

Abstract
Background:
Hypertension is increasing rapidly in developing countries. Today, modern technologies are suggested as the tools used to enhance medication adherence. This study aimed to compare the effectiveness of short message service (SMS) to reminder cards with regard to medication adherence in patients with hypertension.
Methods:
The present study is a randomized controlled clinical trial. The subjects consisted of 123 patients with hypertension at the clinical-educational center of Sayyed-Al Shohada, Urmia, who met the study criteria. Selected based on the convenience method, the samples were randomly divided into three groups: the SMS group, the reminder-cards group, and the control group. The subjects in the SMS group were sent 6 text messages a week for three months, and the subjects in the reminder-cards group were trained in how and in what order to use their cards. Hill-Bone medication adherence scale was completed by all the participants before and three months after the intervention. Data analysis was performed in SPSS software, using one-way ANOVA.
Hill-Bone medication adherence scale was completed by all the participants before and three months after the intervention. Data analysis was performed in SPSS software, using one-way ANOVA.
Results:
The results of ANOVA test demonstrated that the mean scores of medication adherence were statistically different among the three groups of control (46.63±2.99), SMS (57.70±2.75) and the reminder cards (57.51±2.69) after the intervention (P<0.001). However, after the intervention the means of the patients’ medication adherence scores were not statistically different between the two groups trained via SMS and reminder cards (P>0.05).
Conclusion:
The findings of the present research demonstrated that training and distance-monitoring via SMS and reminder cards promote medication adherence of patients. Therefore, healthcare teams and nurses are recommended to apply such training methods.
Trial Registration Number: IRCT2015110917059N2
KEYWORDS: Hypertension, Medication adherence, Reminder system, Short message service
INTRODUCTION
A global medical challenge, hypertension can cause a variety of disorders in one’s organs, especially the heart.1 Despite the many advances in the treatment of hypertension, there are still many unanswered questions in the pathology of the disorder; in 90 to 95 percent of patients, the cause of hypertension cannot be diagnozed.2 Hypertension is a prevalent disorder worldwide, with approximately 73 million American adults suffering from the disease.3 According to the latest statistics of world health organization (WHO), hypertension has affected more than one-third of the world’s population over 25 years.4 Likewise, in Iran many studies report the incidence of hyertension to be high; in 2006, Delavari et al. reported that 25.31 and 26.05 percent of men and woemn in Iran suffer from hypertensin, respectively.5 In a national research in 2004, the incidence of hypertension in urban and rural areas was found to be 30.5 and 29.2 percent, respectively.6
Heart diseases are the the leading cause of death in patients with hypertension.7 It is estimated that by 2030, 23 million people wil have lost their lives due to hypertension-related cardiovascular diseases.4 The incidence of brain stroke caused by high blood presure (especially in people over 65) is rapidly increasing.7 Moreover, prolonged hypertension can, by damaging the renal veins, cause kidney failure and, if left untreated, lead to death.8
By medication adherence, patients can avoid the serious consequences of hypertension. Medication adherence will not only prevent the occurrence of subsequent problems, but can control and treat the disease in its early stages. On the other hand, failure to adhere to one’s medication is one of the most serious barriers to achieving the positive results of treatment plans.9 Medication adherence can be defined as following the dietary and medicine instructions or the lifestyle recommended by the providers of clinical care.10 In the case of patients with hypertension, adherence includes sticking to the recommended diet, exercising, medication, and monitoring ad recording one’s blood pressure.11
On average, 65 to 75 percent of patients follow the diets recommended by their care providers; however, only 45 to 55 percent of those with chronic diseases such as hypertension included adhered to their diets.9 In developing countries, medication adherence has been found to be even less (50 percent), and only 30 to 50 percent of patients with hypertension have been reported to observe their treatment plans.10 Poor medication adherence prevents the patients from achieving the goals of their treatment plans and, ultimately, form recovery. An incomplete recovery process, in turn, results in frequent visits to medical centers, reduction in the quality of life of patients, and an increase in medical costs.11
