

Abstract
In the early 2000s, the prevalence of diabetes in adults aged ≥30 years in Korea was about 9% to 10%, and it remained stable. However, a nationwide survey showed that this prevalence increased over the past few years. After age-standardization using the Korean population of the year 2010, the prevalence of diabetes in adults aged ≥30 years was 10.0% to 10.8% between 2001 and 2012, which increased to 12.5% in 2013 and 11.6% in 2014. During that period, there have been changes in the gender- and age-specific prevalence of diabetes in Korean adults. The prevalence of diabetes in the elderly population increased significantly, while this prevalence in young adults, especially in young women, did not change significantly. The contribution of each diabetic risk factor, such as obesity, β-cell dysfunction, sarcopenia, and socioeconomic status, in developing diabetes has also changed during that period in each gender and age group. For young women, obesity was the most important risk factor; by contrast, for elderly diabetic patients, sarcopenia was more important than obesity as a risk factor. Considering the economic burden of diabetes and its associated comorbidities, a public health policy targeting the major risk factors in each population might be more effective in preventing diabetes.
Keywords: Diabetes mellitus, Korea, Obesity, Prevalence, Sarcopenia
INTRODUCTION
The International Diabetes Federation estimated the global prevalence of diabetes to be 151 million in 2000 [1] and 285 million in 2010 [2]. This prevalence is expected to rise to 552 million by 2030 [3]. In Korea, after a rapid increment of the prevalence of diabetes during the last 30 years, the prevalence of diabetes in adults aged ≥30 years reached about 9% to 10% and remained stable between 2000 and 2010 [4,5]. A recent Korea National Health and Nutritional Examination Survey (KNHANES) 2011 to 2014 showed that the prevalence of diabetes in adults aged ≥30 years increased to 10% to 11% [6]. During that period, along with the trend of an increasing number of elderly people in Korea [7], the number of elderly patients with type 2 diabetes mellitus (T2DM) increased significantly [8,9]. In addition, the gender disparity in the trend of the prevalence of diabetes and obesity was apparent in the 2000s [9,10]. In this review, we summarized the recent trends in the prevalence of diabetes in Korea, and the risk factors associated with those trends will be discussed.
THE PREVALENCE OF DIABETES
The prevalence of diabetes in Korean adults aged ≥30 years remained stable at approximately 9% to 10% between 2000 and 2010 [4,5]. The Korean Centers for Disease Control and Prevention reported that it increased to 10% to 11% between 2011 and 2014 [6]. If cases of diabetes mellitus (DM) were defined as subjects who were users of antidiabetic medication, including insulin, at the point of the survey or had 8-hour fasting plasma glucose levels ≥126 mg/dL, the age-standardized prevalence of diabetes using the Korean population in the year 2010 was 10.0% to 10.8% in adults aged ≥30 years during 2001 to 2012, which increased to 12.5% in 2013 and 11.6% in 2014 (Fig. 1A). In men, age-standardized prevalence in 2013 and 2014 was 13.7% and 13.1% respectively; in women, that was 11.5% and 10.3%, respectively (Fig. 1A). The age-standardized prevalence in subjects 30 to 59 years old did not change much between 2005 and 2014: 8.3% to 10.2% in men and 4.3% to 5.9% in women (Fig. 1B). By contrast, the elderly population aged ≥60 years showed an increasing trend of diabetes prevalence from 19.0% in 2001 to 21.4% in 2010 and to 24.7% in 2014 (Fig. 1B).
Fig. 1. The age-standardized prevalence of diabetes in adults aged ≥30 years from the Korean National Health and Nutrition Examination Survey 2001 to 2014. Age standardization was done using the Korean population in the year 2010. Cases of diabetes mellitus were defined as subjects who were users of antidiabetic medication, including insulin, at the point of the survey or had 8-hour fasting plasma glucose levels ≥126 mg/dL. (A) The overall prevalence of diabetes mellitus in adults aged ≥30 years was shown according to gender. The prevalence in men and women was presented by a circle and square with a standardized error bar, respectively. (B) The prevalence of diabetes mellitus in adults aged 30 to 59 years and ≥60 years was presented with black and gray bars, respectively.

