

Abstract
Background:
As key determinants of many favorable health and quality of life outcomes, it is important to identify factors associated with mobility and social participation. Although several investigations have been carried out on mobility, social participation and neighborhood environment, there is no clear integration of these results. This paper presents a scoping study protocol that aims to provide a comprehensive understanding of how the physical and social neighborhood environment is associated with or influences mobility and social participation in older adults.
Methods:
The rigorous methodological framework for scoping studies is used to synthesize and disseminate current knowledge on the associations or influence of the neighborhood environment on mobility and social participation in aging. Nine databases from public health and other fields are searched with 51 predetermined keywords. Using content analysis, all data are exhaustively analyzed, organized, and synthesized independently by two research assistants.
Discussion:
A comprehensive synthesis of empirical studies provides decision-makers, clinicians and researchers with current knowledge and best practices regarding neighborhood environments with a view to enhancing mobility and social participation. Such a synthesis represents an original contribution and can ultimately support decisions and development of innovative interventions and clear guidelines for the creation of age-supportive environments. Improvements in public health and clinical interventions might be the new innovation needed to foster health and quality of life for aging population. Finally, the aspects of the associations or influence of the neighborhood environment on mobility and social participation not covered by previous research are identified.
Conclusions:
Among factors that impact mobility and social participation, the neighborhood environment is important since interventions targeting it may have a greater impact on an individual's mobility and social participation than those targeting individual factors. Although investigations from various domains have been carried out on this topic, no clear integration of these results is available yet.
Keywords: Mobility, neighborhood environment, older adults, quality of life, scoping study, social participation
INTRODUCTION
What current knowledge needs comprehensive synthesis to inform decision-makers, managers, professionals, and researchers? One example to increase health and quality of life in older adults.
Aging: One of the most important challenges needing innovative interventions to improve the health and quality of life of the population
In industrialized countries, older adults make up a sizeable proportion of the population. Furthermore, between 2000 and 2050, the proportion of the world's population over 60 years will double from about 11% to 22%.[1] By 2050, the world will have almost 400 million people aged 80 years or older. Many people aged 65 and older suffer from chronic diseases such as arthritis and rheumatism (47.3%), hypertension (42.8%), heart disease (19.8%) or diabetes (13.5%), and almost half (42%) have disabilities.[2] Since they have significant consequences for individuals, communities, and social and health services, these demographic challenges represent one of the most important factors influencing our society. Fortunately, chronic diseases and disabilities can be prevented or their onset delayed by public health (e.g., urban planning) and clinical (e.g., rehabilitation) interventions. Nevertheless, both prevention and delay necessitate innovative interventions and human and financial resources. Despite the challenge of the increasing prevalence of chronic disease and disability, industrialized countries have imposed major financial restrictions, limiting public health and clinical interventions.[3] Consequently, the health and quality of life of older adults is a major concern for decision-makers, clinicians and researchers concerned with the older population. Innovative interventions on major modifiable health determinants are thus needed.[4]
Mobility and social participation: Major modifiable determinants of older adults’ health
As one of the key dimensions of successful aging,[5] social participation has been found to be a determinant of many favorable health and quality of life outcomes.[6] Mortality[7] and morbidity[8] have been shown to be associated with limited social participation. Consequently, and as an outcome amenable to change,[9] it is important to identify the factors influencing social participation as a basis for informing and improving public health and clinical interventions. In this study and based on the work done by,[10] social participation has been defined as a person's involvement in social activities that provide social interactions within his/her community or society. Depending on the main goal of these social activities, involvement of the individual with others can be presented in a range of six proximal to distal levels (taxonomy). This taxonomy might be useful in pinpointing the focus of future investigations and clarifying dimensions specific to social participation.[10]
Social participation is conceptualized by the Human Development Model - Disability Creation Process model as resulting from the interaction between personal and environmental factors Figure 1; Fougeyrollas, 2010). Identified as protecting against cognitive decline among community-dwelling older persons,[11] social participation is done primarily for the person's own sake and cannot be delegated to a third party without losing benefits.[12] From a population perspective, older helpers and volunteers are a resource for their families, communities and economies in supportive and enabling living environments.[13] Social participation has been shown to be closely related to mobility in the community[14] and home,[15] and to decline as a result of the “normal” aging process.[16,17] Social participation can be optimized by public health[18] and clinical[19] interventions. Disability and environmental factors are among the most important determinants of social participation because greater disability and lack of neighborhood resources can restrict social participation[20] and decrease the likelihood of independent living.[21] In fact, disability, defined as any disturbance resulting from an impairment in the capacity to perform a physical or mental activity considered normal for a human being,[22] has been found to be one of the most powerful determinants of social participation.[23,24,25,26,27,28,29,30,31,32,33]
Figure 1.

Human Development Model - Disability Creation Process (HDM - DCP)
As an intrinsic dimension of the person, mobility disability is common among older adults.[34,35] For example, in Canada, more than 1.1 million people[36] and approximately half of people aged 65 and older have restricted mobility.[2,4] According to,[4] “Mobility is broadly defined as the ability to move oneself (e.g., by walking, using assistive devices, or taking transportation) within community environments that expand from one's home, to the neighborhood, and to regions beyond.” It can thus be qualified in relation to life-space, from home to community. As a critical element of older adults’ health, diminished mobility has been associated with a sedentary lifestyle,[37,38,39,40] obesity,[37,40,41] physical disability,[21,42,43,44] lower quality-of-life,[42,45,46] premature mortality,[47,48,49] and increased health care costs.[50,51] It has been shown that older adults with access to private or public transportation participate more frequently in social activities. Community mobility using transportation, especially active or public transportation, is favorable to older adults’ health.[52] Indeed, such sustainable modes of transportation simultaneously encourage physical activity and reduce local traffic-related air pollution, both known to be associated with cardiovascular and other chronic diseases.[53] In addition to individual factors such as health problems that affect muscle strength and balance, some environmental challenges such as constraints that involve physical loading and postural transitions (e.g., sloping terrain or stairs) can specifically influence mobility.[54,55] As for social participation, although empirical evidence exists, a clear understanding of how environmental factors are associated with or influence mobility in older adults is nevertheless needed.
Optimizing the neighborhood environment: One promising intervention strategy to enhance mobility and social participation in aging
Environmental factors are important[56] since interventions targeting them may have a greater impact on individual and population mobility and social participation than those targeting individual factors,[57] including disability. The environment is defined by the physical and social characteristics in which people live.[58] Among the characteristics of the environment, neighborhood living conditions are important for health and well-being, especially for older adults. Compared to adults in the workforce, older adults are more place-bound,[59,60] that is, spend more time each day in their neighborhood and stay longer in the same residential environment.[2,61] In this study and based on,[62] neighborhood environment includes, but is not restricted to: Built environment, that is, characteristics of the physical context including aspects of urban design (e.g., presence of sidewalks), traffic density and speed, distance to and design of venues for physical activity such as walking (e.g., parks and access to services), aesthetics, crime and safety. Since mobility is also influenced by social aspects of the environment,[4] that is, support and associations, attitude, services, systems and policies, it is necessary to consider the neighborhood environment and not only the built environment. In comparison to the current population of older adults, future generations of older adults will likely have a better expectancy of years in good health[2] and as a result, a larger proportion will have the potential for higher levels of mobility and social participation. This further emphasizes the need for future interventions to improve neighborhood living conditions to enhance mobility and social participation in this population.
