

Abstract
Background and Objectives
There is strong empirical support that individuals with elevated social anxiety are at risk for alcohol-related impairment. Because social anxiety is a multi-faceted construct, it is important to consider which specific facets contribute to alcohol problem vulnerability. For example, although social anxiety has traditionally been conceptualized as a fear of negative evaluation (FNE), emerging data suggest that fear of positive evaluation (FPE) is also an important factor in pathological social anxiety. The current manuscript reports novel findings regarding FPE, alcohol use motives, and reported alcohol use problems.
Design and Methods
Participants included undergraduates from two American universities (n = 351) who completed a battery of measures assessing fears of evaluation, drinking motives, and alcohol usage related problems.
Results
FPE significantly predicted alcohol use problems, above and beyond FNE. Also, coping and conformity motives for drinking, but not social or enhancement motives, each uniquely mediated the relationship between FPE and alcohol use problems.
Conclusions
FPE may be an important cognitive-affective vulnerability factor. With additional clinical research, FPE could serve as a meaningful therapeutic target in interventions designed to decrease problem drinking among highly socially anxious patients.
Keywords: Alcohol, drinking motives, social anxiety, social phobia, fear of positive evaluation, fear of negative evaluation
Social anxiety is uniquely associated with alcohol-related problems including alcohol use disorders (AUD; for reviews see Buckner, Heimberg, Ecker, & Vinci, 2013; Morris, Stewart, & Ham, 2005). To illustrate, in the National Epidemiologic Survey on Alcohol and Related Conditions, nearly half of individuals with a lifetime diagnosis of social anxiety disorder (SAD) met criteria for an AUD (Grant et al., 2005), and adolescents with SAD were five times more likely to develop an AUD in early adulthood (Buckner et al., 2008). In the National Comorbidity Survey, SAD was associated with higher rates of AUD than most other anxiety disorders (Kessler et al., 1997) and remained related to AUD after controlling for other Axis I disorders (Buckner, Timpano, Zvolensky, Sachs-Ericsson, & Schmidt, 2008). In prospective analyses, when anxiety and mood disorders were entered simultaneously, only SAD remained significantly related to the development of AUD (Buckner, Schmidt, et al., 2008). Elevated social anxiety in non-clinical samples has also been associated with greater alcohol-related problems (e.g., Buckner, Eggleston, & Schmidt, 2006; Buckner & Heimberg, 2010; Gilles, Turk, & Fresco, 2006; Lewis & O'Neill, 2000). The co-occurrence between social anxiety and alcohol-related problems is related to greater impairment than either condition alone (e.g., Buckner, Timpano, et al., 2008; Schneier et al., 2010). Thus, identification of factors related to alcohol-related problems among socially anxious individuals could have important treatment and prevention implications.
To understand why individuals with social anxiety (as opposed to other types of anxiety or negative affect more broadly) appear to be at such high risk for alcohol-related impairment, research has begun to examine whether there is something about the nature of social anxiety itself that contributes to alcohol problem vulnerability (e.g., Buckner & Heimberg, 2010; Thomas, Randall, & Carrigan, 2003). Although tension-reduction-based models of substance-related impairment posit that some socially anxious persons may rely on alcohol to help manage chronically elevated negative affect, data have been mixed. Specifically, individuals with elevated social anxiety report using alcohol in situations involving negative affect, and using alcohol in this way mediated the relation between social anxiety and alcohol-related problems (Buckner, et al., 2006). Further, social anxiety has been related to coping motives for alcohol use (Blumenthal, Leen-Feldner, Frala, Badour, & Ham, 2010; Lewis et al., 2008; Stewart, Morris, Mellings, & Komar, 2006). Yet, not all studies find social anxiety to be related to coping motives (Buckner, et al., 2006; Ham, Bonin, & Hope, 2007). In examination of whether socially anxious individuals use substances to cope specifically with their social anxiety, two studies confirm that social anxiety is related to drinking to cope specifically with social anxiety (Buckner & Heimberg, 2010; Thomas, et al., 2003).
Furthermore, individuals with social anxiety are more susceptible to engage in social comparison and submission to peers (e.g., Gilbert, 2000). Although there is mixed evidence as to whether social anxiety is related to conformity motives (Buckner, et al., 2006; Buckner & Shah, 2015; Lewis, et al., 2008; Stewart, et al., 2006), some evidence suggests that drinking to socially conform, in addition to coping motives, mediates the relationship between social anxiety and alcohol related problems for college students (Buckner & Shah, 2015; Lewis, et al., 2008). Yet, these approaches neglect to consider that social anxiety is a multi-faceted construct, and it may be that specific types of social fears place individuals at greatest risk for drinking to cope with negative affect broadly and to fit in with peers.