Since 2011, all adult participants in the KNHANES had their glycosylated hemoglobin (HbA1c) level measured following the guidelines of the Korean Diabetes Association, which adopted an HbA1c ≥6.5% as a diagnostic criterion for DM since 2011 [11]. Considering that in the previous KNHANES, only participants who had a medical history of diabetes measured their HbA1c level, a trend in the prevalence of diabetes estimated from the KNHANES should be interpreted with caution. After adopting an HbA1c ≥6.5% as one of the diagnostic criteria of diabetes, the prevalence of diabetes was increased 2.2% to 2.4% (Fig. 2) as previously reported [12]; the age-standardized prevalence of diabetes in adults aged ≥30 years reached 13.2%, 12.3%, 15.6%, and 13.8% in 2011, 2012, 2013, and 2014, respectively (Fig. 2).
Fig. 2. The age-standardized prevalence of diabetes in adults aged (A) ≥30 years and (B) 30 to 59 years from the Korean National Health and Nutrition Examination Survey 2010 to 2014 using different diagnostic criteria. Cases of diabetes mellitus were defined as subjects who were users of antidiabetic medication, including insulin, at the point of the survey or had 8-hour fasting plasma glucose levels ≥126 mg/dL (criteria I, solid line). After adopting an glycosylated hemoglobin ≥6.5% as one of diagnostic criteria of diabetes (criteria II, dashed line), the prevalence of diabetes was increased 2.2% to 2.4%.

Nationwide claim data showed that the peak incidence of T2DM between 2008 and 2010 was observed at 60 to 79 years of age (i.e., 23 to 25/1,000 person-year [PY]) both in men and women (Fig. 3) [8]. In men, the incidence of diabetes in individuals 50 to 59 years old and 80 to 89 years old was next (18/1,000 PY). In the case of women, the incidence of diabetes in individuals 80 to 89 years of age was next (17/1,000 PY). Women aged 50 to 59 years old showed a relatively lower incidence of diabetes than men of the same age (13/1,000 PY vs. 19/1,000 PY) [8].
Fig. 3. The incidence of type 2 diabetes mellitus in the Korean population by age group from the National Health Insurance database. PY, person-year.

Korea is one of the most rapidly aging countries; the proportion of the elderly population aged ≥65 years reached 11.0% in 2010 and is expected to be 22% in 2020 [7]. The increasing size of the elderly population might result in the nationwide increasing prevalence of diabetes. Considering that the increasing prevalence of diabetes may also increase the economic burden, a public strategy targeting elderly people for diabetes prevention is urgent.
In the case of the younger population, a nationwide health survey showed a relatively stable prevalence of diabetes, especially in women [9]. These results corresponded with the nationwide survey in Japan [13] but were not observed in China [14]. However, considering that only 50% to 60% of young diabetic patients aged 30 to 40 years have insight to have diabetes in Korea [15,16], and undiagnosed diabetic patients showed a significantly higher risk of cardiovascular disease compared to diagnosed diabetic patients [15], a public heath strategy targeting the younger population for diabetes screening might be needed.
TRENDS IN RISK FACTORS FOR DEVELOPING DIABETES
Obesity
In Korea, the prevalence of obesity and abdominal obesity in the general population has increased from 2005 to 2007; it has remained steady since then [17]. However, in the cases of young women, body mass index (BMI) and waist circumference have significantly decreased during the 2000s in the general population [9,10]. By contrast, in the cases of women with diabetes of the same age, the prevalence of abdominal obesity increased from 66.3% to 72.9% during the same period [18]. Along with this trend, abdominal obesity is the single most important independent risk factor for diabetes in young Korean women [18]. It was associated with more than four times a higher risk of diabetes in 2010 even after an adjustment for age, dyslipidemia, family history, and exercise. The fact that abdominal obesity is the most important risk factor of diabetes in women was in agreement with a large cohort study conducted in the United States on young women during 16 years of follow-up [19]. Attributing the power of obesity or abdominal obesity for developing diabetes was more prominent at a young age compared to the elderly population in Korean women [18], as well as in Japanese women [20].
