

Abstract
The appearance of the ear is an important component of the facial characteristics. Lower auricular malformations are less frequent than total or upper auricular malformations. The patients are affected unilaterally in general. Cleft earlobe is frequently encountered among earlobe anomalies. The presented case may be classified as longitudinal type according to Kitayama (Jpn J Plast Reconstr Surg 11:663–670, 1980). Many of the correction methods may lead to patient discomfort due to possible conspicuous scar. The patient was a 5 year old girl. In the presented case, a simple method has been performed. Satisfactory outcome is achieved. As a simple method applying longitudinal division and rotation procedure does not have marginal excision. Furthermore there is no additional incision outside the cleft margin. Local flap and graft are not applied. Conservative approach was maintained with respect to scar occurrence. This method is not favourable in the case of acquired split earlobe deformities due to the wide cleft surface. Postoperative 3rd-month appearance demonstrated adequate correction.
Keywords: Congenital, Cleft, Earlobe, Division
Introduction
The clinical presentations in cleft earlobe malformations show variable deficiencies in the earlobe. Presented case may be classified as longitudinal type according to Kitayama [1].
The primitive ear arises in a 50-day-old embryo. Failure of the fusion between the first and sixth hillocks probably results from congenital cleft earlobe malformation [2]. Congenital cleft earlobe malformations have been divided into various subgroups by different authors [1, 3–5]. Reconstructive demands may increase depending on the malformation severity [6]. In the presented case, a simple method has been performed. Satisfactory outcome is achieved.
Methods
Patient was a 5 year old girl (Fig. 1). Patient and her family complained about the appearance of her left ear. On inspection, the horizontal levels of the ears were equal. Cleft had a gap. A dotted line was placed from the top of the gap to the bottom of the medial component. A marking of the same length was placed in the lateral component (Fig. 2). All margins were marked at the longitudinal axis (Fig. 3A). The operation was performed under general anesthesia. Thumb and index finger of the nondominant hand were used to stabilize the cleft margin. Margin was bisected 3 mm deep longitudinally, and thus the two division surfaces were gained anteriorly and posteriorly (Fig. 3B). Lateral and medial margins were matched and sutured on both surfaces one by one. Postoperative appearance of the ear is shown (Fig. 4). Postoperative 3rd-month appearance demonstrated adequate correction (Fig. 5).
Fig. 1.

A 5 year-old female patient with longitudinal type congenital cleft earlobe
Fig. 2.
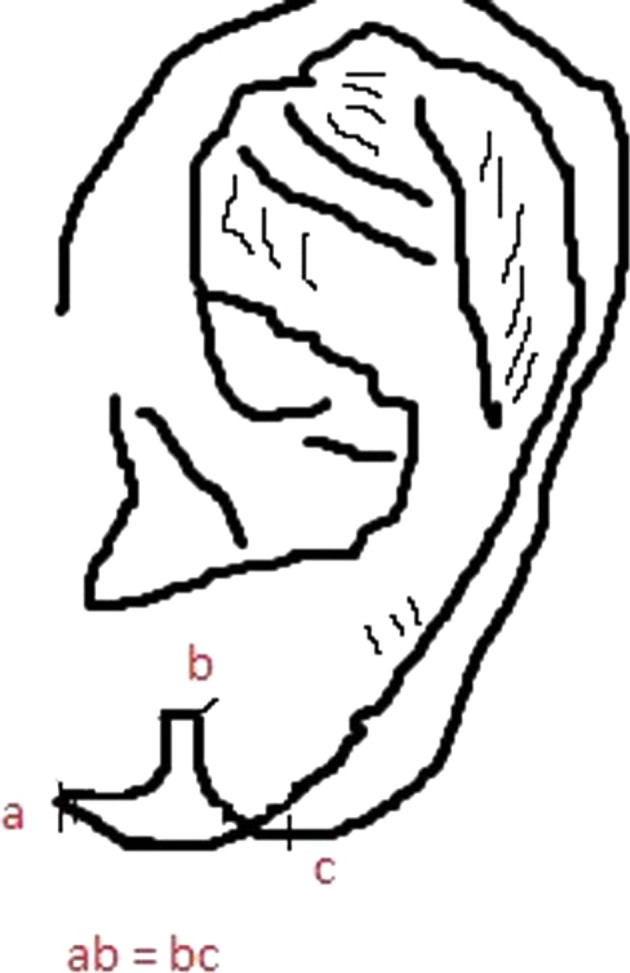
Diagrammatic representation of congenital cleft earlobe, designate of the equal lengths
Fig. 3.