Social anxiety disorder is characterized by fear of scrutiny in social and/or performance situations (American Psychiatric Association, 2013). This fear of scrutiny is often conceptualized as a fear of negative evaluation (FNE), and past findings indicate that coping and conformity drinking motives may mediate the relationship between FNE and alcohol use problems (Stewart et al., 2006). One promising, although understudied, facet of social anxiety relative to FNE is fear of positive evaluation (FPE; Weeks, Heimberg, Rodebaugh, & Norton, 2008). FPE pertains to apprehension and distress about others’ positive evaluations of oneself. As proposed by Weeks and colleagues (2008; Weeks & Howell, 2014), FPE may derive in part from psycho-evolutionary-based tendencies to perceive oneself as falling lower in social rank relative to others (e.g., see Gilbert, 2001), as well as concomitant concerns of social reprisal from socially dominant others for standing out in a positive light (Weeks, Heimberg, Rodebaugh, & Norton, 2008). Accordingly, FPE and FNE may serve distinct, adaptive goals. Individuals who perceive themselves as ranking socially lower than others may be motivated to (a) avoid giving such a positive impression that they would be viewed as a threat by other members of the group (i.e., FPE), while also motivated to (b) not appear so socially undesirable as to be ostracized (i.e., FNE; see Weeks, Rodebaugh, Heimberg, Norton, & Jakatdar, 2009). In other words, highly socially anxious individuals feel compelled to be as inconspicuous as possible in feared social situations. Although FPE is significantly related to FNE (with both FPE and FNE significantly related to social anxiety; see Weeks, Norton, & Heimberg, 2009), these constructs are statistically distinct (Fergus et al., 2009; Weeks, Heimberg, Rodebaugh, Goldin, & Gross, 2012; Weeks, Jakatdar, & Heimberg, 2010), and maintain separate, trait-like components over time (Rodebaugh, Weeks, Gordon, Langer, & Heimberg, 2012). Altogether, SAD may be conceptualized as a psychological disorder involving fear of evaluation in general (i.e., bivalent fear of evaluation model; Weeks & Howell, 2012).
No known research has been conducted regarding the relationship between FPE and drinking. However, some self-report data suggest that undergraduates perceive moderate drinking to be associated with greater dominance and disinhibition (Southwick, Steele, Marlatt, & Lindell, 1981), suggesting that alcohol may actually reduce the effects of FPE on expectations of social anxiety-related submissive behavior (Weeks et al., 2010). Moreover, comparative data show that subdominant rats are at higher risk of alcohol abuse-like behavior, particularly in the presence in socially dominant rats (Duncan et al., 2006). Also, groups of both male and female rats that have continual access to alcohol are significantly less likely to form dominance hierarchies, versus rats not exposed to alcohol (Duncan et al., 2006). Another study (Filatova, Egorov, Shnitko, & Afanasiev, 2008) found that when caging together rats that previously exhibited dominant or submissive gestures, and when forcing intoxication among these rats, the number of hierarchical gestures no longer significantly differed among rats of different social rank. These comparative findings provide fairly compelling evidence that alcohol use may collectively reduce dominance behaviors among group members, or even increase affiliative behavior. Accordingly, individuals with higher FPE may use alcohol to not only cope with their chronically elevated negative affect in social situations (e.g., see Buckner, Eggleston et al., 2006); they may also perceive social events which include alcohol (e.g., college parties) as less socially threatening than social events without alcohol, thereby drinking to fit in with peers and/or easily acquiescing to peer-pressure to drink. The aim of the current dual-site study was to elucidate the relationships between FPE and drinking in several ways. First, we tested the hypothesis that FPE would be uniquely related to alcohol-related problems after accounting for the variance attributable to FNE. Second, we tested whether FPE would be related to drinking to cope with negative affect and to conformity motives. Third, we tested whether these drinking motives mediated the relation between FPE and drinking problems, beyond other motives for drinking.
Method
Participants and procedures
After giving informed consent, undergraduates at two universities in different regions of the USA completed a battery of questionnaires and received partial course credit: Southern (i.e., Louisiana State University; n = 184; Mage = 20.4; 82.1% female; 85.9% Caucasian) and Midwestern (i.e., Ohio University; n = 189; Mage = 19.09; 70.7% female; 92.8% Caucasian). Participants (N = 353) included individuals who reported drinking at least one alcoholic drink in a typical week, and who completed all measures in the present study (see Measures). Two participants were excluded, as their reported number of drinks in typical weeks (e.g., 145) were extreme outliers within our samples, yielding a total study sample of 351 (Mage = 19.79; 76.6% female; 89.2% Caucasian). The present study was approved by the human research ethics committees at both recruitment sites.