In terms of men, there might be a difference in the contribution of obesity in the development of diabetes compared to women. For the last 10 years, BMI was significantly increased in young men [9,10]. However, there has not been much change in the prevalence of diabetes in young Korean men [9]. Furthermore, in them, the association between obesity and diabetes has been attenuated [18]. In the early 2000s, the prevalence of abdominal obesity in subjects with diabetes was about two times higher than that in nondiabetic subjects; however, there was no difference in the prevalence of abdominal obesity between subjects with and without diabetes in 2010 [18]. Instead, the association between a family history of diabetes and DM in these subjects was much stronger in the late 2000s [18].
β-Cell function
The main pathogenic mechanism in developing T2DM in obesity or aging is insulin resistance; however, more than 70% of obese or elderly people are free of diabetes [5,17,21]. Recently, a 10-year follow-up cohort study showed that insulin sensitivity was significantly decreased with aging, regardless of the glucose tolerance state at the follow-up [22]. However, compared with participants who remained normal glucose tolerance (NGT), those who progressed to diabetes had a lower β-cell function [22], which agreed with previous reports in Japan [23] and a multiethnic population [24]. They have suggested that impaired β-cell function might be the determining factor whether or not T2DM develops or the condition of insulin resistance increased.
The main determinants of β-cell function in T2DM is genetic factor associated with the insulin secretion capacity and the proliferation and regeneration of β-cells [25]. A long-term cohort study in Korea also confirmed that a genetic variant near the glucokinase gene was significantly associated with the progression to diabetes [22].
In terms of age of onset, β-cell dysfunction might be more important in people with early-onset diabetes compared to elderly-onset diabetic patients [26], which was also reproduced in Korea [27]. Among people with recent-onset diabetes from the KNHANES, defined as those who have diabetes for <5 years, there was an inverse correlation between age and the homeostasis model assessment of β-cell function (Fig. 4). In addition, young diabetic patients were more influenced by a family history of diabetes compared to elderly patients [18], which was in agreement with Caucasians [28]. That association was more prominent in men. In young men, a family history of diabetes was associated with more than six times a higher risk of diabetes [18]. In the case of women of the same age, however, the presence of obesity but not family history was the most important determinant of diabetes status [18].
Fig. 4. The level of (A) insulin secretion capacity and (B) insulin resistance according to the age of patients with recent-onset diabetes from the Korean National Health and Nutrition Examination Survey 2008 to 2010. Recent-onset diabetes patients were defined as those who have had diabetes for <5 years. HOMA-β, the homeostasis model assessment of β-cell function; HOMA-IR, the homeostasis model assessment of insulin resistance; DM, diabetes mellitus.

Sarcopenia
A decrease in the insulin sensitivity with the aging is well known, even in individuals who remained as NGT at 10 years [22], which can be partially explained by decreased muscle mass (i.e., sarcopenia, along with increased fat mass). The KNHANES 2008 to 2010 showed that for elderly-onset diabetic patients, insulin resistance was more prominent compared to middle-age-onset patients at the time of diagnosis [27]. Although insulin resistance was higher in the elderly-onset diabetic patients compared to the middle-age-onset patients, the BMI, waist circumference, and body fat mass of the elderly-onset subjects were not different across the age group, which was in agreement with the Chinese population [29]. In a cross-sectional study comparing Caucasian and Chinese patients with recent-onset diabetes (duration <2 years), a negative correlation between the age at diagnosis and BMI or insulin resistance was only observed in Caucasians. In Chinese diabetic patients, there was no relationship between age at diagnosis and BMI, insulin resistance, or triglyceride level [29].