A Margin marked at the longitudinal axis. B Longitudinal incision along margin
Fig. 4.

Postoperative appearance after suturation
Fig. 5.

Appearance 3 month after the operation
Results
Although scar maturation was not completed, patient was evaluated on the postoperative 3rd month. Scar contracture and lobular notching were at an acceptable level.
Discussion
In the method used by Bhandari [7], a flap was prepared from the lateral component to realize the inferior lobule margin, and medial component was advanced into the rotated lateral component. Our patient had a wide cleft, therefore this method was not applied.
The techniques for correction of a cleft earlobe can be listed as simple wedge excision and suture introduction, Z-plasty or W-plasty [8], local flaps [9], Y–V advancement flaps [6], 7-plasty [10], flap plus graft [11] and hinge flap [12]. Many of these techniques may lead to patient discomfort due to possible conspicuous scar. Applying longitudinal division and rotation procedure does not have marginal excision. Furthermore there is no additional incision outside the cleft margin. Local flap and graft are not applied. Conservative approach was maintained with respect to scar occurrence. This method is not favourable in the case of acquired split earlobe deformities due to the wide cleft surface.
Contributor Information
Selman Karaci, Phone: +90 462 341 56 56, Email: selmankaraci@gmail.com.
Rüştü Köse, Email: rustu.kose@erdogan.edu.tr.
References
- 1.Kitayama Y, Yamamoto M, Tsukada S. Classification of congenital cleft earlobe. Jpn J Plast Reconstr Surg. 1980;11:663–670. [Google Scholar]
- 2.Streeter GL. Development of the auricle in the human embryo. Carnegie Contrib Embryol. 1992;14:111. [Google Scholar]
- 3.Park C. Lower auricular malformations: their presentation, correction, and embryologic correlation. Plast Reconstr Surg. 1999;104(1):29–40. doi: 10.1097/00006534-199907000-00005. [DOI] [PubMed] [Google Scholar]
- 4.Kurihara K. Congenital deformities of the external ear. In: Cohen M, editor. Mastery of surgery: mastery of plastic and reconstructive surgery. Boston: Little, Brown and Co; 1994. pp. 776–779. [Google Scholar]
- 5.Yamada A, Fukuda O, Soeda S, et al. The evaluation of cleft earlobe. Jpn J Plast Reconstr Surg. 1967;19:171–175. [Google Scholar]
- 6.Maral T, Tuncali D, Ozgür F, Gürsu KG. A technique for the repair of simple congenital earlobe clefts. Ann Plast Surg. 1996;37(3):326–331. doi: 10.1097/00000637-199609000-00016. [DOI] [PubMed] [Google Scholar]
- 7.Bhandari PS. Congenital cleft earlobe: surgical repair. Plast Reconstr Surg. 2001;108(4):986–987. doi: 10.1097/00006534-200109150-00027. [DOI] [PubMed] [Google Scholar]
- 8.Yotsuyanagi T, Yamashita K, Sawada Y. Reconstruction of congenital and acquired earlobe deformity. Clin Plast Surg. 2002;29(2):249–255. doi: 10.1016/S0094-1298(01)00010-4. [DOI] [PubMed] [Google Scholar]
- 9.Fujiwara T, Matsuo K, Taki K, Noguchi M, Kiyono M. Triangular flap repair of the congenital earlobe cleft. Ann Plast Surg. 1995;34(4):402–405. doi: 10.1097/00000637-199504000-00011. [DOI] [PubMed] [Google Scholar]
- 10.Borman H, Deniz M, Ertas NM, Seyhan T, Caglar B. 7-plasty technique for the surgical treatment of congenital longitudinal ear lobe cleft. J Craniofac Surg. 2008;19(6):1643–1644. doi: 10.1097/SCS.0b013e31818c0306. [DOI] [PubMed] [Google Scholar]
- 11.Hwang K, Kim DH, You SH. Correction of congenital transverse cleft of the earlobe. J Craniofac Surg. 2011;22(1):279–280. doi: 10.1097/SCS.0b013e3181f7b7c5. [DOI] [PubMed] [Google Scholar]
- 12.Qing Y, Cen Y, Xu X, Chen J. A new technique for correction of simple congenital earlobe clefts: diametric hinge flaps method. Ann Plast Surg. 2013;70(6):657–658. doi: 10.1097/SAP.0b013e31824144a7. [DOI] [PubMed] [Google Scholar]