

Abstract
Fibrous histiocytoma is a benign tumor of mesenchymal origin. The tumor frequently appears in sun exposed areas on skin and orbital tissues. The subcutaneous appearance of this tumor in deep soft tissues is rare. We present here the eighth reported case of subcutaneous benign fibrohistiocytoma in a 27 year old male patient. Histopathology of the tumor comprises fibroblastic and histiocytic cells which mimic dermatofibroma, xanthomas and nodular fasciitis. Special stains like vimentin can only differentiate these tumors.
Keywords: Benign fibrous histiocytoma, Cheek swelling, Painless swelling, Vimentin
Introduction
Benign fibrous histiocytoma (BFH) is a mesenchymal tumor composed of fibroblasts and histiocytes arising in cutaneous and non cutaneous soft tissues [1]. Cutaneous BHF commonly originate in sun exposed areas of skin. Non cutaneous BFH comprises 1 % of all benign FH lesions [2]. Mean age of patients is 55 years with a range from 12 to 71 years. In the oral cavity the most common site is buccal mucosa and appears to originate from the tongue, gums, upper lip and bone [3–5].
The tumor presents varied histocytology; though the composition includes fibroblasts and histiocytes they differentially diagnose with dermatofibroma, xanthoma, granuloma, and nodular sub epidermal fibrosis. These lesions should be well differentiated from the malignant forms which are more aggressive in nature [6].
This article describes a case of subcutaneous benign fibro histiocytoma in relation to right premolar region.
Case Report
A 27 year old male patient presented to the department of oral and maxillofacial surgery, KLR Lenora Institute of Dental Sciences, Rajahmundry with a complaint of swelling in the right lower part of chin which was gradually increasing in size over a period of one year (Fig. 1). The patient did not have any complaint other than the obvious growth disturbing his work; his profession was marketing personnel, and the clients were complaining that he was holding food in his mouth while talking to them.
Fig. 1.

Extra oral profile photograph
On examination, the tumor was oval in shape, well circumscribed and 2 × 2 cm in size. There was no pain associated with the swelling which was firm in consistency with limited mobility. The clinical differential diagnosis included traumatic neuroma in relation to mental nerve, enlarged massetric lymph nodes and enlarged aberrant salivary gland.
The tumor showed no color change in skin intraorally (Fig. 2). The patient did not have any associated symptoms. The radiograph showed no bony involvement. There was no resorption, pathology nor erosion of the bone.
Fig. 2.

Intra oral photograph
Informed written consent from the patient was obtained.
Surgical Technique
Under aseptic precautions local anesthesia with adrenaline, right inferior alveolar nerve block and local infiltration was administered. A vestibular incision was made intraorally extending from midline to right second premolar region. The lesion was exposed by combination of blunt and sharp dissection. During dissection the mental nerve was visualized and protected. Once the lesion was exposed, it was freed from the surrounding tissues and with the help of Allis tissue forceps the mass was gently teased and excised. After surgical exposure the extension of lesion was identified extending into the cheek from the skin opposite to the lower premolar region. Primary closure of the incision was done and pressure pack given (Fig. 3). There was no abnormal hemorrhage and the entire procedure finished uneventfully. The tissue was then sent for histopathological examination (Fig. 4).
Fig. 3.

Surgical photograph
Fig. 4.