Even though considerable amounts of time and energy are spent for diagnostic measures, most patients ignore or only partially follow the medical diets they are instructed to follow.2 Among the factors that affect the patients’ adherence are demographic characteristics, severity of disease, complexity of drug regimen (number of drugs and daily doses prescribed), drug classes (due to tolerability and side effects to medication), patients’ forgetfulness and lack of understanding about the nature of the disease.12 In another retrospective cohort study on variance in adherence among hypertensive patients, it was found that the factors that had the strongest positive effect on adherence included duration of hypertension (better adherence in patients with shorter duration) and the use of newer agents.13 In view of the direct consequences of hypertension and patients’ poor medication adherence, it is necessary to educate the patients on the nature of hypertension, the urgency of seeking medical care, and the importance of adherence to the recommended medication.14 A wide range of different strategies and interventions have been used to support the patients in adherence to treatment plans, although the results are not consistent.15 Reducing the number of daily doses appears to be effective in increasing adherence to blood pressure treatment plans.16 Methods of encouraging patients to stick to the administration of the drugs prescribedinclude: motivational interview, family support, daily- or weekly-graded reminder boxes, recording one’s own blood pressure, and simplification of the patients’ medical regimens.10
Today, such new technologies as text messaging are suggested as ways to enhance medication adherence. To increase the patiens’ adherence to their treatement plans, text messages can be sent daily or weekly to maintain a one-sided or interactive (asking and answering questions) relationship with patients and remind them to take their medication.17 Text messaging, one of the simplest and most popular functions of mobile phones, can provide the patients with access to the information they need at any time and place; moreover, compared to other forms of information thechnology, e.g. the Internet, mobile phones are easier to use.18 Two trials in Spain with short follow-up periods have explored the efficacy of SMS-based interventions for people with hypertension to improve treatment compliance and blood pressure control. Although the trials’ results suggest the potential for small to moderate effect sizes in improved compliance and blood pressure control, the effects were not statistically significant.15 However, despite the many advantages of text messaging, errors are also inevitable; messages may not be received due to technical failure, a patient’s cell-phone may be off, or a message may be ignored.18
Another method for monitoring the patients after discharge is using reminder systems: tools which patients are provided with at discharge. There are various forms of reminder systems, such as electronic systems and reminder cards.19 Reminder cards are simple educational tools which are easy to use and very common. The cards can result in greater attention to treatment-related hygenic and clinical matters and effectively remind the patients of their instructions; however, since reminder cards are more costly than sending text messages in patient education, they are approached with caution.20 By encouraging self-care and medication adherence, reminder packages can improve the treatment process.21 However, this system has its own shortcomings, such as the patients’ forgetting about the educational package, failure to use it at the right time, using the reminder cards all at once and disregarding them during the rest of one’s treatment.19 Long-term blood pressure control requires integrating the medication into daily life to support adherence and persistance on treatment.15 Therfore, the present study aimed to compare the effectiveness of text messaging with that of reminder cards in medication adherence in the case of patients with hypertension referring to the clinical-educational center of Sayyed-Al Shohada, Urmia, in 2013.
MATERIALS AND METHODS
This is a randomized controlled clinical trial study with a pretest-posttest design, conducted at the governmental clinical-educational center of Sayyed-Al Shohada, affiliated with Urmia University of Medical Sciences. The data were collected from April to October 2013. The inclusion criteria for this study were: age between 20-60 years, literacy, expert confirmation of uncontrolled hypertension, being on medication for hypertension, living in the city of Urmia, having access to a mobile phone, being able to use the text messaging function (reading and composing a text message), not being on medication for prostate in the male patients, and willingness to participate in the study. The exclusion criteria were: being hospitalized in the duration of the study, unwillingness to participate further, moving to another city, being permanently treated for hypertension, and loss of contact with the patient through his/her mobile phone.
Sample size was calculated using power sample size calculator (SSC) software and the results of a previous study conducted by Strandbygaard et al. in which μ1, and μ2 were respectively equal to 86.6, 60.8.22 Then, with a type I error of 0.05 and a power of 0.80, the sample size was estimated to be 41 patients for each group. In total, 123 patients participated in the study. Sampling was based on the convenience method. In this study allocation concealment was observed, and the patients were randomly divided into three groups: each patient was asked to choose a card from a pack of cards of three different colors green, red and yellow; those with a green card were assigned to the text messaging group, the red cards were assigned to the control group and the yellow cards were assigned to the reminder cards group. The patients had not been informed of the significance of colors and the researchers until the allocation of patients to three groups they did not know which patient will be in which group (figure 1).