Measures
Measures of Evaluative Fears
Brief Fear of Negative Evaluation Scale—Straightforward Items (BFNES-S)
The BFNE-S (Leary, 1983) is a self-report measure of fear and distress related to negative evaluation from others. Rodebaugh et al. (2004) and Weeks et al. (2005) have recommended excluding the reverse-scored items from the BFNE score. The BFNES-S has demonstrated excellent internal consistency, factorial validity, and construct validity in undergraduate (Rodebaugh et al., 2004) and clinical (Weeks et al., 2005) samples. The BFNES-S demonstrated excellent internal consistency for both sites in the current study (both αs = .92).
Fear of Positive Evaluation Scale (FPES)
The FPES (Weeks, Heimberg, & Rodebaugh, 2008) assesses trait levels of FPE (e.g., “I am uncomfortable exhibiting my talents to others, even if I think my talents will impress them”). The FPES has demonstrated strong internal consistency, good 5-week and 4.5-month test-retest reliability, treatment sensitivity, and strong convergent, discriminant, and factorial validity (Fergus et al., 2009; Rodebaugh et al., 2012; Weeks, Heimberg, & Rodebaugh, 2008; Weeks et al., 2012). The FPES demonstrated acceptable (Site 2: α = .76) to good (Site 1: α = .80) internal consistency for the current study.
Alcohol use measures
Drinking Motives Questionnaire – Revised (DMQ-R)
The DMQ-R (Cooper, 1994) measures self-reported frequency of drinking, as driven by different motives, over the past 90 days. Four subscale scores each reflect one motive: coping motives (e.g., “you feel more self-confident or sure of yourself”), conformity motives (e.g., “to fit in with a group you like”), enhancement motives (e.g., “it's exciting”), and social motives (e.g., “it makes social gatherings more fun”). The DMQ-R demonstrates high internal consistency, as well as good factorial and criterion validity (Cooper, 1994; McLean & Lecci, 2000). For both samples, all four subscales demonstrated good to excellent internal consistency (all αs ≥ .87).
Daily Drinking Questionnaire-Revised (DDQ-R)
The DDQ-R assesses daily quantity and frequency of standard drink consumption during a typical or heavy week in the past 30 days (Collins, Parks, & Marlatt, 1985). DDQ-R items have demonstrated adequate test-retest reliability (Borsari & Carey, 2000) and convergent validity (Morean & Corbin, 2008). The DDQ-R was utilized to determine average quantity of alcohol consumption per day that alcohol was consumed, calculated by dividing the total number of drinks in a typical week by the number of drinking days in a typical week (e.g., see Buckner et al., 2006) (hereafter, typical alcohol consumption).
Rutgers Alcohol Problems Index (RAPI)
Alcohol-related problems were assessed using the past-month version of the RAPI (White & Labouvie, 1989), which has demonstrated adequate psychometric properties (Buckner, et al., 2006; White & Labouvie, 1989). As in previous work, endorsed items were summed to provide a total count of problems (e.g., Morean & Corbin, 2008). The RAPI demonstrated excellent internal consistency (both αs = .94).
Results
Assumptions of normality for all parametric tests were assessed and addressed. 1 Means and standard deviations are presented in Table 1.
Table 1.
Bivariate correlations among all study variables.