In an effort to shape active aging as a lifelong process, the World Health Organization challenged not only neighborhoods but also cities to become more age-friendly in order to take advantage of the potential that older people represent for humanity.[13] An age-friendly city encourages active aging by optimizing opportunities for health, participation and security in order to enhance quality of life as people age. To encourage mobility and social participation, an age-friendly city adapts its structures and services to be accessible to and inclusive of older people with varying needs and capacities.[13] Eight issues and concerns have been voiced by older people as characteristics of an age-friendly city: (1) Outdoor spaces and buildings; (2) transportation; (3) housing; (4) social participation; (5) respect and social inclusion; (6) civic participation and employment; (7) communication and information; and (8) community support and health services. Taking these issues into consideration, and in accordance with the theoretical perspective of,[61] neighborhood facilitators (i.e., helpful environmental factors, such as flexibility, environmental prostheses, resource availability, engagement opportunities, and social support) can support personal capabilities such as mobility, which can in turn enable greater social participation.[57,61] In contrast, environmental obstacles (e.g., physical barriers, inaccessibility of services and amenities, social stress, and resource inadequacy) can challenge and exceed personal capabilities, thereby limiting social participation. Indeed, support from the social environment[61,63] and accessibility in the physical neighborhood environment[61,64,65,66,67] are seen as imperatives for helping individuals with disabilities living in the community.[61,68,69]
According to empirical studies, neighborhood characteristics such as living in close proximity to services[70,71] have been shown to be important in performing activities to meet daily needs, including access to food shopping, health services, public transportation, banking and social clubs. Most individual behaviors, e.g., walking to the grocery store versus taking the car, are influenced by the neighborhood environment. Moreover, local resources may have an impact on initiating and maintaining social links with community members.[71] The closing of nearby services has been shown to be worrisome,[71] especially for women considering the prospect of not being able to drive or concerned about declines in mobility.[70] For someone with diminished physical endurance, walking distance or perceived walking distance between the home and neighborhood resources may be critical. Previous research in sociology showed that older adults living in resource affluent areas were less likely to have low levels of social functioning, independently of individual demographic and socioeconomic characteristics.[72] Individuals’ perceptions of the area as neighborly and having good facilities were also independently associated with a higher likelihood of social activities[72] and well-being.[73] The presence of local resources may affect the likelihood of initiating and maintaining social ties with members of the community.[74] For instance, older people living in an environment with a lot of resources have a higher level of social participation independently of individual demographic and socioeconomic characteristics. A neighborhood perceived as friendly and well-appointed has also been reported to be associated independently with an increased likelihood of participation in social activities.[75] Walking distance, weather conditions, terrain characteristics, external physical loads, demands on attention, and traffic levels can all influence community mobility[42,76,77,78] and social participation.[79] Finally, architectural (e.g., porches) and neighborhood design features can promote interaction among individuals in a neighborhood.[80] Although studies from various domains have been done on mobility, social participation and neighborhood environments, no clear integration of these results is available yet.
Integrated knowledge of empirical studies of the neighborhood environment and its influences on mobility and social participation: What is missing from the literature
Despite widespread acceptance of the importance of the neighborhood environment for mobility and social participation, a rigorous and comprehensive portrait integrating the results of the studies done is still lacking. Two ecological models of health [Figure 2],[40,81] including multiple aspects such as the neighborhood environment, have been developed recently to reduce communication difficulties and stimulate collaboration across disciplines (e.g., public health, rehabilitation, and gerontology). Moreover, recent advances have been made in the conceptualization (theoretical organization of a concept) of mobility[4] and social participation,[10] and the operationalization (measurement) of the environment.[82] Such efforts are required to allow optimal comprehension of research results,[83] especially given the interesting, diverse and large number of studies (results reported above and others) and recent theoretical advances. It is thus timely, innovative and essential to carry out a comprehensive synthesis of the existing literature in order to gain fundamental knowledge and better understand how neighborhood is associated with or influences mobility and social participation.[73]
Figure 2.
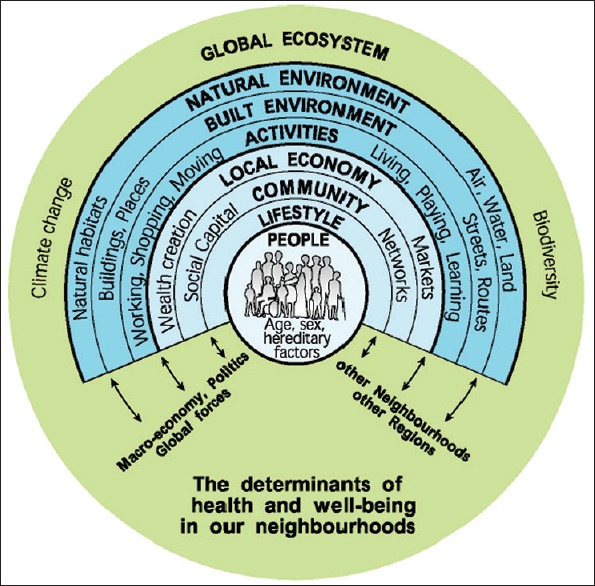
Human Development Model - Disability Creation Process (HDM - DCP)
Note: Adapted from: Fougeyrollas, P. (2010). Le funambule, le fil et la toile. Transformations réciproques du sens du handicap. [The tightrope walker, wire and canvas. Reciprocal transformations of the meaning of disability] Presses de l’Université Laval
Mobility, social participation, and the neighborhood environment: The knowledge that needs to be integrated by decision-makers and researchers to improve the health of older adults
The main objective of this paper was to present a scoping study protocol that aims to provide a comprehensive understanding of how the physical and social neighborhood environment is associated with or influences mobility and social participation in older adults. Such a synthesis of the research is needed to inform decision-makers, clinicians, and researchers about current knowledge and best practices regarding how the neighborhood environment enhances mobility and social participation. This synthesis represents an original contribution and ultimately supports decisions and the development of innovative interventions and clear guidelines. For example, environmental accessibility or barrier guidelines and community-based interventions could provide ways to increase facilitators and reduce obstacles within the neighborhood environment, resulting in improved mobility and social participation by older adults. Such improvements in public health and clinical interventions might be the new innovation needed to foster health and quality of life for aging population.
HOW TO CONDUCT A SCOPING STUDY (METHODS): DESCRIPTION OF HOW THE PROJECT ON THE NEIGHBOURHOOD ENVIRONMENT IS CARRIED OUT AS AN EXAMPLE
To synthesize and disseminate current knowledge on the associations or influence of the neighborhood environment on mobility and social participation in aging, the methodological framework for scoping studies is used.[84,85,86,87] Scoping studies are specifically designed to “…identify gaps in the evidence base where no research has been conducted” and to “…summarize and disseminate research findings (p. 21).”[84] Epistemological and ontological assumptions underlying the methodology of scoping studies are situated in between positivist and naturalist methodological traditions. Indeed, the scoping methodology follows rigorous steps and a systematic process of study selection. It also considers both quantitative and qualitative research, and involves summarizing the results of studies without specifically pooling the data or evaluating the quality of the studies. By conducting scoping studies, researchers can generate original results and endeavor to implement the evidence-based knowledge. In the present project, partnership with decision-makers and knowledge-users enables the synthesis of current evidence regarding the neighborhood environment, mobility, and social participation. This is a relatively novel field of expertise where, to our knowledge and probably due to challenges in diversity and concepts, a full synthesis of the literature does not exist. The partnership in the current project fosters not only fast and effective knowledge translation, but also the development of innovative interventions and guidelines on the neighborhood environment, mobility and social participation. As a scoping study is a rigorous literature review that synthesizes and disseminates current knowledge, evaluation by an ethics committee was not required.