Figure 1.
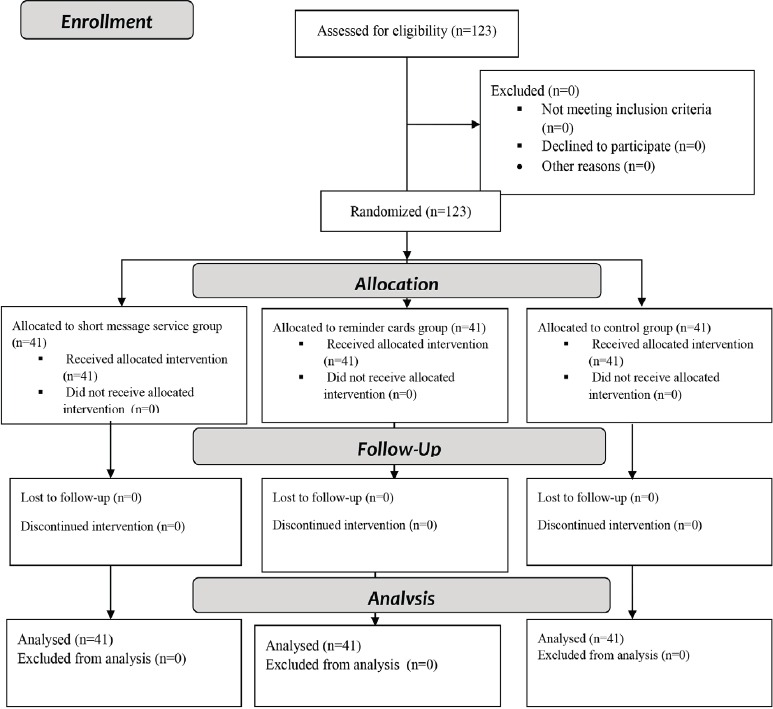
Design and protocol of the study
The study was approved by the research deputy and the research ethics committee of Urmia University of Medical Sciences with the code number of 1525. To begin the study, the researcher explained the objectives to the patients and all the participants signed a written informed consent before participation in the study. The questionnaires were anonymous and all of the participants were assured about the confidentiality of their personal information. The participants were free to withdraw from the study at any time. The researchers observed all ethical issues in accordance with the latest version of Helsinki ethical declaration.
The data collection instrument used by the researchers was the Hill-Bone Compliance to High Blood Pressure Therapy Scale, as developed by Kim et al. in 2000.23 The questionnaire consists of 14 questions which fall into three categories: medication adherence, treatment regimen adherence, and medical appointments adherence. Each item was a four-point Likert scale: never (1), occasionally (2), often (3), and always (4); the maximum and minimum possible scores were, respectively, 56 and 14.
This scale has been validated in many investigations, among which in a South African primary health care setting. Lambert et al. have verified the criterion validity and internal consistency of the Hill-Bone Scale; their results were compared favorably with those from an urban African-American setting (Standardized Cronbach’s alpha was 0.74–0.84).24 In their study, Taher et al. confirmed the validity of the scale based on the content validity approach and under the supervision of 12 faculty members at Shahid Beheshti School of Nursing; moreover, the reliability of the scale was confirmed by calculating the Chronbach’s alpha coefficient of the scores of 20 patients with hypertension; the alpha was found to be 0.8.25 Likewise, the reliability of the Hill-Bonescale has been verified by Ashktorab et al., who found the Cronbach’s alpha of the scale to be 0.71.26 In the present study, the content validity of the scale was verified by 10 nursing faculty members and 5 cardiovascular specialists, and the reliability of the instrument was calculated to be 0.81, 0.84, 0.79, 0.91 respectively for total adherence to treatment, medication adherence, treatment regimen adherence, and medical appointments adherence based on the value of the Cronbach’s alpha.
All the questionnaires were filled out through individual interviews in a private room at the clinical-educational center of Sayyed-Al Shohada. A trained interviewer who was blind to the patients’ groups conducted all the interviews. After completing the questionnaires, 123 patients were randomly assigned into three groups including control, short messaging and reminder cards groups by block randomization.