| Measure | 1. | 2. | 3.b | 4. | 5. | 6.b | 7. | 8.b | 9. | 10. | M | SD |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Sex (0 = Female; 1= Male) | — | |||||||||||
| 2. Age2 | −.03 | — | 19.72 | 3.22 | ||||||||
| 3. Typical alcohol consumptionb | .34* | .01 | — | 4.31a | 2.32 | |||||||
| 4. Fear of Positive Evaluation | .04 | .01 | .07 | — | 26.53 | 12.72 | ||||||
| 5. Fear of Negative Evaluation | −.03 | −.06 | .01 | .50* | — | 22.48 | 7.53 | |||||
| 6. Alcohol Use Problemsb | .11 | −.03 | .37 | .24* | .13 | — | 5.54a | 5.77 | ||||
| 7. Coping Motives | −.01 | −.04 | .22* | .29* | .30* | .41* | — | 13.61 | 5.94 | |||
| 8. Conformity Motivesb | .13 | −.03 | .09 | .26* | .27* | .28* | .46* | — | 9.64a | 5.52 | ||
| 9. Social Motives | .07 | .01 | .26* | .12 | .19* | .28* | .45* | .30* | — | 19.37 | 6.05 | |
| 10. Enhancement Motives | .06 | −.01 | .38* | .01 | .12 | .29* | .42* | .14 | .67* | — | 19.21 | 5.81 |
Preliminary analyses
Preliminary analyses indicated that participants at the Midwestern site, versus Southern site, reported greater typical alcohol consumption (i.e., by about one drink per week), t (349) = −3.58, p < .001, d = −0.38, weaker social and enhancement drinking motives, both ts ≥ 2.38, both ps ≤ .02, both ds ≥ 0.25, and were younger by about one year on average, t (349) = 1.43, p = .001, d = 0.15. 2 There was also a significant difference in composition of self-reported sex, such that there was a lower percentage of females at the Midwestern site, χ2 (1) = 5.48, Phi = −0.13. There were no other significant variable differences between sites, all ps ≥ .15. Due to these differences across our subsamples, recruitment site was entered as a covariate in the primary analyses.
Relations between FNE, FPE, and drinking behaviors
Bivariate correlations are presented in Table 1. Both FPE and FNE were positively correlated with number of drinking problems and with coping, conformity, and social motives. Also, FNE but not FPE was positively related to enhancement motives. Neither FPE nor FNE was significantly correlated with typical alcohol consumption. Lastly, all four coping motives, typical alcohol consumption, and participant sex were positively related to alcohol use problems.
FPE and FNE were simultaneously entered as predictor variables into a linear regression equation to examine the unique relations of these variables with alcohol-related problems. Recruitment site, sex, and typical alcohol consumption were entered as covariates. The full model was significant, F (5, 345) = 15.87, p < .001, with a medium-to-large multivariate effect, Cohen's f2 = .23. Only FPE remained significantly related to drinking problems, β = .20, p < .001, sr2 = .03 (FNE: β = .03, p = .57, sr2 = .0007). 3
Mediation analyses
Given that FPE was robustly related to greater drinking problems, we tested whether relevant drinking motives mediated the relation between FPE and alcohol-related problems. A multiple mediation model was tested, using a bootstrapping method with 5,000 bootstrap resamples (Preacher & Hayes, 2008). Bootstrapping is a nonparametric method that generates confidence intervals (CIs) for each mediator of the model—estimating the total, as well as the specific, indirect effects of those mediator variables. Bias-corrected and accelerated (BCa) 95% CIs were utilized for the present study. If zero is not within an estimated CI, then the indirect effect differs significantly from zero; the mediator variable(s) can then be concluded to mediate the relationship between the independent and dependent variables, while controlling for other mediator variables and other covariates (e.g., Preacher & Hayes, 2008). The four alcohol use motives were simultaneously entered as the mediator variables, to account for indirect effects of all motives (Preacher & Hayes, 2008). Site, sex, and typical alcohol consumption were entered as covariates.
See Figure 1 for direct, indirect, and partial effects. FPE was significantly and positively related to social, coping, and conformity motives (a paths). Only coping and conformity motives were significantly related to alcohol problems, in the presence of other motives (b paths). Of the covariates, only typical alcohol consumption had a significant partial effect on the relationship between FPE and alcohol problems. Among the mediators, coping and conformity motives had significant, unique indirect effects on the relation between FPE and alcohol use problems (see Table 2).4 Contrast effects indicated that the unique indirect effect of coping motives, but not conformity motives, was significantly stronger than the effects of either social or enhancement motives (see Table 2). There was no significant difference between coping and conformity motives.
Figure 1.
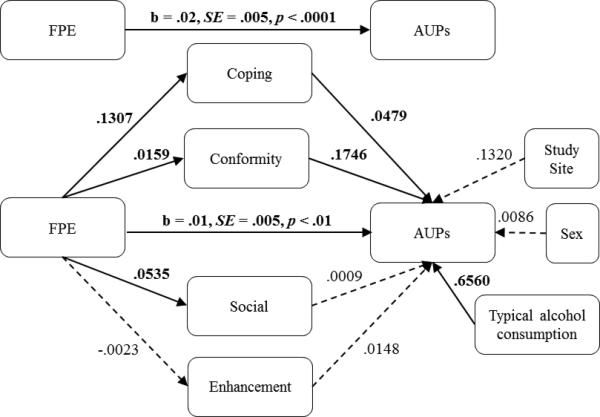
Graphical depiction of beta weight paths in testing multiple mediation effects of alcohol use motives on fear of positive evaluation and alcohol use problems, controlling for recruitment site, sex, and typical alcohol consumption.