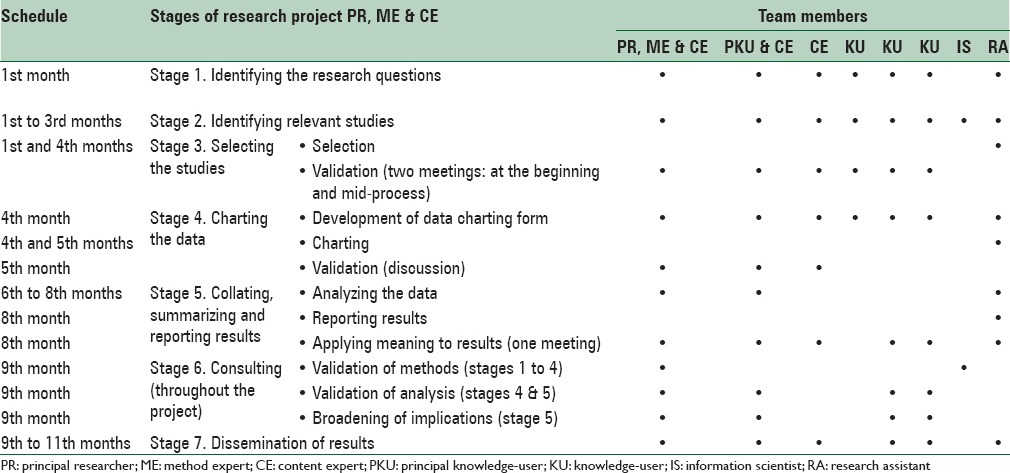
The framework for the scoping study[84,85,86,87] includes seven stages [Table 1] that involve specific tasks currently in process, clearly outlined (as proposed in the present project) and under the responsibility of each of the research team members. Moreover, a guide on the collaboration between researchers and knowledge-users in health research is used to optimize this multidisciplinary partnership.[88]
Table 1.
Roles and responsibilities of each team member in the seven stages of the scoping study
Identifying the research questions (Stage 1)
Based on a comprehensive approach, maximizing the pertinence and probability of knowledge translation, the research questions were determined by the research team (experts, knowledge-users and research assistants). Specifically, the research questions emerged from the two team leaders: The principal researcher and the principal knowledge-user, and were refined through discussion with the team. To optimally map current knowledge on the associations or influence of the neighborhood environment on mobility and social participation in aging population, the research questions are broad and based on the Human Development Model - Disability Creation Process[89] and the theoretical framework for population health and environment,[81] as well as clear definitions of all related concepts.[85] Three questions are specifically addressed:
What are the social and physical aspects of the neighborhood environment which have been shown to be associated with or influence mobility and social participation in older adults?
How is the neighborhood environment associated with or how does it influence mobility and social participation in older adults?
Which aspects of the neighborhood environment have not been covered by previous research on mobility and social participation in older adults?
Identifying relevant studies (Stage 2)
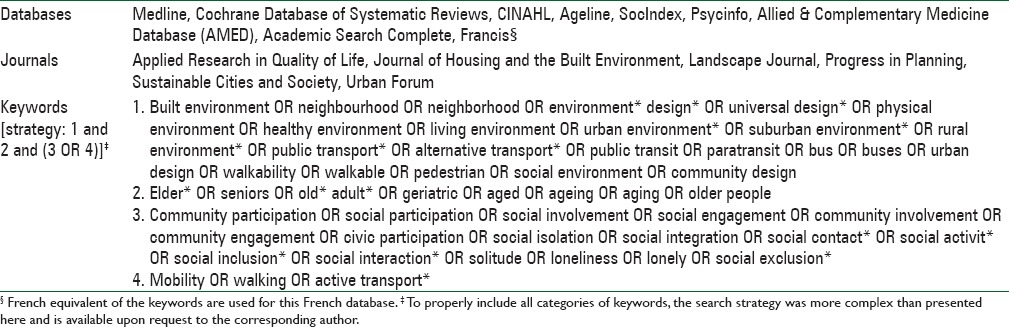
Considering the multidisciplinary nature of the research questions outlined above, the strategy of the present scoping study is designed for the active participation of all team members: Experts, knowledge-users, researchers, and information scientists from different fields [Table 1]. An electronic search is first conducted by one specially trained research assistant supervised by the principal researcher and information scientist. The selected databases and specific related keywords [Table 2] used to carry out the electronic search are validated by all team members. The search is limited to studies published in English and French between January 1980 and the 4th month of the current project. This timeline allows retrieval of up-to-date research, as the concepts evolve and are defined and identification of the studies is completed (Stage 2) within the expected timeframe. To optimize search results, keywords vary according to the specificity of each database and when relevant, consider Medical Subject Headings (MeSH; Table 2).
Table 2.
Databases, journals and keywords chosen
Selecting the studies (Stage 3)
A systematic team approach is used to properly select the studies.[85] First, studies are screened for eligibility by title and, when available, by abstract, by two research assistants who duplicate the screening [Table 1]. The research assistants are specifically trained and supervised by the principal researcher and information scientist. All studies that comprehensively inform about the associations or influence of the neighborhood environment on mobility and social participation are retained. The selection of relevant literature is restricted, though not exclusively (retained if it also presents results specific to adults), to papers on older adults. Extended search strategies include other studies found with a manual search of bibliographies, health-related Websites (e.g., health and social services department, agencies and institutions) and journals of interest (e.g., Health and Place, Annual Review of Public Health and BMC Public Health). Relevant studies proposed by the team members and selected experts in the field of public health, rehabilitation, and gerontology are also included. Studies are excluded if they: (1) Focus on narrow concepts (e.g., only on participation in a seniors’ center or volunteering or home mobility, nursing home, gait, fear, migration, rehabilitation, physical functions, car settings, physical activity other than walk, daily activity, voluntary) or broader ones (e.g., exclusively on sociocultural, economic or policy aspects of the environment), (2) report expert opinions or conference proceedings (often not providing sufficient information), or (3) study specific population (e.g., people with diabetes or visual problems). To discuss and resolve any ambiguity concerning study selection, the research assistants meet regularly with the principal researcher once a week. To ensure the clinical and managerial relevance of the study selection, team meetings with all team members are also held at the beginning (first group meeting) and in the middle (second group meeting) of this process. Final selection of all studies to be included is made in agreement with the two research assistants. Any disagreements are submitted to a third person on the team (principal knowledge-user). To ensure transparency and reproducibility of the process,[85] a flow chart of the systematic literature search following PRISMA-guidelines[90] is carried out and methodological choices are documented.
Charting the data (Stage 4)
From a preliminary reading, all selected studies are first categorized into two groups describing the neighborhood's associations or influence on: (1) Mobility, or (2) social participation. To characterize the selected studies based on association or influence of the neighborhood on mobility (Group 1) or social participation (Group 2), contextual data (template in Appendix 1) are first collected according to the year of publication; country of origin; type of study (e.g., research paper); type of study design (if applicable); sampling method (random, purposeful, convenience, not reported); characteristics of participants (age, gender, etc.); characteristics and operationalization (objective measures, subjective measures or both) of neighborhood; operationalization (self-reported measures, observed measures or both) of mobility; conceptualization and operationalization (objective measures, subjective measures) of social participation; and setting (rural, urban or both). Main quantitative or qualitative findings of the selected studies, that is, the data that are analyzed in the current study, are also summarized (template in Appendix 2) according to how the neighborhood environment is associated with or influences (i.e., significantly positively [+], significantly negatively [−] or insignificantly [0] mobility and social participation.
Appendix 1.
