

Introduction
Superior Vena Cava syndrome (SVC) is commonly seen in clinical practice, the most common cause being bronchogenic carcinoma. Here we present an uncommon case of SVC syndrome i.e. dissecting aortic aneurysm.
Case Report
A 48 year old male smoker with no significant past medical history, presented with a two month history of noticing prominent veins over the left side of chest wall, shoulder and left arm. At around the same time he also noticed a dull aching, nagging, continuous pain over the left side of chest, shoulder, arm and neck. The pain was non radiating with no aggravating or relieving factors; it used to subside on taking analgesics. He presented to the casualty when he developed sudden onset of hoarseness of voice. He denied history of cough, haemoptysis, dyspnoea, wheeze or significant weight loss.
General examination revealed an averagely built individual, with a weight of 62 kg. Pulse was 74/min; regular, high volume and collapsing, bilaterally synchronous and all peripheral pulses were felt. BP was 140/40 mm of Hg, Hill's sign was positive. JVP was raised 5 cm above the sternal angle. Prominent veins were seen over the left side of chest, shoulder and arm, the flow was from above downwards (Fig-1). The arm veins remained distended even on raising the hand above the head. There was facial puffiness present and the conjunctiva was suffused. There was grade III clubbing present but no significant lymphadenopathy or dependent edema in any of the limbs.
Fig. 1.
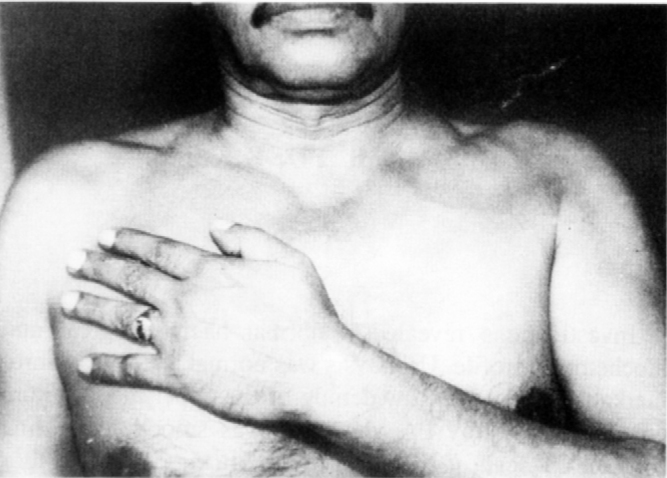
Distended veins and clubbing
Respiratory system examination revealed decreased movements on the left side, Trail's sign positive with trachea shifted to the right, there was fullness of the left supra clavicular region. There was a dull note on percussion over the left infra clavicular region, over the clavicles, supraclavicular region and interscapular area on the left side. Low-pitched bronchial breathing was heard over the same areas. Cardiovascular system examination, revealed an ill localized apex and on auscultation there was an early diastolic murmur heard best in the Erb's area. Palpatation of the abdomen revealed an enlarged liver, 3 cm below the costal margin. There was no neurological deficit.
Investigations revealed a normal haematological and biochemical profile. Urinalysis was normal. ECG was unremarkable. There was a widening of the upper mediastinum on the chest X-ray PA view that was smooth in outline (Fig-2). CT scan of the chest revealed (Fig-3) a large thoracic aortic aneurysm involving the ascending aorta, arch and the proximal part of the descending aorta measuring 68 mm at the aortic arch level, 62 mm at the ascending aorta, 43 mm at aortic root level. There was evidence of dissection containing mural thrombus and measuring 3 mm in thickness involving the left anterolateral aspect of the arch and extending upto 45 mm. Trans-esophageal echocardiography demonstrated a dilated left ventricle with moderate aortic regurgitation (AR). The presence of an aneurysm with a false lumen was confirmed. Color Doppler demonstrated flow in the true and false lumen. HIV and VDRL were non-reactor. The patient was managed with beta-blockers and ACE inhibitors and was subsequently taken up for aortic graft surgery and aortic valve replacement.
Fig. 2.
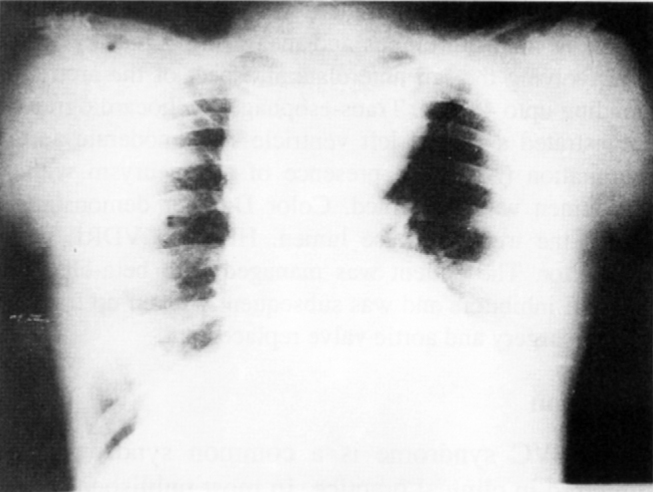
X-ray chest PA view showing widening of mediastinum with smooth outline
Fig. 3.