Note: Bold font = p < .05; FPE = fear of positive evaluation; AUPs = alcohol use problems.
Table 2.
Mediation effects of drinking motives on fear of positive evaluation and alcohol use problems
| BCa 95% CI |
||||
|---|---|---|---|---|
| Point Estimate (a path*b path) | SE | Lower | Upper | |
| Indirect Effects | ||||
| Coping Motives | .0063 | .0021 | .0029 | .0113 |
| Conformity Motives | .0028 | .0017 | <.0001 | .0069 |
| Social Motives | <.0001 | .0007 | −.0015 | .0017 |
| Enhancement Motives | <.0001 | .0005 | −.0014 | .0008 |
| TOTAL | .0091 | .0027 | .0044 | .0151 |
| Contrast Effects | ||||
| Coping vs. Conformity | ..0035 | .0027 | −.0093 | .0016 |
| Coping vs. Social | .0062 | .0022 | .0118 | .0027 |
| Coping vs. Enhancement | .0063 | .0020 | .0030 | .0112 |
| Conformity vs. Social | .0027 | .0021 | −.008 | .0075 |
| Conformity vs. Enhancement | .0028 | .0018 | −.0001 | .0070 |
Note: Bold font = significant (CIs do not cross zero); BCa = bias corrected and accelerated.
Discussion
The present study contributes to our understanding of the relation of social anxiety with drinking behaviors in several ways. First, data contribute to a large body of work finding that aspects of social anxiety tend to be related to drinking problems (e.g., Buckner, Ecker, & Proctor, 2011; Buckner, et al., 2006; Buckner & Heimberg, 2010; Gilles, et al., 2006; Grant, et al., 2005; Lewis & O'Neill, 2000; Terlecki, Ecker, & Buckner, 2014; Terra et al., 2006). The current study extended this body of research by determining that FPE was strongly related to more drinking-related problems. Notably, FPE was robustly related to drinking problems even after controlling for FNE, sex, typical alcohol consumption, and recruitment site. Second, and consistent with past work finding social anxiety to be unrelated to drinking quantity or frequency (e.g., Bruch, Heimberg, Harvey, & McCann, 1992; Bruch, Rivet, Heimberg, & Levin, 1997; Buckner, et al., 2006; Buckner & Heimberg, 2010; O'Grady, Cullum, Armeli, & Tennan, 2011), FPE was not significantly related to typical alcohol consumption. Third, FPE was related to social, coping, and conformity drinking motives. Taken together, these data suggest that individuals with elevated FPE do not typically drink more often or in greater quantities than their peers with lower FPE; rather, their motives for drinking appear to be associated with greater problems.
Our data regarding drinking motives suggest one possible pathway by which those who fear positive appraisal and social reprisal from dominant others may come to experience problems related to their alcohol use, despite not drinking more. Specifically, our data suggest that these individuals are especially vulnerable to drinking to cope with negative affect, as well as drinking to conform to peers, and that each of these motives accounts significantly for their alcohol-related problems. In following, FPE may be unrelated to quantity or frequency of use if those with elevated FPE only drink when in situations involving negative affect. In fact, socially anxious persons report consuming more alcohol in situations involving negative affect than in other contexts (Terlecki, et al., 2014). A possible future direction would be to ask participants more detailed information regarding the contexts in which they drink for stress reduction (e.g., alone and/or in social situations only, as indicated by conformity motives). Identification of the specific situations in which those with elevated FPE drink to cope and conform will be an important next step in identifying factors that contribute to their experience of more drinking problems. In addition, the current cross-sectional findings are in line with animal research findings (e.g., Duncan et al., 2006; Filatova et al., 2008), such that humans with high FPE may also be more likely to attend and drink in social situations in which most peers are drinking to intoxication (e.g., drinking parties). Social hierarchies may be less pronounced among intoxicated individuals, thereby reducing self-perceptions of subordinate social status (and concomitant negative affect) for those who struggle with social anxiety.
The current findings have several clinical implications. Namely, alcohol use and intoxication may serve as perceived threat-avoidance strategies for some SAD patients. To date, manualized cognitive-behavioral treatments for SAD specifically address FNE and disqualification of positive social outcomes (e.g., Hope, Heimberg, & Turk, 2010), but not FPE. Psychoeducational and exposure-related material concerning FPE is also absent in manualized treatments specially designed for patients with comorbid SAD and substance use disorders (Buckner, 2014). Thus, clinicians may consider explicitly assessing for and targeting FPE when treating patients for SAD (see Weeks & Howell, 2014, for a review) or co-occurring social anxiety and drinking problems. However, this recommendation is tentative—our findings should be replicated in clinical samples to further inform treatment.