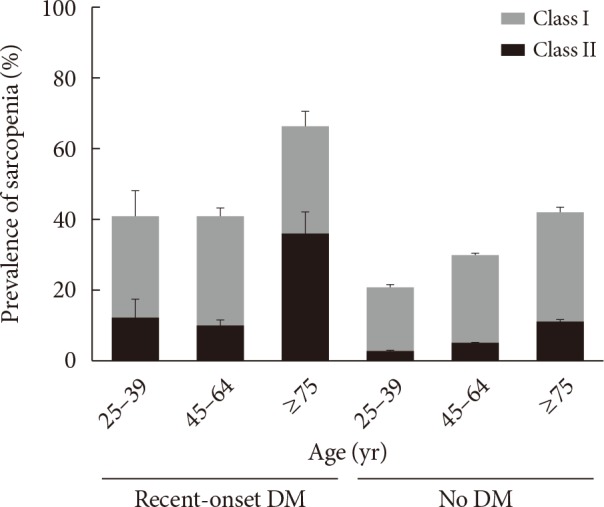
Instead, a Korean nationwide survey showed that elderly-onset diabetic patients had significantly lower skeletal muscle mass and higher prevalence of sarcopenia compared with the middle-age-onset group [27]. Comparing the elderly-onset diabetic patients with the age-matched NGT subjects (although there was no difference in the sarcopenia class I prevalence) (milder form of sarcopenia; 1 to 2 standard deviations below the gender-specific mean for healthy young adults), the advanced stage of sarcopenia (>2 standard deviations below the gender-specific mean for healthy young adults; classified as class II) was found about three times more frequently in those with recent-onset diabetes compared with nondiabetic subjects (Fig. 5).
Fig. 5. The prevalence of sarcopenia (class I+class II) in subjects with recent-onset diabetes and without diabetes. Sarcopenia was classified as class I or class II, defined as appendicular skeletal muscle mass/weight 1 to 2 or >2 standard deviations, respectively, below the gender-specific mean for healthy young adults. The entire prevalence of sarcopenia in each age group was separated by gray and black bars which represent the prevalence of sarcopenia class I and II, respectively. DM, diabetes mellitus.
Socioeconomic status
Low socioeconomic status (SES) is a well-documented risk factor of diabetes in developed countries [30,31]. Korea is one of the most rapidly developing countries in the world [32]; low SES has been an emerging risk factor for DM in recent years [33,34,35]. Both low income status and low education level were significantly associated with the risk of diabetes in the KNHANES 2008 to 2012 even after an adjustment for other risk factors (i.e., obesity and dyslipidemia) [33,34], which was not observed in 2001 or 2005 [33]. In other Asian countries, such as India and China, the same tendency was also observed [36,37]. In addition, the association between SES and diabetes was prominent in people less than 65 years old [33,35].
Poorer and less educated people have fewer opportunities for primary prevention, early diagnosis, and appropriate management [38]; however, these disadvantages can be overcome [31,39]. Low SES is also associated with a high prevalence of obesity [33,37]. The reduction of obesity in populations with a lower SES has proven to be successful for preventing diabetes in India [37], which might be another possible strategy for reducing health inequality according to SES.
CONCLUSIONS
In the 2000s, despite a steady state of the overall prevalence of diabetes, there have been changes in the gender-, age-, and SES-specific prevalence in Korean adults. A nationwide survey showed that there was a difference in major determining risk factors of diabetes according to each gender and age group. Considering the economic burden of diabetes and its associated comorbidities, a public health policy targeting major risk factors in each population (i.e., obesity in women or sarcopenia in older people) might be more effective in preventing diabetes at the national level.
Footnotes
CONFLICTS OF INTEREST: No potential conflict of interest relevant to this article was reported.