Specimen photograph
Histological Examination
Histological analysis of the specimen showed dense fibrous connective tissue stroma haphazardly arranged collagen fiber bundles and spindle shaped fibroblasts like cells arranged in short fascicles (Fig. 5). Fibroblasts were plump with hyper chromatic nuclei. Histiocytes with vesiculated nuclei were seen.
Fig. 5.
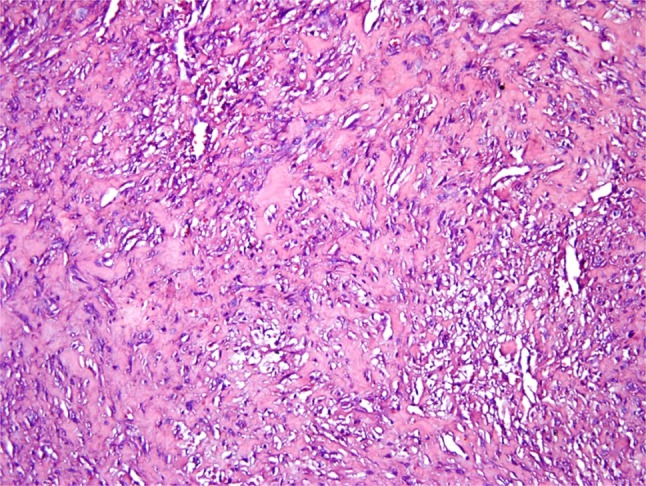
×20 magnification reveals plump, vesiculated spindle shaped fibroblasts along with histiocyte like cells with vesiculated nuclei and areas of hyalinization
Immunohistochemical staining demonstrated a focal positivity for CD34 and stromal cells showing diffuse cytoplasmic positivity for vimentin and negativity for S100 diagnosed as benign fibrous histiocytoma (Fig. 6).
Fig. 6.
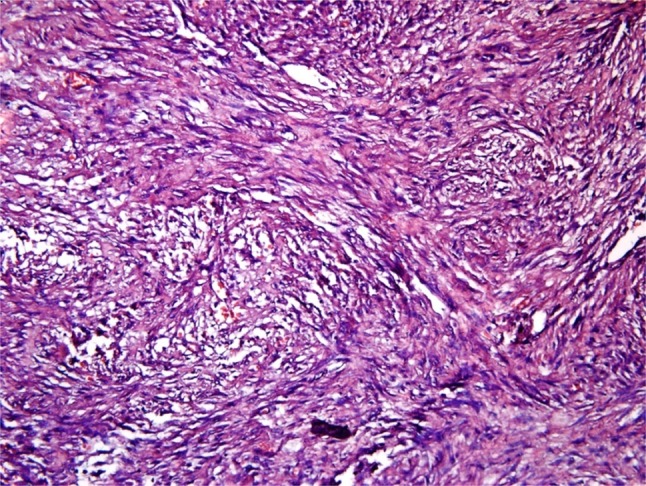
×40 magnification reveals spindle shaped fibroblasts with hyperchromatic nuclei in storiform pattern, histiocyte like cells and endothelial cells
Discussion
Fibrous histiocytomas represent a classical entity for diagnosis. They are mesenchymal in origin. The tumor mimics various other forms of dermatofibromas and aggressive malignant fibrous histiocytoma [3]. The diagnosis relies on immunohistochemistry and electron microscopy.
The tumor most frequently occurs in dermis but is also found in soft tissue and parenchymal organs. The BFH usually originates in sun exposed areas of skin and orbital tissues whereas occurrence of this lesion in deep soft tissue of head and neck has rarely been reported [10]. The search of literature shows only 7 cases of subcutaneous benign fibrohistiocytoma of head and neck region (Table 1) [2].
Table 1.
Review of literature of subcutaneous fibrous histiocytoma
| S. no. | Surgeon | Site | Age/sex | Treatment | Year |
|---|---|---|---|---|---|
| 1 | Fletcher | Subcutaneous face | 45/M | Local excision | 1990 |
| 2 | Fletcher | Subcutaneous scalp | 31/M | Local excision | 1990 |
| 3 | Fletcher | Subcutaneous scalp | 58/F | Local excision | 1990 |
| 4 | Fletcher | Subcutaneous scalp | 10/F | Local excision | 1990 |
| 5 | Fletcher | Subcutaneous cheek | 60/M | Local excision | 1990 |
| 6 | Fletcher | Subcutaneous cheek | 56/M | Local excision | 1990 |
| 7 | C.E. Skoulakis | Subcutaneous cheek | 22/M | Local excision | 2007 |
These tumors usually present between 1 and 70 years [11, 12] with a male to female ratio of 2.5:1 [10]. These tumors develop to a size of 2–12 cm in diameter and the duration of development ranges from 3 to 12 months as reported in literature [6, 7]. Rare intrabony tumors are also reported. The nature of the tumor appears to be both neoplastic and reactive. It was also reported that fibrous histiocytoma reacts to certain insect bites, thorn pricks and trauma.
Sub cutaneous BFH are usually painless mass which are nodular with mild mobility and firm to elastic in consistency. The overlying skin is normal and presents no lymph node involvement. The clinical appearance shows the tumor is soft tissue in origin.
As there are no specific markers for fibrous histiocytoma the diagnosis is usually confirmed by noting the absence of markers for cells of other lineages.
The tumor is very difficult to diagnose clinically; as stated the tumor is fibroblastic and histiocytic in origin. The immunohistochemistry only confirms the diagnosis. The positivity for CD 34 and vimentin indicates fibro histiocytic nature and negativity for S-100 differentiates the lesion from leiyomyosarcoma and neurogenic tumors [7].
The differential diagnosis of BFH includes nodular fasciitis which present as spindle cells arranged in stori form configuration separated by myxoid stroma. Second differential diagnosis is solitary fibrous tumor which is negative for CD34. Another differentiation is neurofibroma which is positive for S-100 [10].
Benign Fibrohistiocytoma tumors should be differentiated from aggressive form—malignant fibrohistiocytoma—which appear in childhood and are characterized by sheets of histiocytes interrupted by cystic areas of hemorrhage surrounded by dense cuff of lymphocytes and plasma cells.
Most lesions are treated by local excision with clear margins. The lesion has no metastatic potential and generally has good prognosis [8]. Fewer than 5 % of cutaneous fibrous histiocytoma recur following local excision and there are no reported cases of recurrence in mouth. Local excision of these lesions show no major functional or cosmetic morbidity [9]. Radiation therapy and chemotherapy have currently no major role in management of benign fibrous histiocytoma [10].
Conclusion
Benign fibrous histiocytoma is a mesenchymal tumor composed of cells with fibroblastic and histiocytic characteristics. The tumor is rare and presents a clinical and histopathological challenge. After two year of follow up the patient did not have any specific problems (Figs. 7, 8). Proper diagnosis and treatment plan with long term follow up is of utmost importance in the management of these tumors.
Fig. 7.