The present findings should be considered in light of other limitations, as well. First, the cross-sectional nature of the design limits our ability to test temporal, causal relationships. However, the data do provide, for the first time in the literature, a rationale for future longitudinal work on the relationships among types of fears of evaluation, motives for drinking, and drinking-related problems. Second, the sample was comprised solely of undergraduates, a group that is at particular risk for social anxiety (e.g., Spokas & Heimberg, 2009) and drinking-related impairment (see Ham & Hope, 2003). In addition, our samples were composed mostly of Caucasian females.
Future work could benefit from examining the impact of FPE on drinking behaviors among other populations (with higher proportions of males) to determine the generalizability of the current findings. For example, prior work has found gender to moderate the relationship between social anxiety and alcohol use motives (e.g., Norberg, Norton, Olivier, & Zvolensky, 2010). Future work may extend upon our findings by directly measuring state negative affect and submissiveness in social situations; these constructs play important roles in our current models, but we were unable to test them directly in the current study. Despite these limitations, the current study has identified an important cognitive vulnerability factor related to drinking problems: fear of positive evaluation (FPE). FPE could serve as a critical therapeutic target in interventions designed to decrease problem drinking among socially anxious undergraduates.
Acknowledgements
This work was partially supported by the National Institute of Drug Abuse (NIDA) under Grant [5R21DA029811-02] and under Grant [1R34DA031937-01A1]. NIDA had no further role in study design; in the collection, analysis and interpretation of data; in the writing of the manuscript; or in the decision to submit the manuscript for publication.
Footnotes
Four initially non-normally distributed (skewness or kurtosis ≥ 1.28) measures (i.e., age; DMQ-R: Conformity motives subscale; RAPI; and typical alcohol consumption) were square-root transformed (all transformed skewness and kurtosis values ≤ 0.87) before being included in analyses.
Twenty participants did not report their age in the current sample. No other data was missing.
To explore possible moderating effects of sex on the relationship between FPE and alcohol problems, the interaction term of sex and FPE was also entered into the equation. There was no significant interaction effect, t = 1.00, p = .32, indicating that sex did not moderate the relation between FPE and alcohol problems.
It is worth noting that the pattern of results held when enhancement motives (uncorrelated to FPE) was removed from the mediation model.
References
- American Psychiatric Association . Diagnostic and Statistical Manual of Mental Disorders. 5th ed. American Psychiatric Association; Arlington, VA: 2013. [Google Scholar]
- Blumenthal H, Leen-Feldner EW, Frala JL, Badour CL, Ham LS. Social anxiety and motives for alcohol use among adolescents. Psychology Of Addictive Behaviors. 2010;24(3):529–534. doi: 10.1037/a0019794. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Borsari B, Carey KB. Effects of a brief motivational intervention with college student drinkers. Journal of Consulting and Clinical Psychology. 2000;68(4):728–733. doi: 10.1037/0022-006x.68.4.728. [PubMed] [Google Scholar]
- Bruch MA, Heimberg RG, Harvey C, McCann M. Shyness, alcohol expectancies, and alcohol use: Discovery of a suppressor effect. Journal of Research in Personality. 1992;26(2):137–149. doi: 10.1016/0092-6566(92)90050-e. [Google Scholar]
- Bruch MA, Rivet KM, Heimberg RG, Levin MA. Shyness, alcohol expectancies, and drinking behavior: Replication and extension of a suppressor effect. Personality and Individual Differences. 1997;22(2):193–200. doi: 10.1016/s0191-8869(96)00190-0. [Google Scholar]
- Buckner JD. Dual Diagnosis Cases: Treating Comorbid Social Anxiety Disorder and Substance Abuse or Dependence. In: Weeks JW, editor. Wiley-Blackwell Handbook of Social Anxiety Disorder. John Wiley & Sons, Ltd.; Oxford: 2014. pp. 547–568. [Google Scholar]