Intervention for the reminder cards group consisted of education in the appropriate usage and ordering of the cards. The patients in the text messaging group were sent 6 messages a week. Both groups were presented with the same educational content, which fell into four domains: medication adherence, treatment regimen, physical activities, and blood pressure monitoring. The patients in the control group received the standard education of the clinical center. The intervention lasted for 3 months. The patients were expected to inform the researchers if they failed to check their blood pressure or had to visit the clinical center again in the duration of the intervention. Also, all the patients were asked to visit the clinical center on alternate weeks (6 times in total during the 3-month intervention) and have their blood pressure checked for free. The patients in the text messaging group could text the researchers if they had any questions about the educational messages they were sent. At the end of the intervention, the patients were asked to visit the clinical center and complete the compliance scale again.
Statistical analyses were conducted using SPSS software (Version 20; SPSS Inc, Chicago, IL). The normality of data was determined using the Kolmogorov–Smirnov test, as well as skewness and kurtosis values. All the tests conducted were two-tailed. The alpha level of significance for all inferential statistics was set at 0.05. Differences in adherence scores between the groups were tested using ANOVA.
RESULTS
The ANOVA and Chi-square test results showed that the qualitative variables of gender, marital status, occupation, education, income, hypertension familial history and smoking and the quantitative variables of age and body mass index (BMI) among the three groups were not significantly different (table 1).
Table 1.
Comparison of demographic characteristics in three groups
| Variable | Category | Control group | Text messaging group | Reminder Cards group | Chi-square test result |
|---|---|---|---|---|---|
| N (%) | N (%) | N (%) | |||
| Gender | Woman | 29 (70.7) | 27 (65.9) | 31 (75.6) | X2=0.943 df.=2 P=0.624 |
| Man | 12 (29.3) | 14 (34.1) | 10 (24.4) | ||
| Marital Status | Single | 1 (2.4) | 1 (2.4) | 0 (0) | X2=1.469 df.=4 P=0.832 |
| Married | 38 (92.7) | 38 (92.7) | 40 (97.6) | ||
| Divorced | 2 (4.9) | 2 (4.9) | 1 (2.4) | ||
| Occupation | Unemployed | 2 (4.9) | 1 (2.4) | 0 (0) | X2=6.052 df.=6 P=0.417 |
| Employee | 5 (12.2) | 9 (22.0) | 3 (7.3) | ||
| Housewife | 27 (65.9) | 24 (58.5) | 30 (73.2) | ||
| Retired | 7 (17.1) | 7 (17.1) | 8 (19.5) | ||
| Education Level | Primary | 23 (56.1) | 20 (48.8) | 20 (48.8) | X2=6.607 df.=6 P=0.339 |
| Secondary school | 6 (14.6) | 11 (26.8) | 9 (22.0) | ||
| High school | 9 (22.0) | 4 (9.8) | 10 (24.4) | ||
| College graduate | 3 (7.3) | 2 (4.9) | 6 (14.6) | ||
| Income | Adequate | 17 (41.5) | 29 (70.7) | 22 (53.7) | X2=7.177 df.=4 P=0.127 |
| Somewhat sufficient | 20 (48.8) | 10 (24.4) | 16 (39.0) | ||
| Insufficient | 4 (9.8) | 2 (4.9) | 3 (7.3) | ||
| Smoking | Yes | 4 (14.3) | 14 (50) | 10 (35.7) | X2=8.755 df=4 P=0.068 |
| No | 35 (38) | 26 (28.3) | 31 (33.7) | ||
| Former smokers | 2 (66.7) | 1 (33.3) | 0 (0) | ||
| Variable | Mean±SD | Mean±SD | Mean±SD | ANOVA test result | |
| Age (year) | 50.54±8.14 | 53.68±6.94 | 50.29±10.51 | P=0.307 | |
| BMI | 27.64±3.61 | 28.79±6.22 | 27.33±2.96 | P=0.146 | |
Before the intervention, the mean adherence to treatment and its dimensions (adherence to diet, drug regimen and follow-up medical appointments) scores in the three groups of control, text messaging and reminder cards had no statistically significant differences (P>0.05). However, the mean scores of adherence to treatment and its dimensions (adherence to diet, drug regimen, and follow-up medical appointments) after the intervention increased in the text messaging and reminder cards groups, compared to the control group. Individual one-way ANOVA tests for the three groups showed statistically significant differences between the mean scores of adherence to treatment and its dimensions among the three groups after the intervention (P<0.001) (table 2).
