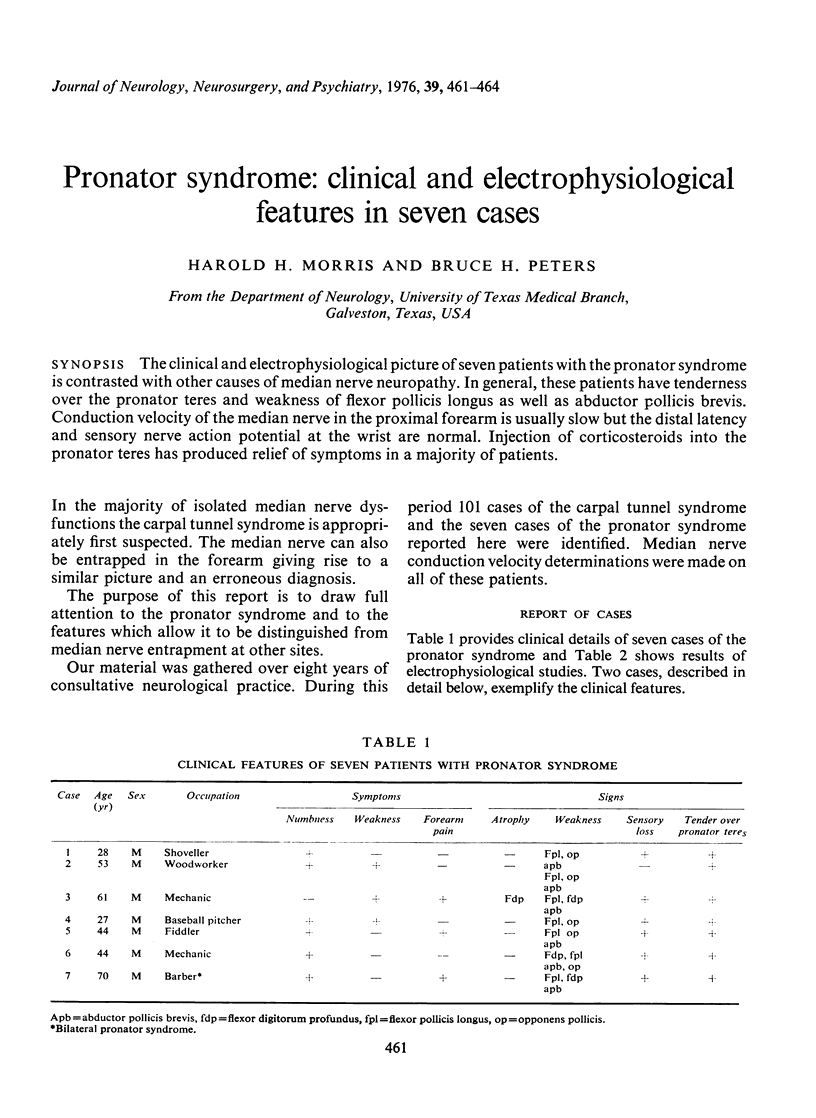
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Esposito G. M. Peripheral entrapment neuropathies of upper extremity. N Y State J Med. 1972 Mar 15;72(6):717–724. [PubMed] [Google Scholar]
- KOPELL H. P., THOMPSON W. A. Pronator syndrome: a confirmed case and its diagnosis. N Engl J Med. 1958 Oct 9;259(15):713–715. doi: 10.1056/NEJM195810092591503. [DOI] [PubMed] [Google Scholar]
- SEYFFARTH H. Primary myoses in the M. pronator teres as cause of lesion of the N. medianus (the pronator syndrome). Acta Psychiatr Neurol Scand Suppl. 1951;74:251–254. [PubMed] [Google Scholar]
- SOLNITZKY O. Pronator syndrome: compression neuropathy of the median nerve at level of pronator teres muscle. Georgetown Med Bull. 1960 May;13:232–238. [PubMed] [Google Scholar]