- Buckner JD, Ecker AH, Proctor SL. Social anxiety and alcohol problems: The roles of perceived descriptive and injunctive peer norms. Journal of Anxiety Disorders. 2011;25(5):631–638. doi: 10.1016/j.janxdis.2011.02.003. doi: 10.1016/j.janxdis.2011.02.003. [DOI] [PubMed] [Google Scholar]
- Buckner JD, Eggleston AM, Schmidt NB. Social anxiety and problematic alcohol consumption: The mediating role of drinking motives and situations. Behavior Therapy. 2006;37(4):381–391. doi: 10.1016/j.beth.2006.02.007. doi: 10.1016/j.beth.2006.02.007. [DOI] [PubMed] [Google Scholar]
- Buckner JD, Heimberg RG. Drinking behaviors in social situations account for alcohol-related problems among socially anxious individuals. Psychology of Addictive Behaviors. 2010;24(4):640–648. doi: 10.1037/a0020968. doi: 10.1037/a0020968. [DOI] [PubMed] [Google Scholar]
- Buckner JD, Heimberg RG, Ecker AH, Vinci C. A biopsychosocial model of social anxiety and substance use. Depression and Anxiety. 2013;30(3):276–284. doi: 10.1002/da.22032. doi: 10.1002/da.22032. [DOI] [PubMed] [Google Scholar]
- Buckner JD, Schmidt NB, Lang AR, Small JW, Schlauch RC, Lewinsohn PM. Specificity of social anxiety disorder as a risk factor for alcohol and cannabis dependence. Journal of Psychiatric Research. 2008;42(3):230–239. doi: 10.1016/j.jpsychires.2007.01.002. doi: 10.1016/j.jpsychires.2007.01.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Buckner JD, Shah SM. Fitting in and feeling fine: conformity and coping motives differentially mediate the relationship between social anxiety and drinking problems for men and women. Addiction Research and Theory. 2015;23(3):231–237. doi: 10.3109/16066359.2014.978304. doi:10.3109/16066359.2014.978304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Buckner JD, Timpano KR, Zvolensky MJ, Sachs-Ericsson N, Schmidt NB. Implications of comorbid alcohol dependence among individuals with social anxiety disorder. Depression and Anxiety. 2008;25(12):1028–1037. doi: 10.1002/da.20442. doi: 10.1002/da.20442. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Collins RL, Parks GA, Marlatt GA. Social determinants of alcohol consumption: The effects of social interaction and model status on the self-administration of alcohol. Journal of Consulting and Clinical Psychology. 1985;53(2):189–200. doi: 10.1037//0022-006x.53.2.189. doi: 10.1037/0022-006x.53.2.189. [DOI] [PubMed] [Google Scholar]
- Gilles DM, Turk CL, Fresco DM. Social anxiety, alcohol expectancies, and self-efficacy as predictors of heavy drinking in college students. Addictive Behaviors. 2006;31(3):388–398. doi: 10.1016/j.addbeh.2005.05.020. doi: 10.1016/j.addbeh.2005.05.020. [DOI] [PubMed] [Google Scholar]
- Grant BF, Hasin DS, Blanco C, Stinson FS, Chou SP, Goldstein RB, Huang B. The epidemiology of social anxiety disorder in the United States: Results from the National Epidemiologic Survey on Alcohol and Related Conditions. Journal of Clinical Psychiatry. 2005;66(11):1351–1361. doi: 10.4088/jcp.v66n1102. doi: 10.1097/00006199-199507000-00005. [DOI] [PubMed] [Google Scholar]
- Ham LS, Bonin M, Hope DA. The role of drinking motives in social anxiety and alcohol use. Journal of Anxiety Disorders. 2007;21(8):991–1003. doi: 10.1016/j.janxdis.2006.10.014. doi: 10.1016/j.janxdis.2006.10.014. [DOI] [PubMed] [Google Scholar]
- Ham LS, Hope DA. College students and problematic drinking: A review of the literature. Clinical Psychology Review. 2003;23(5):719–759. doi: 10.1016/s0272-7358(03)00071-0. doi: 10.1016/S0272-7358(03)00071-0. [DOI] [PubMed] [Google Scholar]
- Kessler RC, Crum RM, Warner LA, Nelson CB, Schulenberg J, Anthony JC. Lifetime co-occurrence of DSM-III-R alcohol abuse and dependence with other psychiatric disorders in the National Comorbidity Survey. Archives of General Psychiatry. 1997;54(4):313–321. doi: 10.1001/archpsyc.1997.01830160031005. [DOI] [PubMed] [Google Scholar]