Table 2.
Comparison of the mean scores of adherence to treatment and its dimensions among the three groups before and after the intervention
| Time | Variables | Control group | Massage Service group | Remainder Cards group | ANOVA test result |
|---|---|---|---|---|---|
| Mean±SD | Mean±SD | Mean±SD | |||
| Before the intervention | Follow the diet | 10.19±1.18 | 10.58±1.11 | 10.24±1.79 | P=0.382 |
| Tracking drug regimen | 31.58±2.40 | 30.56±3.39 | 31.41±2.45 | P=0.209 | |
| Follow-up medical appointment | 28.78±2.31 | 32.17±1.20 | 32.09±0.94 | P=0.723 | |
| Adherence to treatment | 52.78±3.65 | 51.46±5.08 | 52.75±5.27 | P=0.264 | |
| After the intervention | Follow the diet | 10.04±1.11 | 11.65±0.52 | 11.46±1.00 | P<0.001 |
| Tracking drug regimen | 5.53±0.86 | 5.60±1.04 | 5.68±0.98 | P<0.001 | |
| Follow-up medical appointment | 5.48±0.86 | 6.73±0.89 | 6.65±0.76 | P<0.001 | |
| Adherence to treatment | 46.63±2.99 | 57.70±2.75 | 57.51±2.69 | P<0.001 | |
Tukey’s post-hoc test showed that after the intervention, the mean score of adherence to treatment for patients in the control group (46.63±2.99), compared with the two groups of text messaging (57.70±2.75) and reminder cards (57.51±2.69), showed a statistically significant difference (P<0.001). But the mean score of adherence to treatment for the patients in the two intervention groups did not show a statistically significant difference (P=0.667).
DISCUSSION
The results of the study showed that the three groups were not significantly different in terms of their demographic profiles: gender, marital status, occupation, educational level, income, age and BMI. Therefore, the statistically significant differences in the dependent variables between the control, text messaging, and reminder cards groups can be attributed to the effectiveness of the interventions in those groups. The results of the present study show that the adherence to treatment mean scores before the intervention in the three groups of control, text messaging, and reminder cards were not significantly different; in other words, all the three groups were homogeneous in adherence to treatment.
Moreover, the results showed that the mean of the three groups’ treatment adherence scores in the three areas of adherence to diet, drug regimen, and follow-up of medical appointments increased significantly, which proves the effectiveness of distance learning through the methods of text messaging and reminder cards. Da Costa et al. reported significant differences in adherence between patients with hypertension who used a reminder alarm card that produced a beep at predetermined times, and patients who did not.19 Andrade et al. found that an electronic reminder device with audiovisual reminders significantly improved adherence in memory-impaired patients (assessed with neuropsychological tests), but not in memory-intact patients.27 On other hand, four studies, which measured the impact of the reminder on multiple time points, showed no effects on adherence at any time point.28-31 Also, Hou et al.’s study revealing no effect used standardized messages without requesting a reply.28
Moreover, the results showed that the increase in treatment adherence did not differ significantly between the two intervention groups; this can mean that the two approaches used in the present study were equally effective in encouraging treatment adherence. Education plays an important role in enhancing treatment adherence.32 The study of Beune et al. confirms the positive impact of education on treatment adherence in patients with hypertension.33
The findings of a study showed an increase in the mean scores of the intervention groups in the area of treatment regimen adherence, and a decrease of the same score in the control group, which proves the efficacy of the educational methods used. In his study, Thomas rated the adherence of patients with heart failure to their regimens as good;34 however, Albert reports that regimen adherence in patients with a chronic cardiovascular disease ranges between average and satisfactory.35 Educating patients in food regimens, exercising and a healthy lifestyle can reduce the risk factors and the consequences of cardiovascular diseases.36
The statistical results of the study demonstrated an increase in the patients’ drug regimen adherence as a result of the researchers’ education. On the other hand, in the case of the control group, who did not undergo any interventions, the results showed a decline in the patients’ adherence to their drug regimen. The results also revealed that text messaging was a more effective way to enhance the patients’ drug regimen adherence: it can be concluded that the daily-sent text messages had acted like an alarm, reminding the patients of the time to take their medicine. Quoting Ingersoll and Cohen, a review study of 76 works of research showed that treatment adherence in patients with a chronic disease increased significantly after the intervention.37
The results of the study also indicated that, after the intervention, the intervention groups had higher scores for adherence to medical appointments than did the control group. According to the statistical results, text messaging has been a more effective way to enhance the patients’ adherence to their medical appointments and periodic visits for monitoring their diseases and medication regimens. In his study entitled “Improving medication adherence in patients with a chronic cardiovascular disease”, Albert concludes that patients’ adherence to their treatment plans increases after education; this conclusion is in the same line with the results of the present study.35 Alongside the effective educational methods employed in the study, the nurses’ regular follow-up inquiries should also be considered as a factor contributing to treatment adherence. Their other advantage is that they can be employed without need for a large staff; it is even possible to use a mass texting service to send out thousands of educational messages daily.