Study Summary
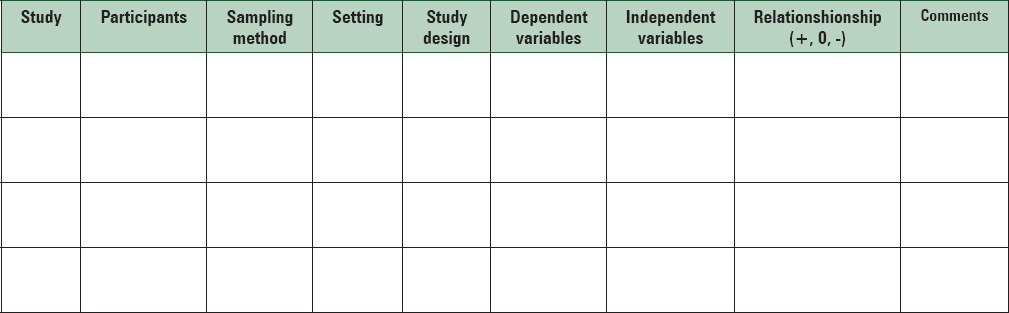
Emerging categories for each group are then identified and lead to the collective development of the data charting form by the research team (templates in Appendices 1 and 2 and Table 1). Following this approach, it is possible for similar factors examined in different studies to be classified under the same category (e.g., density of neighborhood and proximity to neighborhood resources). Specifically, the development of the charting form is led by both the principal researcher and principal knowledge-user with the collaboration of the rest of the team. Considering the iterative nature of scoping studies, the data charting form evolved with the data collating process.[85] Finally, data are independently extracted and categorized by the two research assistants. Validation of the process, including the data charting form and its relevance to the research questions, is provided by a team discussion [Table 1] involving experts and knowledge-users after the first ten selected studies, and subsequently as required.
Collating, summarizing, and reporting results (Stage 5)
Three stages are followed to collate, summarize, and report the results: (a) Analyzing the data; (b) reporting results; and (c) applying meaning to the results.[85]
Analyzing the data
Contextual data are first analyzed through descriptive statistics (means and standard deviations or frequencies and percentages according to number and type of variable, continuous or categorical, respectively). Using content analysis performed independently by the two research assistants,[91] data from previous studies are exhaustively analyzed, organized, and synthesized according to the three research questions. Analyses are also discussed, and one-third are co-coded by the principal researcher or principal knowledge-user. More specifically, within each research question, initial categories are grouped by meaning, synthesized, and then classified into coherent, consistent, relevant, clearly defined and productive themes.[91] Such qualitative methods of analysis of the documents ensure credibility and strength of the results.[85]
Reporting results
The principal researcher and research assistants report current analyzed data numerically with graphics, tables and figures. Narrative data are synthesized into relevant themes. Each theme is: (1) Reported to illustrate associations or influence of the neighborhood environment, and (2) contrasted to show similarities and differences relating to mobility and social participation. The best approach for optimal reporting of the results of the study is adapted for various target audiences (researchers, decision-makers, and clinicians; Figure 3).
Figure 3.
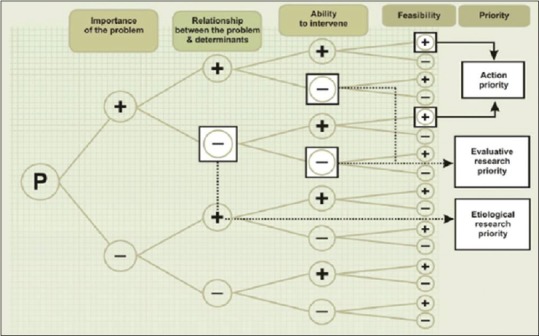
’Health prioritizing’ from a residents training course entitled ‘Assessing needs and prioritizing their health: approaches and challenges’ by Raynald Pineault (2009)
Applying meaning to results
Through discussion with content experts and knowledge-users (third group meeting), implications of the results are challenged and when possible, broadened to include aspects of public health, rehabilitation and gerontology. As their contribution provides direct relevance and feasibility input, the implications provided by the knowledge-users are essential, which supports their significant involvement in the current and following stages of the project [Table 1]. Recommendations consider clinical as well as population and municipal implications.
Consulting (Stage 6)
Inherently part of the research project, knowledge-users ensure clinical relevance of the results and a process congruent with an integrated approach to knowledge translation. As mentioned, and specifically to optimize the methodology of the research project and to guide data collection and analysis, group meetings are conducted twice in Stage 3 and once in Stage 5 [Table 3]. Furthermore, the involvement of researchers and collaborators from different fields (public health, rehabilitation, and gerontology) ensure complementary and multidisciplinary visions of the project. Group meetings allow the findings to be discussed and validated. This collaborative process involves preliminary findings from Stage 5 (in the form of a framework, themes, or list of findings). Based on these results, knowledge-users have the opportunity to support their decisions and interventions based on the evidence and offer a higher level of meaning, content expertise, and perspective to the preliminary findings. This stage is also considered the beginning of knowledge transfer (dissemination strategies).
Table 3.
Dissemination strategies for knowledge generated and expected outcomes
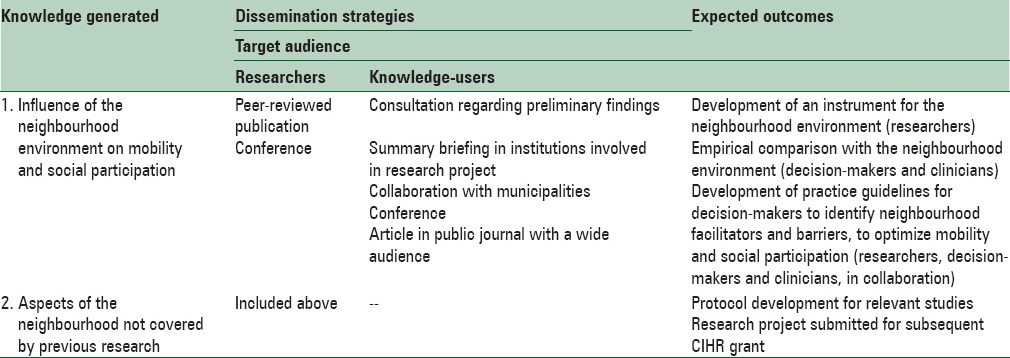
Dissemination of results (Stage 7)
Congruent with an integrated knowledge translation process, various dissemination strategies targeting a wide audience (researchers and knowledge-users including both decision-makers and clinicians) are used [Table 3].
DISCUSSION
First the feasibility, then the potential outcomes of this project will be addressed. Finally, the strengths and limitations will be discussed.
How to demonstrate that the project is feasible: An example of specification from one research team on the neighborhood environment
The feasibility of this scoping study is first assured by the quality and experience of the research team. Researchers and collaborators have been selected strategically, based on their expertise and the qualities required to successfully complete this scoping study. Team members include researchers from health sciences (n = 2), knowledge-users from 5 different types of institutions (Public Health Department, Health and Social Services Agency, Quebec Urban Planners Association, Sherbrooke Transit Authority and Sherbrooke Healthy City), two collaborators specializing in scoping studies, and one information scientist. From a methodological perspective, two team members have already completed or participated in a total of eight scoping studies. Furthermore, the strong multidisciplinary approach ensures optimal realization and dissemination of the results of the present scoping study. Specific contributions from researchers and collaborators to major decisions regarding coordination, study selection and analysis of results [Table 1] also facilitate successful involvement of the team members. In addition, the present scoping study has been designed with specific objectives that can be attained within the grant timeline and funding. Researchers and team members have already agreed to divide the work efficiently into stages (study identification and selection, data charting and analysis, dissemination of results), facilitating completion of the overall scoping study. In short, the research team possesses all of the expertise needed to carry out this scoping study, as well as to ensure clinical pertinence and exhaustive dissemination of results to primary knowledge-users. As all members have agreed to contribute sufficient time to move this project forward, innovative, and significant outcomes are expected.
What outcomes are expected from this project?