Post operative photograph
Fig. 8.

One year post operative Intra oral photograph
Conflict of interest
None.
Ethical approval
Approved by ethical committee of Lenora Institute of Dental Sciences.
Contributor Information
Damera Srikanth, Email: srivaishnavidamera@gmail.com.
Vaishnavi Devi, Email: vaishnavidevimajeti@gmail.com.
Naveen Polishetty, Email: Dr.naveenpolisetty.omfs@gmail.com.
References
- 1.Chen TC, Kuo T-T, Chan H-L. Dermatofibroma is a clonal proliferative disease. J Cutan Pathol. 2000;27(1):36–39. doi: 10.1034/j.1600-0560.2000.027001036.x. [DOI] [PubMed] [Google Scholar]
- 2.Skoulakis CE, Papadakis CE, Datseris GE, Drivas EI, Kyrmizakis DE, Bizakis JG. Subcutaneous benign fibrous histiocytoma of the cheek. Case report and review of the literature. Acta Otorhinolaryngol Italica. 2007;27(2):90–93. [PMC free article] [PubMed] [Google Scholar]
- 3.Gray PB, Miller AS, Loftus MJ. Benign fibrous histiocytoma of the oral/perioral regions. J Oral Maxillofac Surg. 1992;50:1239. doi: 10.1016/0278-2391(92)90165-V. [DOI] [PubMed] [Google Scholar]
- 4.Hong KH, Kim YK, Park JK. Benign fibrous histiocytoma of the floor of the mouth. Otolaryngol Head Neck Surg. 1999;121:330. doi: 10.1016/S0194-5998(99)70202-0. [DOI] [PubMed] [Google Scholar]
- 5.Sullivan BO, Audel N, Catton CN, Gullane PJ. Soft tissue and bone sarcomas of the head and neck. In: Harrison LB, Sessions RB, Hong WK, editors. Head and neck cancer. 2. Philadelphia, PA: Lippincott Williams & Wilkins; 2004. pp. 786–823. [Google Scholar]
- 6.Fletcher CD, Gustafson P, Rydholm A, Willen H, Akerman M. Clinicopathologic re-evaluation of 100 malignant fibrous histiocytomas: prognostic relevance of subclassification. J Clin Oncol. 2001;19:3045–3050. doi: 10.1200/JCO.2001.19.12.3045. [DOI] [PubMed] [Google Scholar]
- 7.Mentzel T, Kutzner H, Rutten A, Hugel H (2001) Benign fibrous histiocytoma (dermatofibroma) of the face: clinicopathologic and immunohistochemical study of 34 cases associated with an aggressive clinical course. Am J Dermatopathol 23:419–426 [DOI] [PubMed]
- 8.Yamada Hiroyuki, Ishii Hiroaki, Kondoh Toshirou, Seto Kanichi. A case of benign fibrous histiocytoma of the upper lip in a 6-month-old infant. J Oral Maxillofac Surg. 2002;60:451–454. doi: 10.1053/joms.2002.31236. [DOI] [PubMed] [Google Scholar]
- 9.Calonje E, Fletcher CDM. Cutaneous fibrohistiocytic tumors: an update. Adv Anat Pathol. 1994;1:2–15. doi: 10.1097/00125480-199407000-00002. [DOI] [Google Scholar]
- 10.Alves FA, Vargas PA, Coelho Siqueira SA, Coletta RD, De Almeida OP (2003) Benign fibrous histiocytoma of the buccal mucosa: case report with immunohistochemical features. J Oral Maxillofac Surg 61(2):269–271 [DOI] [PubMed]
- 11.Yamada H, Ishii H, Kondoh T, Seto K. A case of benign fibrous histiocytoma of the upper lip in a 6-month-old infant. J Oral Maxillofac Surg. 2002;60:451–454. doi: 10.1053/joms.2002.31236. [DOI] [PubMed] [Google Scholar]
- 12.Sohail D, Kerr R, Simpson RH, Babajews AV. Malignant fibrous histiocytoma of the mandible: the importance of an accurate histopathological diagnosis. Br J Oral Maxillofac Surg. 1995;33(3):166–168. doi: 10.1016/0266-4356(95)90290-2. [DOI] [PubMed] [Google Scholar]