

Introduction
The Dandy-Walker complex is a rare congenital intracranial malformation that comprises a spectrum of abnormalities of the posterior fossa which are classified as (a) Dandy-Walker malformation (cystic dilatation of the 4th ventricle, complete or partial agenesis of the cerebellar vermis and an enlarged posterior fossa) (b) Dandy-Walker variant (cystic posterior fossa mass with variable hypoplasia of the cerebellar vermis and no enlargement of the posterior fossa) and (c) Mega-cisterna magna (enlarged cisterna magna with normal cerebellar vermis and fourth ventricle).
The prenatal sonographic diagnosis of the classic Dandy-Walker malformation is simple, however the definitive diagnosis of Dandy-Walker variant and Mega-cisterna magna is difficult before 18 weeks of gestation. This is because the sonographic appearance of normal cerebellum in the second trimester can resemble pathological anomalies as the posterior fossa structures are not established until then and the sonologist must exercise caution before reaching a final diagnosis of Dandy-Walker variant or mega-cisterna magna [1].
We report a case of Dandy-Walker variant which was diagnosed during routine antenatal ultrasonography at 22 weeks of gestation and subsequently confirmed by post natal CT scan of the brain.
Case Report
A 22-year old primi-gravida was referred for routine antenatal ultrasound at 22 weeks of gestation. The patient had no symptoms to offer and obstetrical examination revealed uterine size of 20-22 weeks. Ultrasonography revealed a single live intra-uterine gestation with biparietal diameter and foetal femur length corresponding to 22 weeks of gestation. The foetal posterior fossa was of normal size but with a large anechoic lesion which was communicating with the 4th ventricle. There was a suggestion of hypoplasia of the cerebellar vermis (Fig.1) but no evidence of hydrocephalus. There was no sonographic evidence of agenesis of the corpus callosum or any other congenital intracranial malformation. The patient was followed up till her delivery and no additional findings were detected in the subsequent ultrasound examinations. The patient delivered a female child at term with a birth weight of 2.8 kg. Physical examination of the baby did not reveal any congenital anomaly. Cranial ultrasound done immediately after birth revealed an anechoic posterior fossa mass lesion communicating with the 4th ventricle with evidence of vermian hypoplasia (Fig. 2, Fig. 3). Abdominal ultrasound revealed no abnormalities. CT scan done on the 2nd day after birth confirmed the ultrasound findings of a cystic posterior fossa mass communicating with the 4th ventricle and vermian hypoplasia (Fig.4). There were no other congenital intra or extra-cranial malformations. Echocardiography of the baby showed absence of any congenital cardiac defects. A final diagnosis of Dandy-Walker variant was made.
Fig. 1.
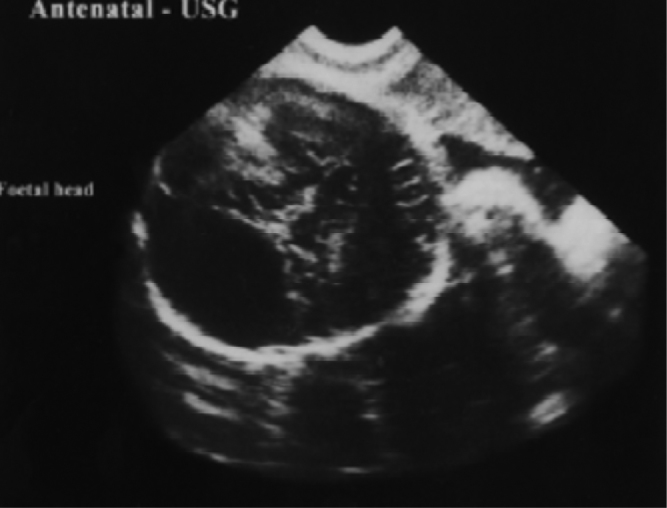
Antenatal ultrasonography showing a large anechoic mass lesion in the posterior fossa of the foetus
Fig. 2.
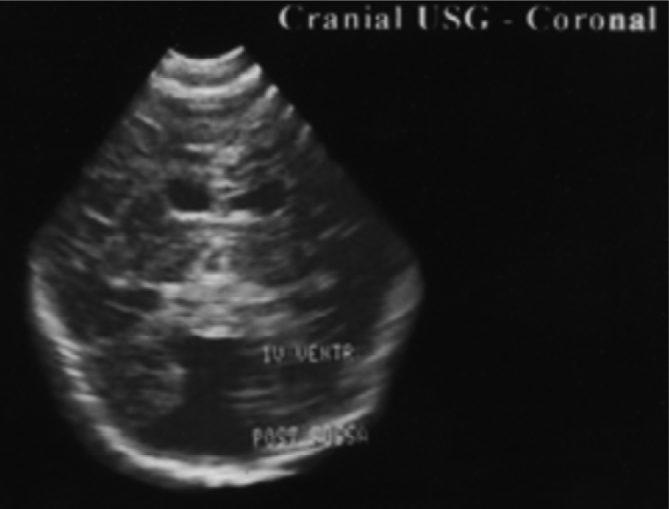
Cranial ultrasonography (coronal section) of the neonate showing a large posterior fossa anechoic mass lesion communicating with 4th ventricle
Fig. 3.

Cranial ultrasonography (sagittal section) of the neonate showing a large posterior fossa mass lesion with hypoplastic cerebellar-vermis
Fig. 4.