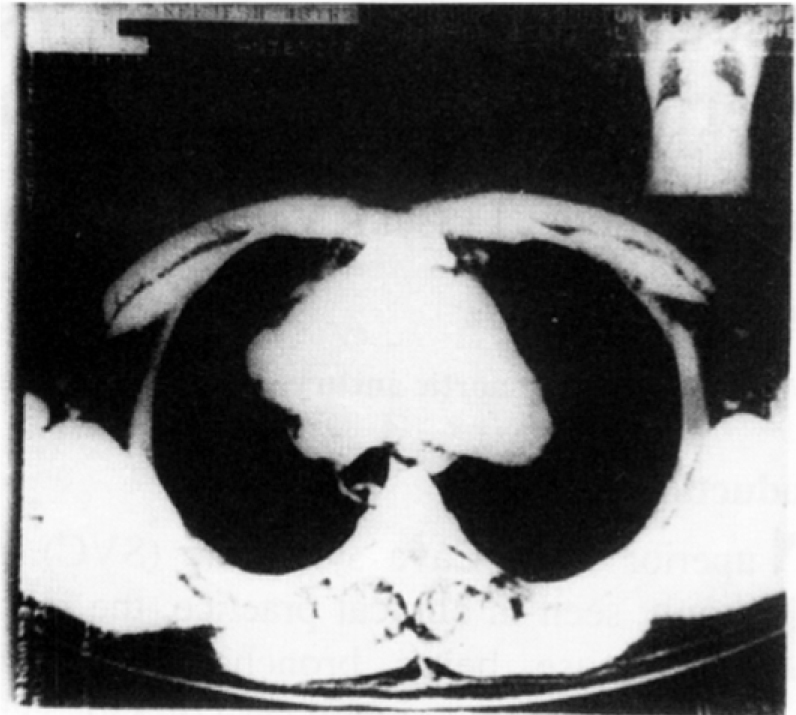
CT scan showing aortic aneurysm with dissection involving the left anterolateral portion
Discussion
The SVC syndrome is a common syndrome encountered in clinical practice. In most published series 95% of the cases are due to underlying malignancy [1]. Among the less known causes is aneurysm of the thoracic aorta. Dissecting aortic aneurysm is an extremely rare cause of SVC syndrome with only a few documented case reports [2].
Aortic dissection is believed to be the commonest cause of potentially fatal aortic disease, an even more common cause of aortic rupture than abdominal aneurysm [3]. Dissecting aortic aneurysm is defined as either a fusiform aneurysm that develops from dilatation of the outer wall of a false lumen or a pre-existing fusiform aneurysm of other origin with superimposed aortic dissection [3]. Dissection can be acute or chronic, the latter lasting for more than 14 days [3]. Our patient had deBakey type I/Stanford type A aortic dissection involving the ascending aorta and the arch. He probably had a pre-existing aneurysm, which dissected and manifested as SVC syndrome. Aortic regurgitation is noted in 50% of aortic dissection involving the ascending aorta.
Fernandez Alonso et al reported a case of painless aortic dissection presenting as SVC syndrome [4]. Our patient had ill defined pain over the chest but it was not the classical pain of acute aortic dissection. Link et al reported a similar case in 1994 [5]. Rosenzweig et al, in their case report, demonstrated the usefulness of trans-esophageal echocardiography (TEE) in a 82 year old woman presenting as SVC syndrome due to dissected aneurysm of the ascending aorta [6]. In our patient too, TEE was used to confirm the findings of CT scan.
This case report emphasizes the rarity of dissecting aortic aneurysm manifesting as SVC syndrome, more so because it mimicked the most common cause of SVC syndrome ie. bronchogenic carcinoma by presenting in a chronic smoker with clubbing and symptoms and signs of mediastinal mass causing pressure effects.
References
- 1.Escalnie CP. Causes and management of Superior Vena Cava Syndrome. Oncology. 1993;7:61. [PubMed] [Google Scholar]
- 2.Fraser RS, Pare PD, Coleman N, Muller NL, editors. Middle Mediastinal masses. Diagnosis of Diseases of Chest 4th ed; Saunders: 1999. p. 2945. [Google Scholar]
- 3.Crawford ES. The diagnosis and management of aortic dissection. JAMA. 1990;264:2537–2541. [PubMed] [Google Scholar]
- 4.Alonso FL, Pelaez FS, Garrido CJ. Superior vena cava syndrome as initial manifestation of acute aortic dissection: a case report and review of literature. An Med Internal. 1997;14(12):633–635. [PubMed] [Google Scholar]
- 5.Link MS, Pietrazak MP. Aortic dissection presenting as a superior vena cava syndrome. Am J Emerg Med. 1994;12:326. doi: 10.1016/0735-6757(94)90150-3. [DOI] [PubMed] [Google Scholar]
- 6.Rosenzweig BP, Kronzon I. Transesophageal echoeardiographic diagnosis of the superior vena cava syndrome resulting from aortic dissection: a multiplane study. J Am Soc Echocardiog. 1994;7(4):414–418. doi: 10.1016/s0894-7317(14)80202-2. [DOI] [PubMed] [Google Scholar]