- Lewis BA, O'Neill HK. Alcohol expectancies and social deficits relating to problem drinking among college students. Addictive Behaviors. 2000;25(2):295–299. doi: 10.1016/s0306-4603(99)00063-5. doi: 10.1016/s0306-4603(99)00063-5. [DOI] [PubMed] [Google Scholar]
- Lewis MA, Hove MC, Whiteside U, Lee CM, Kirkeby BS, Oster-Aaland L, Larimer ME. Fitting in and feeling fine: Conformity and coping motives as mediators of the relationship between social anxiety and problematic drinking. Psychology of Addictive Behaviors. 2008;22(1):58–67. doi: 10.1037/0893-164X.22.1.58. doi: 10.1037/0893-164X.22.1.58. [DOI] [PubMed] [Google Scholar]
- Morean ME, Corbin WR. Subjective alcohol effects and drinking behavior: The relative influence of early response and acquired tolerance. Addictive Behaviors. 2008;33(10):1306–1313. doi: 10.1016/j.addbeh.2008.06.007. doi: 10.1016/j.addbeh.2008.06.007. [DOI] [PubMed] [Google Scholar]
- Morris EP, Stewart SH, Ham LS. The relationship between social anxiety disorder and alcohol use disorders: A critical review. Clinical Psychology Review. 2005;25(6):734–760. doi: 10.1016/j.cpr.2005.05.004. doi: 10.1016/j.cpr.2005.05.004. [DOI] [PubMed] [Google Scholar]
- Norberg MM, Norton AR, Olivier J, Zvolensky MJ. Social anxiety, reasons for drinking, and college students. Behavior Therapy. 2010;41(4):555–566. doi: 10.1016/j.beth.2010.03.002. doi: 10.1016/j.beth.2010.03.002. [DOI] [PubMed] [Google Scholar]
- O'Grady MA, Cullum J, Armeli S, Tennan H. Putting the relationship between social anxiety and alcohol use into context: A daily diary investigation of drinking in response to embarrassing events. Journal of Social and Clinical Psychology. 2011;30(6):599–615. doi: 10.1521/jscp.2011.30.6.599. doi: 10.1521/jscp.2011.30.6.599. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Preacher KJ, Hayes AF. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behavior Research Methods. 2008;40(3):879–891. doi: 10.3758/brm.40.3.879. doi: doi: 10.3758/BRM.40.3.879. [DOI] [PubMed] [Google Scholar]
- Schneier FR, Foose TE, Hasin DS, Heimberg RG, Liu S-M, Grant BF, Blanco C. Social anxiety disorder and alcohol use disorder comorbidity in the National Epidemiologic Survey on Alcohol and Related Conditions. Psychological Medicine. 2010;40(6):977–988. doi: 10.1017/S0033291709991231. doi: 10.1017/S0033291709991231. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spokas M, Heimberg RG. Overprotective parenting, social anxiety, and external locus of control: Cross-sectional and longitudinal relationships. Cognitive Therapy and Research. 2009;33(6):543–551. doi: 10.1007/s10608-008-9227-5. [Google Scholar]
- Stewart SH, Morris E, Mellings T, Komar J. Relations of social anxiety variables to drinking motives, drinking quantity and frequency, and alcohol-related problems in undergraduates. Journal of Mental Health. 2006;15(6):671–682. doi: 10.1080/09638230600998904. [Google Scholar]
- Terlecki MA, Ecker AH, Buckner JD. College drinking problems and social anxiety: the importance of drinking context. Psychology of Addictive Behaviors. 2014;28:545–552. doi: 10.1037/a0035770. doi: 10.1037/a0035770. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Terra MB, Barros HM, Stein AT, Figueira I, Athayde LD, Spanemberg L, da Silveira DX. Does co-occurring social phobia interfere with alcoholism treatment adherence and relapse? Journal of Substance Abuse Treatment. 2006;31(4):403–409. doi: 10.1016/j.jsat.2006.05.013. doi: 10.1016/j.jsat.2006.05.013. [DOI] [PubMed] [Google Scholar]
- Thomas SE, Randall CL, Carrigan MH. Drinking to cope in socially anxious individuals: A controlled study. Alcoholism: Clinical and Experimental Research. 2003;27(12):1937–1943. doi: 10.1097/01.ALC.0000100942.30743.8C. doi: 10.1097/01.ALC.0000100942.30743.8C. [DOI] [PubMed] [Google Scholar]
- White HR, Labouvie EW. Towards the assessment of adolescent problem drinking. Journal of Studies on Alcohol. 1989;50(1):30–37. doi: 10.15288/jsa.1989.50.30. [DOI] [PubMed] [Google Scholar]
- White HR, Labouvie EW. Towards the assessment of adolescent problem drinking. Journal of Studies on Alcohol and Drugs. 1989;50(1):30–37. doi: 10.15288/jsa.1989.50.30. [DOI] [PubMed] [Google Scholar]