References
- 1.International Diabetes Federation. Diabetes atlas. Brussels: International Diabetes Federation; 2000. [Google Scholar]
- 2.International Diabetes Federation. IDF diabetes atlas. 4th ed. Brussels: International Diabetes Federation; 2009. [Google Scholar]
- 3.Whiting DR, Guariguata L, Weil C, Shaw J. IDF diabetes atlas: global estimates of the prevalence of diabetes for 2011 and 2030. Diabetes Res Clin Pract. 2011;94:311–321. doi: 10.1016/j.diabres.2011.10.029. [DOI] [PubMed] [Google Scholar]
- 4.Kim DJ. The epidemiology of diabetes in Korea. Diabetes Metab J. 2011;35:303–308. doi: 10.4093/dmj.2011.35.4.303. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Choi YJ, Kim HC, Kim HM, Park SW, Kim J, Kim DJ. Prevalence and management of diabetes in Korean adults: Korea National Health and Nutrition Examination Surveys 1998-2005. Diabetes Care. 2009;32:2016–2020. doi: 10.2337/dc08-2228. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Korean Centers for Disease Control and Prevention. Korea health statistics 2014: Korea National Health and Nutrition Examination Survey (KNHANES VI-2) Cheongju: Korean Centers for Disease Control and Prevention; 2015. [Google Scholar]
- 7.Statistics Korea. Population projections for Korea: 2010-2040. Daejeon: Statistics Korea; 2011. [Google Scholar]
- 8.Koo BK, Lee CH, Yang BR, Hwang SS, Choi NK. The incidence and prevalence of diabetes mellitus and related atherosclerotic complications in Korea: a National Health Insurance Database Study. PLoS One. 2014;9:e110650. doi: 10.1371/journal.pone.0110650. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Koo BK, Kim EK, Choi H, Park KS, Moon MK. Decreasing trends of the prevalence of diabetes and obesity in Korean women aged 30-59 years over the past decade: results from the Korean National Health and Nutrition Examination Survey, 2001-2010. Diabetes Care. 2013;36:e95–e96. doi: 10.2337/dc13-0247. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Rhee SY, Park SW, Kim DJ, Woo J. Gender disparity in the secular trends for obesity prevalence in Korea: analyses based on the KNHANES 1998-2009. Korean J Intern Med. 2013;28:29–34. doi: 10.3904/kjim.2013.28.1.29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Korean Diabetes Association. Treatment guideline for diabetes. Seoul: Korean Diabetes Association; 2011. [Google Scholar]
- 12.Jeon JY, Ko SH, Kwon HS, Kim NH, Kim JH, Kim CS, Song KH, Won JC, Lim S, Choi SH, Jang MJ, Kim Y, Oh K, Kim DJ, Cha BY Taskforce Team of Diabetes Fact Sheet of the Korean Diabetes Association. Prevalence of diabetes and prediabetes according to fasting plasma glucose and HbA1c. Diabetes Metab J. 2013;37:349–357. doi: 10.4093/dmj.2013.37.5.349. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Charvat H, Goto A, Goto M, Inoue M, Heianza Y, Arase Y, Sone H, Nakagami T, Song X, Qiao Q, Tuomilehto J, Tsugane S, Noda M, Inoue M. Impact of population aging on trends in diabetes prevalence: a meta-regression analysis of 160,000 Japanese adults. J Diabetes Investig. 2015;6:533–542. doi: 10.1111/jdi.12333. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Xi B, Liang Y, He T, Reilly KH, Hu Y, Wang Q, Yan Y, Mi J. Secular trends in the prevalence of general and abdominal obesity among Chinese adults, 1993-2009. Obes Rev. 2012;13:287–296. doi: 10.1111/j.1467-789X.2011.00944.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Lee YH, Armstrong EJ, Kim G, Oh J, Kang SM, Lee BW, Ahn CW, Cha BS, Lee HC, Mantzoros CS, Kang ES. Undiagnosed diabetes is prevalent in younger adults and associated with a higher risk cardiometabolic profile compared to diagnosed diabetes. Am Heart J. 2015;170:760–769.e2. doi: 10.1016/j.ahj.2015.07.024. [DOI] [PubMed] [Google Scholar]
- 16.Korean Diabetes Association. Korea Centers for Disease Control and Prevention: Diabetes fact sheet in Korea 2012. [updated 2012 Nov 13]. Available from: http://www.diabetes.or.kr/temp/Diabetes_Fact_sheet2012.pdf.