Results obtained from this scoping study will provide a greater understanding of how the neighborhood environment is associated with or influences mobility and social participation in older adults.[40] Knowledge generated by the present project will first be useful in providing decision-makers, clinicians, and researchers with current knowledge and best practices regarding how the neighborhood environment is associated with or influences mobility and social participation. Indeed, since the results will help them choose or develop clear guidelines and innovative interventions to increase neighborhood facilitators and reduce environmental obstacles with a view to improving mobility and social participation among older adults, the results will also have policy implications. Identifying aspects of the neighborhood environment that are associated with or influence population health/well-being as well as health behaviors (e.g., use of active or public transportation) will help to promote community-driven development[92] or active living in older adults, which is one of the goals of our knowledge-users. For example, knowledge-users and decision-makers in the municipality use the results of the scoping study to support projects or make decisions about financial investments in urban planning and public safety (modifications to the neighborhood environment that encourage mobility and social participation). Finally, by being part of the overall current scoping study, the decision-makers and knowledge-users will also better understand the scientific validity of scoping studies and be more inclined to use this new knowledge as a guide for decision-making. A better interpretation and greater use of research findings to solve neighborhood problems (e.g., lack of accessibility of recreation facilities or few opportunities for community integration) and address key mobility and social participation issues (e.g., review public transit or intervene to reduce ageism) will thus be encouraged.[93] Moreover, such collaboration also fosters changes in the way researchers think and clinicians act, and how society uses knowledge. Health professionals (occupational/physical therapists, doctors, kinesiologists, etc.) who aim to foster their clients’ mobility and social participation also benefit from the knowledge generated by the present scoping study. Undergraduate, graduate, and postgraduate education in various disciplines could be adapted to help clinicians understand the associations or influence of neighborhood environments on mobility and social participation. Such an integration of knowledge through education and across a variety of disciplines could foster interprofessional collaboration, which supports interventions in a context of complexity.[94]
Researchers will also benefit from the knowledge and collaboration generated by the scoping study that help to identify areas where insufficient evidence exists on the associations or influence of the neighborhood environment on mobility and social participation. Initiation of collaboration with primary knowledge-users (decision-makers and clinicians) and co-researchers from multiple disciplines (health sciences, public health, and urban planning) through the present project will lead to the development and implementation of a high-quality novel research program on the associations or influence of the neighborhood environment on mobility and social participation. The original knowledge that will be generated from this scoping study will lead to the development of an instrument or practice guidelines to optimize positive influences of the neighborhood environment on mobility and social participation. Moreover, the present scoping study represents the first stage of a research program that uses the same teams (experts, collaborators and knowledge-users) that have already worked together. The emerging team developed a research program to: (1) Identify key age- and gender-specific neighborhood environment determinants of mobility and social participation, controlling for individual factors such as tobacco use, body composition (obesity, nutrition) and energy expenditure (physical exercise); (2) develop health-related analytical geomatic tools (interactive atlas) that monitor these relevant neighborhood environmental features from extended continuous recordings; and (3) develop efficient knowledge transfer protocols for clinicians and decision-makers in the form of better clinical toolkits (scales or portable devices) for assessing the impact of intervention strategies on mobility and social participation. This innovative research program will eventually lead to the development of specific intervention strategies, including more comprehensive legislation and policies that can prevent mobility and social participation inequalities by optimizing neighborhood environment issues. Such innovations will ultimately help to improve health and quality of life in the population in general and especially in the older population.
Strengths and limitations
As mentioned, this study uses the rigorous methodological framework for scoping studies,[84,85,86,87] including the comprehensive retrieval of studies on the neighborhood environment, mobility and social participation, in numerous multidisciplinary databases. In addition, results from quantitative studies are completed and extended by results from qualitative studies,[95] which help to understand how the neighborhood environment influences mobility and social participation. Although the particular epistemological and ontological assumptions underlying the methodology (positivist, interpretive, postmodern, etc.) of scoping studies have not been identified, they are situated in between positivist and naturalist methodological traditions. Enriched by the close collaboration of knowledge-users from different fields (public health, urban planning, transportation planning, rehabilitation and gerontology) in a variety of institutions (health agencies, public transit authorities and municipalities), the results provide an accurate and up-to-date synthesis of the literature on how the neighborhood environment is associated with or influences mobility and social participation in older adults. Through the synergy of an exceptional research team, exhaustive dissemination of the results to knowledge-users is also easier to attain. As mentioned, a guide on the collaboration between researchers and knowledge-users in health research is used to optimize the multidisciplinary partnership.[88] Moreover, the aspects that have not been covered by previous research on the influence of the neighborhood environment on mobility and social participation are identified to inform future interdisciplinary research. However, as in other scoping studies,[84] the current project does not systematically combine empirical results of previous studies or provide a detailed appraisal of the quality of the evidence. Furthermore, as textbooks are not systematically included, information available in some textbooks may be missed. The impact of this should nonetheless be minimal since textbooks are generally not a primary source of empirical results. Although carefully reviewed, retrieval of studies on the neighborhood environment, mobility and social participation is challenging as associated key words are numerous and some of them (e.g., walk) might generate many irrelevant results. Finally, definitions and measures of neighborhood environment, mobility, and social participation differ greatly among studies, which increases the complexity of the synthesis of the literature.
CONCLUSIONS
As they influence health and are amenable to change, mobility and social participation are key targets of public health and clinical interventions. Among factors that impact mobility and social participation, the neighborhood environment is important since interventions targeting it may have a greater impact on an individual's mobility and social participation than those targeting individual factors. Although investigations from various domains have been carried out on this topic, no clear integration of these results is available yet. The main objective of this scoping study is to provide a comprehensive understanding regarding how the neighborhood environment is associated with or influences mobility and social participation in older adults. A comprehensive synthesis of studies provides decision-makers, clinicians, and researchers with current knowledge and best practices concerning the neighborhood environment with a view to enhancing mobility and social participation. Such a synthesis represents an original contribution and ultimately supports decisions and the development of innovative interventions and clear guidelines for the creation of age-supportive environments. Considering neighborhood facilitators and obstacles, improvements in public health and clinical interventions might thus be the new innovation needed to foster health and quality of life for aging population. Finally, the aspects of the association of the neighborhood environment with mobility and social participation that have not been covered by previous research will be identified and lead future investigations.
ACKNOWLEDGEMENTS
This study is supported by the Canadian Institutes for Health Research (#KAS-116 630). Thanks to Claude Beaulac from the Ordre des urbanistes du Québec (Quebec urban planners association) for his contribution.
Footnotes
Source of Support: Canadian Institutes for Health Research (#KAS-116 630).
Conflict of Interest: None declared.