This study was conducted on a small number of patients. Moreover, the duration of follow-up and the interval between the intervention and outcome assessment were short in this study. Then replication of the same study with larger sample size and longer follow-up and longer interval between the intervention and outcome assessment is suggested. Secondary outcome, on the other hand, the blood pressure of patients, in this study was not reported that is the limitation of this study.
CONCLUSION
According to the findings of the present study, text messaging and reminder cards can encourage the patients to adhere to their treatment plans. Nowadays, due to the increasing prevalence of hypertension and its serious consequences, as well as the difficulty of making regular visits to medical centers for patients with chronic diseases to be educated and monitored, the methods of text messaging and reminder cards are suggested as helpful and effective approaches. The low cost of text messaging and reminder cards prompt us to recommend these two options. It is suggested that similar studies be done on patients with other chronic diseases.
ACKNOWLEDGMENT
The present article was extracted from the thesis written by Mahsa Safaie and financially supported by Urmia University of Medical Sciences, grants No. 912. Hereby, the authors appreciate and thank the cooperation of the deputy of Urmia University of Medical Sciences, all the patients who helped us sincerely in doing this research and the nurses of Al Shohada clinical-educational center.
Conflict of Interest: None declared.
REFERENCES
- 1.Thawornchaisit P, De Looze F, Reid CM, et al. Validity of self-reported hypertension: findings from the cohort study compared to physician telephone interview. Global Journal of Health Science. 2014;6:1–11. doi: 10.5539/gjhs.v6n2p1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Wang IK, Tsai IJ, Chen PC, et al. Hypertensive disorders in pregnancy and subsequent diabetes mellitus: a retrospective cohort study. Am J Med. 2012;125:251–7. doi: 10.1016/j.amjmed.2011.07.040. [DOI] [PubMed] [Google Scholar]
- 3.Fauci AS, Braunwald E, Kasper DL, et al. Harrisons Principles of Internal Medicine. 17th ed. US: McGraw-Hill Professional; 2008. [Google Scholar]
- 4.Shrivastava SR, Shrivastava PS, Ramasamy J. The determinants and scope of public health interventions to tackle the global problem of hypertension. International Journal of Preventive Medicine. 2014;5:807–12. [PMC free article] [PubMed] [Google Scholar]
- 5.Delavari A, Horri N, Alikhani S, et al. Hypertension & prehypertension: prevalence, awareness, cure and control in adult above 20-year. Journal of Medical Council of Iran. 2006;24:372–80. [In Persian] [Google Scholar]
- 6.Delavari A, Horri N, Alikhani S, et al. Prevalence of hypertension in Iranian urban and rural populations aged over 20 years in 2004. J Mazandaran Univ Med Sci. 2007;17:79–86. [In Persian] [Google Scholar]
- 7.Benjamin I, Griggs RC, Wing EJ. Andreoli and Carpenter’s Cecil Essentials of Medicine. 8th ed. US: Saunders; 2010. [Google Scholar]
- 8.Muxfeldt ES, de Souza F, Margallo VS, Salles GF. Cardiovascular and renal complications in patients with resistant hypertension. Current Hypertension Reports. 2014;16:471. doi: 10.1007/s11906-014-0471-7. [DOI] [PubMed] [Google Scholar]
- 9.Roberts AW, Crisp GD, Esserman DA, et al. Patterns of medication adherence and health care utilization among patients with chronic disease who were enrolled in a pharmacy assistance program. North Carolina Medical Journal. 2014;75:310–8. doi: 10.18043/ncm.75.5.310. [DOI] [PubMed] [Google Scholar]
