

Abstract
This paper presents an evaluation and results of a study conducted on 62 patients out of 140 cases of chronic headache seen in ENT OPD. 32 patients were taken up for minimal endoscopic surgery. 23 cases (72%) have shown significant relief from headache over a period of 6 months or more. 11 cases showed anatomical / pathological variations at the ethmoidalis infundibulum, the commonest cause being enlarged bulla ethmoidalis followed by minimal polyps/polypoidal mucosa at the frontal recess area. Other causes are hyperplastic sinusitis, high posterior septal deviation, large middle turbinate, paradoxical middle turbinate and concha bullosa.
Key Words: Endoscopy, Headache
Introduction
Chronic headache is not an uncommon malady, distressing for both the patient and the physician; to the former due to its nagging nature and to the latter for his inability to diagnose and for problems of self medication in a lot many cases. Since the causes of headache are multifactorial varying from simple tension headache, migraine, to sinister myofacial spasm and temporomandibular joint arthralgia, vascular headache, refractory errors, and brain tumors, it requires a multidisciplinary approach to diagnose the causative factors. Headache may remain undiagnosed in spite of detailed examination and elaborate battery of tests. Some of these undiagnosed cases may be of rhino-sinugenic origin even when the cause is not suspected on preliminary evaluation.
Cold light nasal endoscopy in association with computed tomographic scanning (CT Scan) has opened new vistas in peeping into inaccessible areas and niches of fronto-ethmoid complex and sphenoid sinus. Small lesions and / or anatomical variations undetected clinically and by conventional radiography present in the walls of intricate ethmoid complex may give rise to headache especially when located in key area of ethmoidal infundibulum and frontal recess. The development of intense contact of opposing mucosal surfaces due to many anatomical variations leads to hampered ciliary activity and flow of mucus drainage from ethmoid and other paranasal sinuses. Identification of these anatomical-pathological causes by diagnostic endoscopy and CT scanning followed by minimal surgical intervention by functional endoscopic sinus surgery (FESS) can provide dramatic relief from headache and associated symptomatology present for months and years.
Material and Methods
A total of 140 cases of chronic headache out of over 4390 (3%) were seen in ENT outpatient in the year 1998. 78 (56%) patients were found to have some systemic cause for headache and were thus excluded from this study. Patients with obvious frank rhinological symptom attributable to headache have also not been included in the study. 62 (44%) patients of chronic headache were then subjected to detailed ENT examination. The youngest patient was 15 years and oldest 52 years. All the patients were suffering from headache varying from 6 months to 8 years time. Headache was present in temporal, frontal, vertex, neck and malar region in isolation or in combination of more than one location. It was intermittent with exacerbations, recurrent episodic or continuous dull ache. All the patients were subjected to detailed history taking, clinical and systemic examination prior to otorhinological examination to rule out any systemic causes like hypertension, migraine, tension headache, neurological causes, ophthalamological examination to rule out refractory errors, gynaecological check up to eliminate premenstrual tension and premenopausal syndrome as cause of headache. ENT examination consisted of detailed history of headache, its periodicity, intensity, localization, precipitating factors, associated symptoms like nausea, vomiting, nasal block, rhinorrhoea, anosmia, epistaxis, and snoring. Anterior and posterior rhinoscopy was done to assess and evaluate any anatomical variation or pathological lesion. X-ray paranasal sinuses standard view and additional views if required were done to rule out any paranasal pathology. Routinely this was followed by diagnostic endoscopy under local anaesthesia. CT scan was ordered in patients who were found to have some evidence of pathology or anatomical variation in osteomeatle complex or was a preoperative requirement when therapeutic endoscopy was considered as a roadmap for surgery. After a complete work up a total of 32 out of 62 patients (52%) were taken for functional endoscopic surgery.