REFERENCES
- 1.World Health Organization. [Last accessed on 2015 Apr 16]. Available from: http://www.who.int/features/factfiles/ageing/en/
- 2.Turcotte M, Schellenberg G. Ottawa: Statistics Canada; 2007. A Portrait of Seniors in Canada 2006. [Google Scholar]
- 3.Hébert R. Autonomy insurance: An essential innovation in response to the challenges of aging. Can J Aging. 2012;31:1–11. doi: 10.1017/S0714980811000614. [DOI] [PubMed] [Google Scholar]
- 4.Webber SC, Porter MM, Menec VH. Mobility in older adults: A comprehensive framework. Gerontologist. 2010;50:443–50. doi: 10.1093/geront/gnq013. [DOI] [PubMed] [Google Scholar]
- 5.Rowe JW, Kahn RL. Successful aging. Gerontologist. 1997;37:433–40. doi: 10.1093/geront/37.4.433. [DOI] [PubMed] [Google Scholar]
- 6.Bath PA, Deeg DJ. Social engagement and health outcomes among older people: Introduction to a special section. Eur J Ageing. 2005;2:24–30. doi: 10.1007/s10433-005-0019-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Berkman LF. The role of social relations in health promotion. Psychosom Med. 1995;57:245–54. doi: 10.1097/00006842-199505000-00006. [DOI] [PubMed] [Google Scholar]
- 8.Berkman LF, Glass T, Brissette I, Seeman TE. From social integration to health: Durkheim in the new millennium. Soc Sci Med. 2000;51:843–57. doi: 10.1016/s0277-9536(00)00065-4. [DOI] [PubMed] [Google Scholar]
- 9.Abu-Rayya HM. Depression and social involvement among elders. Internet J Health. 2006;5:9. [Google Scholar]
- 10.Levasseur M, Richard L, Gauvin L, Raymond E. Inventory and analysis of definitions of social participation found in the aging literature: Proposed taxonomy of social activities. Soc Sci Med. 2010;71:2141–9. doi: 10.1016/j.socscimed.2010.09.041. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Zunzunegui MV, Alvarado BE, Del Ser T, Otero A. Social networks, social integration, and social engagement determine cognitive decline in community-dwelling Spanish older adults. J Gerontol B Psychol Sci Soc Sci. 2003;58:S93–100. doi: 10.1093/geronb/58.2.s93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Maier H, Klumb PL. Social participation and survival at older ages: Is the effect driven by activity content or context. Eur J Ageing. 2005;2:31–9. doi: 10.1007/s10433-005-0018-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Geneva, Switzerland: World Health Organization; 2007. World Health Organization. Global Age-friendly Cities: A Guide. [Google Scholar]
- 14.Verdonschot MM, de Witte LP, Reichrath E, Buntinx WH, Curfs LM. Impact of environmental factors on community participation of persons with an intellectual disability: A systematic review. J Intellect Disabil Res. 2009;53:54–64. doi: 10.1111/j.1365-2788.2008.01128.x. [DOI] [PubMed] [Google Scholar]
- 15.Hamzat TK, Kobiri A. Effects of walking with a cane on balance and social participation among community-dwelling post-stroke individuals. Eur J Phys Rehabil Med. 2008;44:121–6. [PubMed] [Google Scholar]
- 16.Desrosiers J, Robichaud L, Demers L, Gélinas I, Noreau L, Durand D. Comparison and correlates of participation in older adults without disabilities. Arch Gerontol Geriatr. 2009;49:397–403. doi: 10.1016/j.archger.2008.12.006. [DOI] [PubMed] [Google Scholar]
- 17.Desrosiers J, Noreau L, Rochette A. Social participation of older adults in Quebec. Aging Clin Exp Res. 2004;16:406–12. doi: 10.1007/BF03324572. [DOI] [PubMed] [Google Scholar]
- 18.Fujiwara Y, Watanabe N, Nishi M, Ohba H, Lee S, Kousa Y, et al. Indirect effects of school volunteering by senior citizens on parents through the “REPRINTS” intergenerational health promotion program. Nippon Koshu Eisei Zasshi. 2010;57:458–66. [PubMed] [Google Scholar]
- 19.Meriano C, Latella D. Thorofare, NJ: SLACK Incorporated; 2008. Occupational Therapy Interventions. Function and Occupations; pp. 423–55. [Google Scholar]
- 20.Rimmer JH, Riley B, Wang E, Rauworth A. Accessibility of health clubs for people with mobility disabilities and visual impairments. Am J Public Health. 2005;95:2022–8. doi: 10.2105/AJPH.2004.051870. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Brach JS, VanSwearingen JM. Physical impairment and disability: Relationship to performance of activities of daily living in community-dwelling older men. Phys Ther. 2002;82:752–61. [PubMed] [Google Scholar]
- 22.Fougeyrollas P, Noreau L, Bergeron H, Cloutier R, Dion SA, St-Michel G. Social consequences of long term impairments and disabilities: Conceptual approach and assessment of handicap. Int J Rehabil Res. 1998;21:127–41. doi: 10.1097/00004356-199806000-00002. [DOI] [PubMed] [Google Scholar]
- 23.D’Alisa S, Baudo S, Mauro A, Miscio G. How does stroke restrict participation in long-term post-stroke survivors? Acta Neurol Scand. 2005;112:157–62. doi: 10.1111/j.1600-0404.2005.00466.x. [DOI] [PubMed] [Google Scholar]
- 24.Jette AM, Keysor J, Coster W, Ni P, Haley S. Beyond function: Predicting participation in a rehabilitation cohort. Arch Phys Med Rehabil. 2005;86:2087–94. doi: 10.1016/j.apmr.2005.08.001. [DOI] [PubMed] [Google Scholar]
- 25.Rochette A, Desrosiers J, Noreau L. Association between personal and environmental factors and the occurrence of handicap situations following a stroke. Disabil Rehabil. 2001;23:559–69. doi: 10.1080/09638280010022540. [DOI] [PubMed] [Google Scholar]
- 26.Harwood RH, Gompertz P, Ebrahim S. Handicap one year after a stroke: Validity of a new scale. J Neurol Neurosurg Psychiatry. 1994;57:825–9. doi: 10.1136/jnnp.57.7.825. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Bourdeau I, Desrosiers J, Gosselin S. Predictors of reintegration to normal living in older adults discharged from an intensive rehabilitation program. Int J Rehabil Res. 2008;31:267–74. doi: 10.1097/MRR.0b013e3282fc0ff2. [DOI] [PubMed] [Google Scholar]
- 28.Clarke PJ, Black SE, Badley EM, Lawrence JM, Williams JI. Handicap in stroke survivors. Disabil Rehabil. 1999;21:116–23. doi: 10.1080/096382899297855. [DOI] [PubMed] [Google Scholar]
- 29.Sturm JW, Dewey HM, Donnan GA, Macdonell RA, McNeil JJ, Thrift AG. Handicap after stroke: How does it relate to disability, perception of recovery, and stroke subtype.: The north North East Melbourne Stroke Incidence Study (NEMESIS)? Stroke. 2002;33:762–8. doi: 10.1161/hs0302.103815. [DOI] [PubMed] [Google Scholar]
- 30.Everard KM, Lach HW, Fisher EB, Baum MC. Relationship of activity and social support to the functional health of older adults. J Gerontol B Psychol Sci Soc Sci. 2000;55:S208–12. doi: 10.1093/geronb/55.4.s208. [DOI] [PubMed] [Google Scholar]
- 31.Levasseur M, Desrosiers J, St-Cyr Tribble D. Do quality of life, participation and environment of older adults differ according to level of activity? Health Qual Life Outcomes. 2008;6:30. doi: 10.1186/1477-7525-6-30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.De Haan R, Horn J, Limburg M, Van Der Meulen J, Bossuyt P. A comparison of five stroke scales with measures of disability, handicap, and quality of life. Stroke. 1993;24:1178–81. doi: 10.1161/01.str.24.8.1178. [DOI] [PubMed] [Google Scholar]
- 33.Wilkie R, Peat G, Thomas E, Croft P. Factors associated with participation restriction in community-dwelling adults aged 50 years and over. Qual Life Res. 2007;16:1147–56. doi: 10.1007/s11136-007-9221-5. [DOI] [PubMed] [Google Scholar]
- 34.Gardener EA, Huppert FA, Guralnik JM, Melzer D. Middle-aged and mobility-limited: Prevalence of disability and symptom attributions in a national survey. J Gen Intern Med. 2006;21:1091–6. doi: 10.1111/j.1525-1497.2006.00564.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Topinková E. Aging, disability and frailty. Ann Nutr Metab. 2008;2:6–11. doi: 10.1159/000115340. [DOI] [PubMed] [Google Scholar]
- 36.Statistics Canada. Disability in Canada: A 2001 Profile. Report N 89-577-XIF. 2001. [Last accessed on 2015 Apr 16]. Available from: http://publications.gc.ca/Collection/Statcan/89-577-X/89-577-XIE2001001.pdf .