- 10.Leiva A, Fajo M, Escriche L, et al. Efficacy of a brief multifactorial adherence-based intervention on reducing the blood pressure of patients with poor adherence: protocol for a randomized clinical trial. BMC Cardiovascular Disorders. 2010;10:44. doi: 10.1186/1471-2261-10-44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Vervloet M, van Dijk L, Santen-Reestman J, et al. Improving medication adherence in diabetes type 2 patients through Real Time Medication Monitoring: a randomized controlled trial to evaluate the effect of monitoring patients’medication use combined with short message service (SMS) reminders. BMC Health Services Research. 2011;11:5. doi: 10.1186/1472-6963-11-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Ambrosioni E, Leonetti G, Pessina AC, et al. Patterns of hypertension management in Italy: results of a pharmacoepidemiological survey on antihypertensive therapy. Scientific Committee of the Italian Pharmacoepidemiological Survey on Antihypertensive Therapy. J Hypertens. 2000;18:1691–9. doi: 10.1097/00004872-200018110-00023. [DOI] [PubMed] [Google Scholar]
- 13.Ramli A, Ahmad NS, Paraidathathu T. Medication adherence among hypertensive patients of primary health clinics in Malaysia. Patient Preference and Adherence. 2012;6:613–22. doi: 10.2147/PPA.S34704. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Pollock SE, Christian BJ, Sands D. Responses to chronic illness: analysis of psychological and physiological adaptation. Nursing Research. 1990;39:300–4. [PubMed] [Google Scholar]
- 15.Bobrow K, Brennan T, Springer D, et al. Efficacy of a text messaging (SMS) based intervention for adults with hypertension: protocol for the StAR (SMS Text-message Adherence suppoRt trial) randomised controlled trial. BMC Public Health. 2014;14:28. doi: 10.1186/1471-2458-14-28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Schroeder K, Fahey T, Ebrahim S. Interventions for improving adherence to treatment in patients with high blood pressure in ambulatory settings. Cochrane Database of Systematic Reviews. 2004;(2):CD004804. doi: 10.1002/14651858.CD004804. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Horvath T, Azman H, Kennedy GE, Rutherford GW. Mobile phone text messaging for promoting adherence to antiretroviral therapy in patients with HIV infection. The Cochrane Database of Systematic Reviews. 2012;3:CD009756. doi: 10.1002/14651858.CD009756. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Wangberg SC, Arsand E, Andersson N. Diabetes education via mobile text messaging. Journal of Telemedicine and Telecare. 2006;12:55–6. doi: 10.1258/135763306777978515. [DOI] [PubMed] [Google Scholar]
- 19.da Costa FA, Guerrriro JP, de Melo MN, et al. Effect of reminder cards on compliance with antihypertensive medication. International Journal of Pharmacy Practice. 2005;13:205–11. [Google Scholar]
- 20.Narasimhan K. Text message appointment reminders. American Family Physician. 2013;88:20–1. [PubMed] [Google Scholar]
- 21.Mahtani KR, Heneghan CJ, Glasziou PP, Perera R. Reminder packaging for improving adherence to self-administered long-term medications. Cochrane Database Syst Rev. 2011;9:CD005025. doi: 10.1002/14651858.CD005025.pub3. [DOI] [PubMed] [Google Scholar]
- 22.Strandbygaard U, Thomsen SF, Backer V. A daily SMS reminder increases adherence to asthma treatment: a three-month follow-up study. Respiratory Medicine. 2010;104:166–71. doi: 10.1016/j.rmed.2009.10.003. [DOI] [PubMed] [Google Scholar]
- 23.Kim MT, Hill MN, Bone LR, Levine DM. Development and testing of the Hill-Bone Compliance to High Blood Pressure Therapy Scale. Progress in Cardiovascular Nursing. 2000;15:90–6. doi: 10.1111/j.1751-7117.2000.tb00211.x. [DOI] [PubMed] [Google Scholar]
