

Abstract
A 74-year-old man presented with right flank pain and a palpable mass in the left flank. Blood pressure was normal. Contrastenhanced computed tomography (CT) showed a 17 × 16 × 12 cm retroperitoneal mass over the left kidney, solid and heterogeneous. There were also 3 retro aortic lymph nodes and bilateral renal lithiasis. Twenty four-hour urinary metanephrines and normetanephrines were normal. The patient underwent a resection of the mass with left adrenalectomy by a lumbar incision. Histological findings revealed an adrenal oncocytic neoplasm (AON) with uncertain malignant potential. Six months after surgery, CT control showed neither local nor distant recurrence.
Keywords: Adrenal gland, Oncocytic neoplasm, Uncertain malignant potential
A 74-year-old man presented with right flank pain and a palpable mass in the left flank. Blood pressure was normal. CT showed a 17 × 16 × 12 cm retroperitoneal mass, over the left kidney, solid, with significant contrast enhancement (Figs. 1 and 2). There were 3 retro aortic lymph nodes and bilateral renal lithiasis, the right kidney was not functional. Serum potassium and daily urinary metanephrines and normetanephrines were normal. The patient underwent a resection of the mass by a lumbar incision. Histological findings revealed an adrenal oncocytic neoplasm(AON) with uncertain malignant potential (Fig. 3). Six months after surgery, CT control showed neither local nor distant recurrence.
Figure 1.

Contrast computed tomography showing a voluminous and heterogeneous supra-renal left mass.
Figure 2.
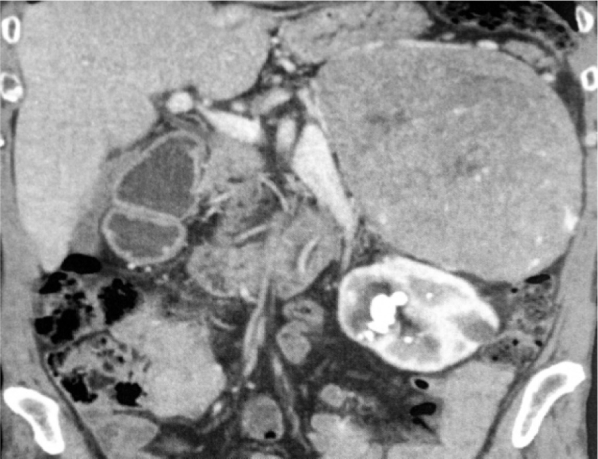
Contrast computed tomography showing a voluminous and heterogeneous supra-renal left mass.
Figure 3.
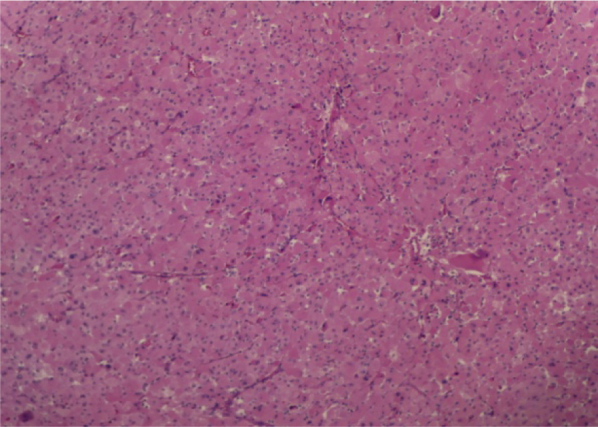
The tumor cells have an oncocytic appearance with abundant eosinophilic, granular cytoplasm and nuclear pleomorphism.
AON are extremely rare, tumors with uncertain malignant potential are rarer.1 They are usually detected in female at the fourth decade.2 Most of these tumors are non-functioning.3 Imaging findings are generally non specific.4 Adrenalectomy is the standard of treatment. Laparoscopy can be performed when there is no evidence of invasion into surrounding tissue and no adenopathy.5 The average diameter is 8 cm. Microscopic examination shows eosinophilic and granular cells arranged in trabecular, tubular or papillary patterns.6 According to Weiss criteria, AONs may be in 3 histological categories. Prognosis depends on these criteria. For tumors with uncertain malignant potential, only evolution may determinate it.
Conflict of interest
There is no conflict of interest.
References
- 1.Mearini L., Del Sordo R., Costantini E. Adrenal oncocytic neoplasm: a systematic review. Urol Int. 2013;91:125–133. doi: 10.1159/000345141. [DOI] [PubMed] [Google Scholar]
- 2.Lin B.T., Bonsib S.M., Mierau G.W. Oncocytic adrenocortical neoplasms. A report of seven cases and review of the literature. Am J Surg Pathol. 1998;22:603–614. doi: 10.1097/00000478-199805000-00012. [DOI] [PubMed] [Google Scholar]
- 3.Wong D.D., Spagnolo D.V., Bisceglia M. Oncocytic adrenocortical neoplasms – A clinicopathologic study of 13 new cases emphasizing the importance of their recognition. Hum Pathol. 2011;42:489–499. doi: 10.1016/j.humpath.2010.08.010. [DOI] [PubMed] [Google Scholar]
- 4.Shah R.K., Oto A., Ozkan O.S. Adrenal oncocytoma: US and CT findings. JBR-BTR. 2004;87:180–182. [PubMed] [Google Scholar]
- 5.Rosenkrantz A.B., Do R.K., Hajdu C.H. Imaging appearance of bulk fat within an oncocytic adrenocortical neoplasm, a rare and potentially malignant tumour. Br J Radiol. 2010;83:204–207. doi: 10.1259/bjr/50022555. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Schittenhelm J., Ebner F.H., Harter P., Bornemann A. Symptomatic intraspinal oncocytic adrenocortical adenoma. Endocr Pathol. 2009;20:73–77. doi: 10.1007/s12022-008-9051-1. [DOI] [PubMed] [Google Scholar]