- 37.Bouchard DR, Beliaeff S, Dionne IJ, Brochu M. Fat mass but not fat-free mass is related to physical capacity in well-functioning older individuals: Nutrition as a determinant of successful aging (NuAge) – The Quebec Longitudinal Study. J Gerontol A Biol Sci Med Sci. 2007;62:1382–8. doi: 10.1093/gerona/62.12.1382. [DOI] [PubMed] [Google Scholar]
- 38.Koster A, Patel KV, Visser M, van Eijk JT, Kanaya AM, de Rekeneire N, et al. Joint effects of adiposity and physical activity on incident mobility limitation in older adults. J Am Geriatr Soc. 2008;56:636–43. doi: 10.1111/j.1532-5415.2007.01632.x. [DOI] [PubMed] [Google Scholar]
- 39.Yeom HA, Fleury J, Keller C. Risk factors for mobility limitation in community-dwelling older adults: A social ecological perspective. Geriatr Nurs. 2008;29:133–40. doi: 10.1016/j.gerinurse.2007.07.002. [DOI] [PubMed] [Google Scholar]
- 40.Koster A, Penninx BW, Newman AB, Visser M, van Gool CH, Harris TB, et al. Lifestyle factors and incident mobility limitation in obese and non-obese older adults. Obesity (Silver Spring) 2007;15:3122–32. doi: 10.1038/oby.2007.372. [DOI] [PubMed] [Google Scholar]
- 41.Ramsay SE, Whincup PH, Shaper AG, Wannamethee SG. The relations of body composition and adiposity measures to ill health and physical disability in elderly men. Am J Epidemiol. 2006;164:459–69. doi: 10.1093/aje/kwj217. [DOI] [PubMed] [Google Scholar]
- 42.Patla AE, Shumway-Cook A. Dimensions of mobility: Defining the complexity and difficulty associated with community mobility. J Aging Phys Act. 1999;7:7–19. [Google Scholar]
- 43.Hirvensalo M, Rantanen T, Heikkinen E. Mobility difficulties and physical activity as predictors of mortality and loss of independence in the community-living older population. J Am Geriatr Soc. 2000;48:493–8. doi: 10.1111/j.1532-5415.2000.tb04994.x. [DOI] [PubMed] [Google Scholar]
- 44.Guralnik JM, Ferrucci L, Pieper CF, Leveille SG, Markides KS, Ostir GV, et al. Lower extremity function and subsequent disability: Consistency across studies, predictive models, and value of gait speed alone compared with the short physical performance battery. J Gerontol A Biol Sci Med Sci. 2000;55:M221–31. doi: 10.1093/gerona/55.4.m221. [DOI] [PubMed] [Google Scholar]
- 45.Beswick AD, Rees K, Dieppe P, Ayis S, Gooberman-Hill R, Horwood J, et al. Complex interventions to improve physical function and maintain independent living in elderly people: A systematic review and meta-analysis. Lancet. 2008;371:725–35. doi: 10.1016/S0140-6736(08)60342-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Tooth L, Russell A, Lucke J, Byrne G, Lee C, Wilson A, et al. Impact of cognitive and physical impairment on carer burden and quality of life. Qual Life Res. 2008;17:267–73. doi: 10.1007/s11136-007-9300-7. [DOI] [PubMed] [Google Scholar]
- 47.Warburton DE, Gledhill N, Quinney A. Musculoskeletal fitness and health. Can J Appl Physiol. 2001;26:217–37. doi: 10.1139/h01-013. [DOI] [PubMed] [Google Scholar]
- 48.Clausen T, Wilson AO, Molebatsi RM, Holmboe-Ottesen G. Diminished mental-and physical function and lack of social support are associated with shorter survival in community dwelling older persons of Botswana. BMC Public Health. 2007;7:144. doi: 10.1186/1471-2458-7-144. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Inouye SK, Peduzzi PN, Robison JT, Hughes JS, Horwitz RI, Concato J. Importance of functional measures in predicting mortality among older hospitalized patients. JAMA. 1998;279:1187–93. doi: 10.1001/jama.279.15.1187. [DOI] [PubMed] [Google Scholar]
- 50.Liu-Ambrose T, Ashe MC, Marra C Conditions Research Team PA. Among older adults with multiple chronic conditions, physical activity is independently and inversely associated with health care utilization. Br J Sports Med. 2008;44:1024–8. doi: 10.1136/bjsm.2008.046458. [DOI] [PubMed] [Google Scholar]
- 51.Mathieson KM, Kronenfeld JJ, Keith VM. Maintaining functional independence in elderly adults: The roles of health status and financial resources in predicting home modifications and use of mobility equipment. Gerontologist. 2002;42:24–31. doi: 10.1093/geront/42.1.24. [DOI] [PubMed] [Google Scholar]
- 52.WHO Regional Office for Europe. Regional Office for Europe: A Physically Active Life Through Everyday Transport. 2002. [Last accessed on 2015 Apr 16]. Available from: http://www.euro.who.int/document/e75662.pdf .
- 53.Frank LD, Greenwald MJ, Winkelman S, Chapman J, Kavage S. Carbonless footprints: Promoting health and climate stabilization through active transportation. Prev Med. 2010;50:S99–105. doi: 10.1016/j.ypmed.2009.09.025. [DOI] [PubMed] [Google Scholar]
- 54.Shumway-Cook A, Patla AE, Stewart A, Ferrucci L, Ciol MA, Guralnik JM. Environmental demands associated with community mobility in older adults with and without mobility disabilities. Phys Ther. 2002;82:670–81. [PubMed] [Google Scholar]
- 55.Sauermann S, Standhardt H, Gerschlager W, Lanmüller H, Alesch F. Kinematic evaluation in Parkinson's disease using a hand-held position transducer and computerized signal analysis. Acta Neurochir (Wien) 2005;147:939–45. doi: 10.1007/s00701-005-0569-4. [DOI] [PubMed] [Google Scholar]
- 56.Verbrugge LM, Jette AM. The disablement process. Soc Sci Med. 1994;38:1–14. doi: 10.1016/0277-9536(94)90294-1. [DOI] [PubMed] [Google Scholar]
- 57.Lawton MP, editor, editors. Environment and Aging. 2nd ed. Monterey: Brooks/Cole; 1986. [Google Scholar]
- 58.Law M. 1991 Muriel Driver lecture.The environment: A focus for occupational therapy. Can J Occup Ther. 1991;58:171–80. doi: 10.1177/000841749105800404. [DOI] [PubMed] [Google Scholar]
- 59.Murata C, Kondo T, Tamakoshi K, Yatsuya H, Toyoshima H. Factors associated with life space among community-living rural elders in Japan. Public Health Nurs. 2006;23:324–31. doi: 10.1111/j.1525-1446.2006.00568.x. [DOI] [PubMed] [Google Scholar]
- 60.Xue QL, Fried LP, Glass TA, Laffan A, Chaves PH. Life-space constriction, development of frailty, and the competing risk of mortality: The Women's Health And Aging Study I. Am J Epidemiol. 2008;167:240–8. doi: 10.1093/aje/kwm270. [DOI] [PubMed] [Google Scholar]
- 61.Glass TA, Balfour JL. Neighborhoods, aging, and functional limitations. In: Kawachi I, Berkman LF, editors. Neighborhoods and Health. New York: Oxford University Press; 2003. pp. 303–34. [Google Scholar]
- 62.Davison KK, Lawson CT. Do attributes in the physical environment influence children's physical activity. A review of the literature? Int J Behav Nutr Phys Act. 2006;3:19. doi: 10.1186/1479-5868-3-19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Carp FM. Neighborhood quality perception and measurement. In: Newcomer RJ, Lawton P, Byerts TO, editors. Housing an Aging Society: Issues Alternatives, and Policy. New York: Van Nostrand Reinhold Company; 1986. pp. 127–40. [Google Scholar]
- 64.International Classification of Functioning, Disability and Health. Geneva, Switzerland: WHO; 2001. World Health Organization, editor. [Google Scholar]
