

Abstract
External jugular vein (EJV) is a major superficial vein in the neck which drains deeper parts of face and posterior scalp region. Although it follows a predicted pattern in formation, course and termination in general unusually it also exhibits variations which are clinically important. Gross variations in the incidence of these variations in EJV are noted. We report an anomalous course of EJV which drains into internal jugular vein in our case report. Knowledge about EJV and its origin, course and termination is important for surgeons, interventional radiologist, anaesthesiologist, clinicians in general to avoid inadvertent complication.
Keywords: External jugular vein, Internal jugular vein, Anomaly
Introduction
Major veins draining head and neck are internal jugular vein (IJV) and external jugular vein (EJV). IJV mainly drains cranial cavity and deep structures of the neck, thus constituting the deep venous system. Superficial venous system is EJV which is formed by union of posterior division of retromandibular vein and posterior auricular vein and runs downward over sternocleidomastoid (SCM) muscle, reaches the roof of posterior triangle and pierces the investing layer of deep cervical fascia and drains into ipsilateral subclavian vein [1]. Shima et al. [2] reported 17 % incidence of double EJV where it begins as two veins and joins at the posterior aspect of SCM caudally. Anatomical course of EJV and relationship to the adjacent stable and predictable landmark is important and this knowledge is important in various clinical scenarios. We report our observation of deviation from such predictable course of EJV. We believe that this knowledge of variation can help head and neck surgeon, microvascular surgeon, interventional radiologist, anaesthetist and clinicians can help in successful planning and in avoiding inadvertent complications.
Case Report
A 50 year old patient presented with biopsy proven squamous cell carcinoma of right lateral border of tongue. Clinically patients TNM staging was T4N2bM0-. As per our protocol patient was investigated for routine haematological and general medical examination. Extent of tongue lesion was determined by MRI and ultrasonography of neck for lymph node status. Right sided hemiglossectomy and modified neck dissection (IJV and CN XI sparing) was performed. During neck dissection with Schobinger incision, when the inferior subplatysmal flap was raised, it was observed that EJV which usually runs downward superficially over sternocleidomastoid muscle, but at the level of cricoid cartilage the EJV was found to pierce through investing layer of deep cervical fascia to run into the deeper aspect of neck. After the separation of SCM when the plane around the IJV was established, it was noted that a major vein joined the IJV from lateral direction. As the IJV does not have any posterior or lateral draining vessel, the vein was carefully dissected and after working around the vein, it was found to be EJV draining into IJV (Fig. 1).
Fig. 1.
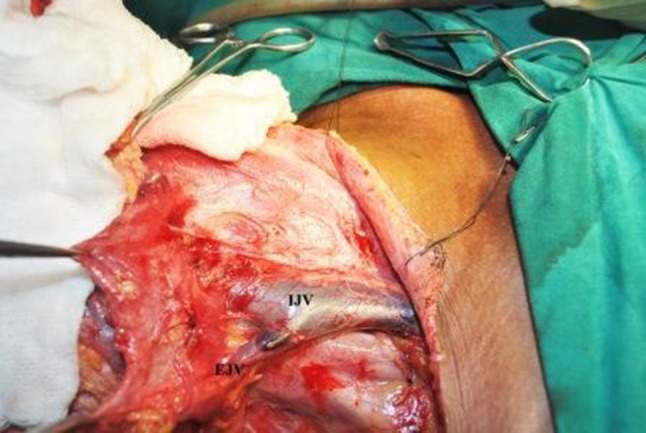
External jugular vein draining internal jugular vein from the lateral aspect right side of neck
Discussion
Variations in venous anatomy are more commonly observed than arterial anatomy. Venous system in the neck shows considerable variation in pattern and dimension and also variation can be either unilateral or bilateral. An anomalous formation of EJV directly from maxillary vein without formation of retromandibular vein and its importance in parotid surgery since it is an important landmark in identifying facial nerve was reported [3]. Duplication of EJV in the middle third of neck on its course down has also been reported [4]. Case reports of absence of EJV [5, 6] and an anomalous communication between EJV and IJV through a communicating vein have been reported [7].
A landmark study by Pikkief [8] describes various patterns of drainage of superficial venous system in the neck. However, even in this study there is no documentation about EJV draining into IJV. Hollinshead mentioned that in one-third of cases EJV drains into IJV. In a human cadaveric study this incidence was 3.33 % [9] and 10 % in yet another study [10]. However literature is sparse on such reports.