Results
Out of a total of 62 patients subjected to diagnostic endoscopy 13 (21%) cases had pathological mucosa and 29 (47%) were seen to have a typical structure of lateral nasal wall (Table 2). Joe et al have shown much larger ratio of atypical lateral nasal wall [1]. 19 of these 29 cases (65%) were seen to cause significant mucosal contact of opposing surfaces or narrowing of osteo meatle complex/frontal recess area. 13 cases had pathological mucosa consisting of small polyps or polypoidal mucosa in middle meatus, middle turbinate or frontal recess in addition to thickened sinus mucosa and antral cysts. Out of these 32 cases (a) 11 cases were seen leading to narrowing of hiatus semilunaris amongst which – 6 had large bulla ethmoidalis, 4 prominent and large medially rotated uncinate process and one case of paradoxical turbinate. Infundibulotomy with anterior ethmoidectomy and wedge resection of middle turbinate in one case was done to reduce the contact of mucosal surfaces. 4 cases had large and prominent Agar nasi cells which needed exentration to clear the blocked frontal recess. Conchectomy was done in 2 cases of concha bullosa. 2 cases underwent submucosal resection of high septal deviation (b) 6 cases were seen to have small polyps/polypoidal mucosa endoscopically and / or on CT scan in the frontal recess area, middle meatus and antrum. Polypectomy was done in these cases. 3 cases of antral cysts were treated by puncturing of cyst with a pointed cannula tube through sinoscope and suction of its contents, (c) 4 cases had hyperplastic sinusitis with blocked or narrow ostium. Infundibulotomy with widening of ostium and sinoscopy to visualise the mucosa only was done in these cases.
Table 1.
Age and sex distribution
| Age group | Diagnostic endoscopy | Functional sinus surgery |
|---|---|---|
| Sex ratio | N-62 | N-32 |
| 15-25 years | 16 | 8 |
| 25-40 years | 35 | 14 |
| Above 40 years | 11 | 10 |
| Male:Female | 27:35 | 15:17 |
Fig. 1.
Large Agar nasi cells bilateral. These appear as air spaces anteriorly and superiorly on lateral nasal wall before visualization of middle turbinate when examining coronal plane of CT scan from anterior to posterior. Frontal recess seen blocked with opacification of left frontal sinus
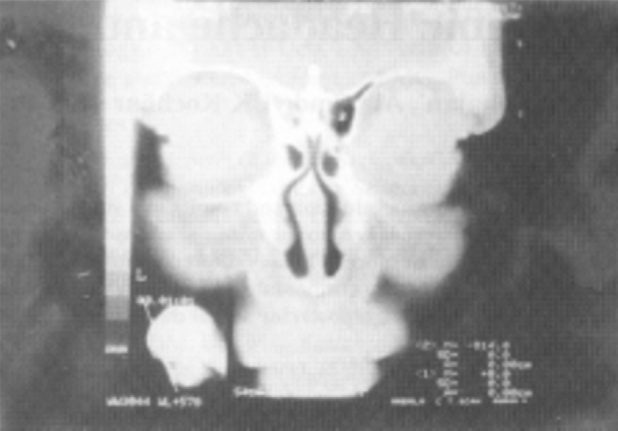
Fig. 2.

Concha bullosa of left middle turbinate. Both anterior ethmoid cells are partially opacified including left frontal sinus. Left infundibulum is narrower compared to right
Table 2.
Results of diagnostic endoscopy anatomic variations N-62
| Present study |
Joe, et al 2000 |
||||
|---|---|---|---|---|---|
| Anatomic variant | Typical | Atypical | Typical | Atypical | |
| (%) | (No) | ||||
| Middle turbinate | 92% | 8% | (5) | 63% | 37% |
| Concha bullosa | (3) | ||||
| Paradoxical turbinate | (1) | ||||
| Bifid turbinate | (1) | ||||
| Uncinate process | 90% | 8% | (5) | 85% | 15% |
| Ethmoid bulla | 85% | 15% | (9) | 45% | 55% |
| Ballooned | (9) | ||||
| Agar nasi cells (large) | 94% | 6% | (4) | − | |
| Accessory ostium | 94% | 6% | (4) | 15% | |
| High septal posterior deviation | 97% | 3% | (2) | − | |
| Total | 46% | (29) | |||
23 (72%) cases reported relief after FESS for a period of six months or more. 6 cases reported no relief and 3 cases were lost to follow up. 2 cases reported with recurrence of polyps and were put on steroid spray (Beclomethasone) with significant relief. One case was found to have scleroma of maxillary and ethmoidal sinus and was treated accordingly. Thus 10 out of 13 cases (77%) with pathological mucosa improved on endoscopic treatment whereas 13 of 19 cases (68%) including those lost to follow up (presumed failed) with anatomical atypical structure responded to minimal endoscopic management.