- 65.Albrecht GL, Devlieger PJ. The disability paradox: High quality of life against all odds. Soc Sci Med. 1999;48:977–88. doi: 10.1016/s0277-9536(98)00411-0. [DOI] [PubMed] [Google Scholar]
- 66.Richards JS, Bombardier CH, Tate D, Dijkers M, Gordon W, Shewchuk R, et al. Access to the environment and life satisfaction after spinal cord injury. Arch Phys Med Rehabil. 1999;80:1501–6. doi: 10.1016/s0003-9993(99)90264-2. [DOI] [PubMed] [Google Scholar]
- 67.Verbrugge LM, Rennert C, Madans JH. The great efficacy of personal and equipment assistance in reducing disability. Am J Public Health. 1997;87:384–92. doi: 10.2105/ajph.87.3.384. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Vik K, Lilja M, Nygård L. The influence of the environment on participation subsequent to rehabilitation as experienced by elderly people in Norway. Scand J Occup Ther. 2007;14:86–95. doi: 10.1080/11038120600971047. [DOI] [PubMed] [Google Scholar]
- 69.Horowitz BP. Occupational therapy home assessments: Supporting community living through client-centered practice. Occup Ther Ment Health. 2002;18:1–17. [Google Scholar]
- 70.Walker RB, Hiller JE. Places and health: A qualitative study to explore how older women living alone perceive the social and physical dimensions of their neighbourhoods. Soc Sci Med. 2007;65:1154–65. doi: 10.1016/j.socscimed.2007.04.031. [DOI] [PubMed] [Google Scholar]
- 71.Baum F, Palmer C. Opportunity structures: Urban landscape, social capital and health promotion in Australia. Health Promot Int. 2002;17:351–61. doi: 10.1093/heapro/17.4.351. [DOI] [PubMed] [Google Scholar]
- 72.Bowling A, Stafford M. How do objective and subjective assessments of neighbourhood influence social and physical functioning in older age. Findings from a British survey of ageing? Soc Sci Med. 2007;64:2533–49. doi: 10.1016/j.socscimed.2007.03.009. [DOI] [PubMed] [Google Scholar]
- 73.Burke J, O’Campo P, Salmon C, Walker R. Pathways connecting neighborhood influences and mental well-being: Socioeconomic position and gender differences. Soc Sci Med. 2009;68:1294–304. doi: 10.1016/j.socscimed.2009.01.015. [DOI] [PubMed] [Google Scholar]
- 74.Lindström M, Moghaddassi M, Merlo J. Individual self-reported health, social participation and neighbourhood: A multilevel analysis in Malmö, Sweden. Prev Med. 2004;39:135–41. doi: 10.1016/j.ypmed.2004.01.011. [DOI] [PubMed] [Google Scholar]
- 75.Clarke P, Ailshire JA, Lantz P. Urban built environments and trajectories of mobility disability: Findings from a national sample of community-dwelling American adults (1986-2001) Soc Sci Med. 2009;69:964–70. doi: 10.1016/j.socscimed.2009.06.041. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Brown SC, Mason CA, Perrino T, Lombard JL, Martinez F, Plater-Zyberk E, et al. Built environment and physical functioning in Hispanic elders: The role of “eyes on the street”. Environ Health Perspect. 2008;116:1300–7. doi: 10.1289/ehp.11160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Frank LD, Andresen MA, Schmid TL. Obesity relationships with community design, physical activity, and time spent in cars. Am J Prev Med. 2004;27:87–96. doi: 10.1016/j.amepre.2004.04.011. [DOI] [PubMed] [Google Scholar]
- 78.Examining the Evidence Report No. 282. Washington, DC: National Academy of Sciences; 2005. Institute of Medicine and Transportation Research Board of the National Academies. Does the Built Environment Influence Physical Activity? [Google Scholar]
- 79.Leyden KM. Social capital and the built environment: The importance of walkable neighborhoods. Am J Public Health. 2003;93:1546–51. doi: 10.2105/ajph.93.9.1546. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Jacobs J. The Death and Life of Great American Cities. New York: Vintage Books, Repr 1992; 1961. [Google Scholar]
- 81.Barton H, Grant M. A health map for the local human habitat. J R Soc Promot Health. 2006;126:252–3. doi: 10.1177/1466424006070466. [DOI] [PubMed] [Google Scholar]
- 82.Shumway-Cook A, Patla A, Stewart AL, Ferrucci L, Ciol MA, Guralnik JM. Assessing environmentally determined mobility disability: Self-report versus observed community mobility. J Am Geriatr Soc. 2005;53:700–4. doi: 10.1111/j.1532-5415.2005.53222.x. [DOI] [PubMed] [Google Scholar]
- 83.Field MJ, Jette AM. Definition and monitoring of disability. In: Jette IM, editor. The Future of Disability in America. Washington, DC: The National Academies Press; 2007. pp. 35–64. [Google Scholar]
- 84.Arksey H, O’Malley L. Scoping studies: Towards a methodological framework. Int J Soc Res Methodol. 2005;8:19–32. [Google Scholar]
- 85.Levack WM. Ethics in goal planning for rehabilitation: A utilitarian perspective. Clin Rehabil. 2009;23:345–51. doi: 10.1177/0269215509103286. [DOI] [PubMed] [Google Scholar]
- 86.Colquhoun HL, Letts LJ, Law MC, MacDermid JC, Missiuna CA. A scoping review of the use of theory in studies of knowledge translation. Can J Occup Ther. 2010;77:270–9. doi: 10.2182/cjot.2010.77.5.3. [DOI] [PubMed] [Google Scholar]
- 87.Anderson S, Allen P, Peckham S, Goodwin N. Asking the right questions: Scoping studies in the commissioning of research on the organisation and delivery of health services. Health Res Policy Syst. 2008;6:7. doi: 10.1186/1478-4505-6-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Parry D, Salsberg J, Macaulay A. A Guide to Researcher and Knowledge-User Collaboration in Health Research. Canadian Institute of Health Research. 2006. [Accessed April 16, 2015]. Available from: http://www.cihr-irsc.gc.ca/e/documents/Guide_to_Researcher_and_KU_Collaboration.pdf .
- 89.Fougeyrollas P, Cloutier R, Bergeron H, Côté J, St-Michel G, editors. The Quebec Classification: Disability Creation Process. Lac St-Charles, Quebec, Canada: International Network on the Disability Creation Process; Canadian Society for the International Classification of Impairments, Disabilities and Handicaps. 1998 [Google Scholar]
- 90.Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009;6:e1000097. doi: 10.1371/journal.pmed.1000097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.L’Écuyer R. Méthodologie de L’analyse Développementale de Contenu: Méthode GPS et Concept de soi [Methodology of Developmental Content Analysis: GPS Method and Self Concept. Quéec, QC: Presses de l’Université du Québec; 1990. [Google Scholar]
- 92.Taylor M. In: Public Policy in the Community. 2nd ed. Hambleton CF, editor. New York, NY: Palgrave Macmillan; 2011. p. 265. [Google Scholar]
- 93.Denis JL, Lomas J. Convergent evolution: The academic and policy roots of collaborative research. J Health Serv Res Policy. 2003;8(Suppl 2):1–6. doi: 10.1258/135581903322405108. [DOI] [PubMed] [Google Scholar]
- 94.D’Amour D, Oandasan I. Interprofessionality as the field of interprofessional practice and interprofessional education: An emerging concept. J Interprof Care. 2005;19(Suppl 1):8–20. doi: 10.1080/13561820500081604. [DOI] [PubMed] [Google Scholar]
- 95.Popay J. Incorporing Qualitative Information in Systematic Reviews. Paper Presented at the 14th Cochrane Colloquium, Dunlin, Ireland. 2006 [Google Scholar]