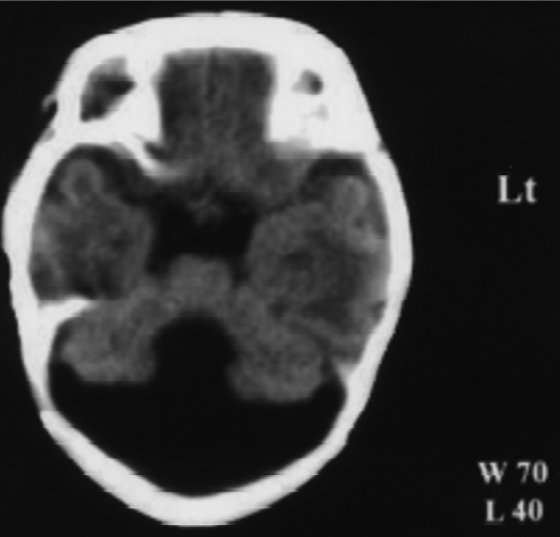
CT scan of the head showing a hypodense posterior fossa mass lesion communicating with the 4th ventricle and vermian hypoplasia
Discussion
The Dandy-Walker malformation is a term which represents not just a single entity, but several abnormalities of brain development which coexist. This disorder is a congenital brain malformation typically involving the fourth ventricle and the cerebellum which was first described in 1914 by W Dandy and K Blackfan and was designated as Dandy-Walker syndrome in 1954 by C Benda, who also reported familial occurrence [2]. The Dandy-Walker malformation has an estimated prevalence of about 1:30,000 live births with a slight female preponderance and is responsible for 4-12% of infantile hydrocephalus [3].
Dandy-Walker malformation is frequently associated with other intracranial anomalies such as agenesis of the corpus callosum, holoprosencephaly, occipital encephaloceles and ocular abnormalities. Extra-cranial anomalies include polycystic kidneys, cardiovascular defects, polydactyly and cleft palate. Postnatal studies indicate that the incidence of associated malformations range between 50 and 70% [4].
Genetic factors have a major role in the etiology of this condition. Dandy-Walker malformation may occur as part of Mendelian disorders and chromosomal aberrations. Environmental factors including viral infections, alcohol and diabetes have also been suggested to play a role in the genesis of Dandy-Walker malformation but the evidence is uncertain. In the absence of a recognizable syndrome a recurrence risk in subsequent pregnancies of 1-5% is suggested [4]. Prenatal sonographic diagnosis of the classical Dandy-Walker malformation is fairly simple; however, its differential diagnosis from other posterior fossa anomalies like mega-cisterna magna and retro-cerebellar arachnoid cyst is important. Dandy-Walker malformation is recognized by an enlarged posterior fossa, cystic posterior fossa mass communicating with the 4th ventricle and varying degree of vermian hypoplasia/agenesis. In this condition, borderline to overt ventriculomegaly and other neural/extra neural defects are generally present. Distinction between Dandy-Walker variant and mega-cisterna magna in the fetus is difficult as definitive criteria have not been firmly established. The former condition should be suspected when a thin communication is found between the fourth ventricle and the cisterna magna, the latter when the cisterna magna has a depth greater than 10 mm [5]. The prenatal differentiation between Dandy-Walker variant and mega-cisterna magna should be made with caution, especially in the early second trimester because the relatively large fourth ventricle and the incompletely formed inferior cerebellar vermis may give a false impression of vermian defect and a follow-up scan at 18 weeks or later is recommended. Even in the second and third trimester a scanning angle too steep, may create the impression of an excessive size of the cisterna magna and even of a vermian defect [5]. Retrocerebellar arachnoid cyst is a less common and more benign anomaly than Dandy-Walker malformation because in these cases the underlying brain is normal. The cerebellar hemispheres are not separated by a cystic mass, rather displaced en-bloc [6].
On the basis of available evidence it is believed that antenatal sonography allows a definitive diagnosis of only the severe anatomic varieties of the Dandy-Walker complex, those characterized by both a large posterior fossa cystic mass and a wide defect in the cerebellar vermis, referred to as classic Dandy-Walker malformation. It is difficult to solve prenatally the doubt of either a mega-cisterna magna or a small inferior defect of the vermis as in Dandy-Walker variant and this can only be resolved by post natal imaging studies.
References
- 1.Babcook CJ, Chong BW, Salamat MS, Ellis WG, Goldstein RB. Sonographic Anatomy of the developing Cerebellum: Normal Embryology can resemble pathology. AJR. 1996;166:427–433. doi: 10.2214/ajr.166.2.8553961. [DOI] [PubMed] [Google Scholar]
- 2.Benda CE. The Dandy-Walker syndrome or the so-called atresia of the foramen Magendie. J Neuropathol Exp Neurol. 1954;13:14–27. doi: 10.1093/jnen/13.1.14. [DOI] [PubMed] [Google Scholar]
- 3.Osenbach RK, Menezes AH. Diagnosis and management of the Dandy-Walker malformation: 30 years of experience. Pediatr Neurosurg. 1991;18:179–185. doi: 10.1159/000120660. [DOI] [PubMed] [Google Scholar]
- 4.Murray JC, Johnson JA, Bird TD. Dandy-Walker malformation: etiologic heterogeneity and empiric recurrence risk. Clin Genet. 1985;28:272–276. doi: 10.1111/j.1399-0004.1985.tb00401.x. [DOI] [PubMed] [Google Scholar]
- 5.Laing FC, Frates MC, Brown DL, Benson CB, Di Salvo DN, Doubilet PM. Sonography of the fetal posterior fossa: False appearance of Mega-Cistema magna and Dandy-Walker variant. Radiology. 1994;192:247–251. doi: 10.1148/radiology.192.1.8208946. [DOI] [PubMed] [Google Scholar]
- 6.Filly Roy A. Ultrasound evaluation of the foetal neural axis. In: Callen Peter W., editor. Ultrasonography in Obstetrics and Gynaecology. 3rd ed. WB Saunders; 1994. pp. 192–196. [Google Scholar]