Discussion
Headache is the 9th most common symptom that brings a patient to a physician and agonizes both the sufferer and physician equally [2]. Though it has been described in old literature some 5000 years back, the management continues to remain a dilemma due to its ill known aetiopathogenesis [3]. In the year 1988 The International Headache Society (IHS) constituted a headache classification committee which has laid down broad diagnostic criteria for headache disorders and facial pain [4]. The classification is used for research purposes to maintain uniformity in diagnostic criteria. The easiest and simplest way to treat a headache patient is to categorize all acute, subacute and chronic headaches into primary and secondary headaches. With the present day understanding of pathophysiology and newer modalities of investigations it is possible to pin point an attributable secondary cause in many cases, however many case will fail to reveal any abnormality. Such cases are labelled as primary headaches. These cases are more chronic and intractable and where no overt cause is known even after maximal detailed systemic examination by general physician, ophthalmologist, dentist, neurophysician and even gynaecologist. Some of these cases may have their origin of headache in the intricate region of nose and paranasal sinuses. With the help of CT scanning and fibreoptic nasal endoscopy it may be possible to have an access and visualization of the niches and narrow spaces in this region. The role of endoscopist in association with study of CT scan would be to locate the possible trigger area in sinonasal area which initiates the pain reflex.
There are nociceptor peripheral nerve receptors conveying information of noxious stimuli, mechanoreceptive neurones responsible for non-noxious stimuli and the third type of wide dynamic range receptors stimulated by both noxious and non-noxious stimuli present in the head and neck region including the nasal mucosa and cutaneous dermatomes. These peripheral receptors carry sensation to central corticle area in the sensory nucleus of Trigeminal nerve. In the ultimate analysis, the central cortex may cross localize the mucosal pain to the dermatome and hence the referral of sinugenic pain to other areas of head and neck. The sensitivity of these receptors is initiated, altered or enhanced by various chemical irritants released by local tissue injury. The studies of Wolff, Dalessian and Greenfield have shown that vascular engorgement in response to tissue injury leads to release of vasoactive amines. Apart from neurotransmitters like noradrenaline and acetylcholine, neuropeptides have been found to be responsible for induction of pain. Substance P (SP) is the common neuropeptide which has strong vasodilatory effect along with plasma extravasation, hypersecretion and smooth muscle contraction. The release of SP can be triggered by stimuli such as chemicals, infections, thermal irritants and even mechanical pressure. SP mediates pain from receptors of mucosa through unmyelinated C fibres to cortex [5,6]. Identification of such intranasal and sinus lesions leading to close contact of mucosal area or subclinical infections will help the endoscopist to reduce the trigger area. The hall mark of the nasal and paranasal physiology is (a) proper ventilation of paranasal sinus through natural ostium and (b) movement of mucus blanket by ciliary beating towards ostium.
Osteo-meatle complex is the key area in which maxillary sinus drains through its ostium inferiorly and frontal sinus through frontal recess superiorly. Any anatomical variation or pathology in the narrow area of infundibulum is likely to clog the sinuses and lead to malventilation. The presence of narrow spaces also precludes establishing of close contact of opposing mucosal surfaces which in turn hinder the normal flow of mucous blanket. Consequent to impaired ciliary mobility the stagnant mucus blanket acts as nidus for infection. A vicious cycle of congestion, mucosal oedema, resultant mechanical pressure and / or narrowing of ostia and malventilation may set in consequently. Depending upon the state of anatomical disposition and pathology the patient may present with frank disease or manifest as nasal discomfort, fullness or headache. The cause of such headache is attributed to :
-
(a)
Malventilation of sinuses leading to local hypoxia, reduced pH, reduced ciliary beat and thick viscous mucus and increased vulnerability to infections.