Although many variations have been reported in the literature about the EJV draining into IJV, most studies are cadaveric. In our series of 250 neck dissections for managing oral malignancies from 2008 to 2014, we have found this incidence once and hence to be rare and worth documenting. Embryologically this anomaly can be explained by drainage of EJV into portion of cephalic vein which got incorporated into IJV. Upon growth, on elongation of neck this draining area moves upward [10].
Retrospectively, patient’s photographs showed sudden disappearance of dilated EJV at the level of cricoid cartilage. Hence surface anatomy may provide us with a clue about the probable course of underlying vein (Fig. 2).
Fig. 2.

Surface anatomy of external jugular vein. Arrow mark shows disappearance of EJV vascular surface marking at the level of cricoid cartilage
The knowledge of variations in venous patterns in face and neck is of paramount important for head and neck surgeons to avoid unnecessary bleeding during surgical procedures, plan for selecting a suitable IJV/EJV for end to side or end to end anastomosis for free flap tissue transfer. This knowledge of anomaly is also important for catheterisation of EJV for haemodialysis, for the interventional radiologist who performs transjugular procedure, for microvascular surgeon for anastomosis during free flap surgeries.
Acknowledgments
We thank Dr. Niranjan Kumar, Medical Director, SDM College of Medical Sciences and Hospital and Dr. Srinath Thakur, Principle of SDM College of Dental Sciences and Hospital for their constant support and encouragement.
Compliance with Ethical Standards
Conflict of interest
The authors have no financial interest to declare in relation to the content of this article.
Contributor Information
Venkatesh Anehosur, Email: venkyrao12@yahoo.co.in.
Saravanan Rajendiran, Email: dr.saravanan30@gmail.com.
Gautam R. Jayade, Email: gautamjayade83@gmail.com
Niranjan Kumar, Email: drniranjankumar@sdmmedicalcollege.org.
References
- 1.Hollinshead WH. Anatomy for surgeons. 2. Harper: New York; 1956. pp. 530–531. [Google Scholar]
- 2.Shima H, von Luedinghausen M, Ohno K, et al. Anatomy of microvascular anastomosis in the neck. Plast Reconstr Surg. 1998;101:33–41. doi: 10.1097/00006534-199801000-00007. [DOI] [PubMed] [Google Scholar]
- 3.Patil J, Kumar N, Swamy RS, D’Souza MR, Guru A, Nayak SB. Absence of retromandibular vein associated with atypical formation of external jugular vein in the parotid region. Anat Cell Biol. 2014;47(2):135–137. doi: 10.5115/acb.2014.47.2.135. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Comert E, Comert A. External jugular vein duplication. J Craniofac Surg. 2009;20(6):2173–2174. doi: 10.1097/SCS.0b013e3181bf0248. [DOI] [PubMed] [Google Scholar]
- 5.Balachandra N, Padmalatha K, Prakash BS, Ramesh BR. Variation of the veins of the head and neck—external jugular vein and facial vein. Int J Anat. 2012;5:99–101. [Google Scholar]
- 6.Abhinitha P, Rao MKG, Kumar N, Nayak SB, Ravindra SS, Aithal PA. Absence of the external jugular vein and an abnormal drainage pattern in the veins of the neck. OA Anat. 2013;1(2):1–3. [Google Scholar]
- 7.Lalwani R, Rana KK, Das S, Khan RQ. Communication of the external and internal jugular veins: a case report. Int J Morphol. 2006;24(4):721–722. doi: 10.4067/S0717-95022006000500033. [DOI] [Google Scholar]
- 8.Pikkieff E. On the subcutaneous veins of the neck. J Anat. 1937;72(pt 1):119–127. [PMC free article] [PubMed] [Google Scholar]
- 9.Vaida MA, Niculescu V, Motoc A, Bolintineanu S, Sargan I, Niculescu MC. Correlations between anomalies of jugular veins and areas of vascular drainage of head and neck. Rom J Morphol Embryol. 2006;47(3):287–290. [PubMed] [Google Scholar]
- 10.Yadav S, Ghosh SK, Anand C. Variations of superficial veins of head & neck. J Anat Soc India. 2000;49(1):61–62. [Google Scholar]