- 24.Lambert EV, Steyn K, Stender S, et al. Cross-cultural validation of the Hill- Bone compliance to high blood pressure therapy scale in a South African, primary health care setting. Ethnicity & Disease. 2006;16:286–91. [PubMed] [Google Scholar]
- 25.Taher M, Abredari H, Karimy M, et al. The relation between social support and adherence to the treatment of hypertension. Journal of Education and Community Health. 2014;1:63–9. [In Persian] [Google Scholar]
- 26.Ashktorab T, Esmaili Zabihi R, Benaderekhshan H, et al. Correlation between self-concept according to roy adaptation model and adherence to therapeutic health regimen in hypertensive outpatients who attended in one of hospitals affiliated to Urmia University of Medical Science and Health Service. Faculty of Nursing of Midwifery Quarterly. 2011;21:11–16. [In Persian] [Google Scholar]
- 27.Andrade AS, McGruder HF, Wu AW, et al. A programmable prompting device improves adherence to highly active antiretroviral therapy in HIV-infected subjects with memory impairment. Clin Infect Dis. 2005;41:875–82. doi: 10.1086/432877. [DOI] [PubMed] [Google Scholar]
- 28.Hou MY, Hurwitz S, Kavanagh E, et al. Using daily text-message reminders to improve adherence with oral contraceptives: a randomized controlled trial. Obstet Gynecol. 2010;116:633–40. doi: 10.1097/AOG.0b013e3181eb6b0f. [DOI] [PubMed] [Google Scholar]
- 29.Christensen A, Christrup LL, Fabricius PE, et al. The impact of an electronic monitoring and reminder device on patient compliance with antihypertensive therapy: a randomized controlled trial. J Hypertens. 2010;28:194–200. doi: 10.1097/HJH.0b013e328331b718. [DOI] [PubMed] [Google Scholar]
- 30.Santschi V, Wuerzner G, Schneider MP, et al. Clinical evaluation of IDAS II, a new electronic device enabling drug adherence monitoring. Eur J Clin Pharmacol. 2007;63:1179–84. doi: 10.1007/s00228-007-0364-7. [DOI] [PubMed] [Google Scholar]
- 31.Simoni JM, Huh D, Frick PA, et al. Peer support and pager messaging to promote antiretroviral modifying therapy in seattle: A randomized controlled trial. J Acquir Immune Defic Syndr. 2009;52:465–73. doi: 10.1097/qai.0b013e3181b9300c. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Bernocchi P, Scalvini S, Bertacchini F, et al. Home based telemedicine intervention for patients with uncontrolled hypertension: a real life non-randomized study. BMC Medical Informatics and Decision Making. 2014;14:52. doi: 10.1186/1472-6947-14-52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Beune EJ, Moll van Charante EP, Beem L, et al. Culturally adapted hypertension education (CAHE) to improve blood pressure control and treatment adherence in patients of African origin with uncontrolled hypertension: cluster-randomized trial. PlOS ONE. 2014;9:e90103. doi: 10.1371/journal.pone.0090103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Thomas CM. The influence of self-concept on adherence to recommended health regimens in adults with heart failure. The Journal of Cardiovascular Nursing. 2007;22:405–16. doi: 10.1097/01.JCN.0000287037.85067.3d. [DOI] [PubMed] [Google Scholar]
- 35.Albert NM. Improving medication adherence in chronic cardiovascular disease. Critical Care Nurse. 2008;28:54–64. [PubMed] [Google Scholar]
- 36.Perez-Idarraga A, Valencia Gomez K, Gallo Villegas J, et al. Intervention with rumba and nutrition education to modify cardiovascular risk factors in adults with metabolic syndrome. Pan American Journal of Public Health. 2015;37:29–37. [PubMed] [Google Scholar]
- 37.Ingersoll KS, Cohen J. The impact of medication regimen factors on adherence to chronic treatment: a review of literature. Journal of Behavioral Medicine. 2008;31:213–24. doi: 10.1007/s10865-007-9147-y. [DOI] [PMC free article] [PubMed] [Google Scholar]