-
(b)
Constant intense mucosal contact leading to referred pain.
-
(c)
Pressure from proliferating polyps.
The diagnosis and treatment of such cases will lie in the realm of nasal endoscopist. A detailed anterior and posterior rhinoscopy examination and conventional radiogram should be followed by diagnostic endoscopy under careful local anaesthesia and vasoconstriction. Any anatomical abnormalities which by themselves may not be pathological are noted. The endoscopy will invariably be supplemented by CT scan of paranasal sinuses. Once the atypical offending anatomical / pathological area in the lateral nasal wall is delineated a minimal conservative resection of the areas is done as per standard Messenger Klinger technique.
The aim of the surgery would be to improve ventilation of sinuses by clearing the blockage of sinus / ostia. Common variations which have been found in this study and are responsible for the blocking of ethmoidal infundibulum are enlarged bulla, enlarged middle turbinate, high posterior septal deviation, narrow frontal recess due to pneumatised or over riding Agar nasi cells and frontal cells. In frontal sinus, opening the lower anterior ethmoid cells and the Agar nasi cells have reversed the frontal recess blockage. Jacob in his study has shown that the symptoms of sinusitis have improved even in the presence of disease as shown by CT scan by opening the blockage by clearing the recess without touching the frontonasal ostium or sinus [7].
To conclude, functional endoscopic sinus surgery is not a procedure but a concept of diagnosis of functional status of nasal and paranasal sinuses as well as surgical treatment of functional and anatomical variants including the post operative follow up. Minimal conservative resection of anatomical abnormalities which per se may not be disease entities or small pathological lesions in intricate lateral wall of nose may only be required to alleviate chronic intractable headache.
References
- 1.Joe JK, Steven YH, Yanagisawa E. Documentation of variation in sinonasal anatomy by intraoperative nasal endoscopy. Laryngoscope. 2000;110:229–235. doi: 10.1097/00005537-200002010-00008. [DOI] [PubMed] [Google Scholar]
- 2.Bellanger JJ. Headache and Neuralgia of Face. In: Bellanger John J, Snow James B., editors. Otorhinolaryngology and Head Neck Surgery. 15th ed. Williams And Wilkins; Philadelphia: 1996. pp. 158–162. [Google Scholar]
- 3.David RA. Headache in adolescent: Diagnosis and management. Med Clin North Am. 1991;75:653–660. doi: 10.1016/s0025-7125(16)30440-0. [DOI] [PubMed] [Google Scholar]
- 4.The Headache Classification committee of the International Headache Society Classification and diagnostic criteria for Headache disorder, Cranial neuralgia and facial pains. Cephalgia. 1988;8(suppl):1–96. [PubMed] [Google Scholar]
- 5.Acquadro MA, Montgomery WW. Treatment of Chronic Paranasal Sinus Pain with Minimal Sinus Disease. Ann Otol Rhinol Laryngol. 1996;105:607–614. doi: 10.1177/000348949610500804. [DOI] [PubMed] [Google Scholar]
- 6.Stammberger H, Wolf G. Headaches and Sinus Disease: The endoscopic approach. Ann Otol Rhinol Laryngol. 1988;134(suppl):3–23. doi: 10.1177/00034894880970s501. [DOI] [PubMed] [Google Scholar]
- 7.Seiden AM, Stankiewich JA. Frontal Sinus Surgery: The state of the Art. Am J Otolaryngology. 1998;19:183–193. doi: 10.1016/s0196-0709(98)90086-2. [DOI] [PubMed] [Google Scholar]