- 17.Kim CS, Ko SH, Kwon HS, Kim NH, Kim JH, Lim S, Choi SH, Song KH, Won JC, Kim DJ, Cha BY Taskforce Team of Diabetes Fact Sheet of the Korean Diabetes Association. Prevalence, awareness, and management of obesity in Korea: data from the Korea national health and nutrition examination survey (1998-2011) Diabetes Metab J. 2014;38:35–43. doi: 10.4093/dmj.2014.38.1.35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Koo BK, Kim SW, Yi KH, Park KS, Moon MK. Changing relative contribution of abdominal obesity and a family history of diabetes on prevalence of diabetes mellitus in Korean men and women aged 30-49 years from 2001 to 2010. J Diabetes. 2015;7:465–472. doi: 10.1111/1753-0407.12202. [DOI] [PubMed] [Google Scholar]
- 19.Hu FB, Manson JE, Stampfer MJ, Colditz G, Liu S, Solomon CG, Willett WC. Diet, lifestyle, and the risk of type 2 diabetes mellitus in women. N Engl J Med. 2001;345:790–797. doi: 10.1056/NEJMoa010492. [DOI] [PubMed] [Google Scholar]
- 20.Tatsumi Y, Ohno Y, Morimoto A, Nishigaki Y, Mizuno S, Watanabe S. Age differences in the risk of diabetes incidence according to body mass index level in Japanese women. Obes Res Clin Pract. 2013;7:e455–e463. doi: 10.1016/j.orcp.2012.05.001. [DOI] [PubMed] [Google Scholar]
- 21.Meigs JB, Wilson PW, Fox CS, Vasan RS, Nathan DM, Sullivan LM, D'Agostino RB. Body mass index, metabolic syndrome, and risk of type 2 diabetes or cardiovascular disease. J Clin Endocrinol Metab. 2006;91:2906–2912. doi: 10.1210/jc.2006-0594. [DOI] [PubMed] [Google Scholar]
- 22.Ohn JH, Kwak SH, Cho YM, Lim S, Jang HC, Park KS, Cho NH. 10-Year trajectory of beta-cell function and insulin sensitivity in the development of type 2 diabetes: a community-based prospective cohort study. Lancet Diabetes Endocrinol. 2016;4:27–34. doi: 10.1016/S2213-8587(15)00336-8. [DOI] [PubMed] [Google Scholar]
- 23.Morimoto A, Tatsumi Y, Deura K, Mizuno S, Ohno Y, Miyamatsu N, Watanabe S. Impact of impaired insulin secretion and insulin resistance on the incidence of type 2 diabetes mellitus in a Japanese population: the Saku study. Diabetologia. 2013;56:1671–1679. doi: 10.1007/s00125-013-2932-y. [DOI] [PubMed] [Google Scholar]
- 24.Festa A, Williams K, D'Agostino R, Jr, Wagenknecht LE, Haffner SM. The natural course of beta-cell function in nondiabetic and diabetic individuals: the Insulin Resistance Atherosclerosis Study. Diabetes. 2006;55:1114–1120. doi: 10.2337/diabetes.55.04.06.db05-1100. [DOI] [PubMed] [Google Scholar]
- 25.Park KS. The search for genetic risk factors of type 2 diabetes mellitus. Diabetes Metab J. 2011;35:12–22. doi: 10.4093/dmj.2011.35.1.12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Mohan V, Amutha A, Ranjani H, Unnikrishnan R, Datta M, Anjana RM, Staimez L, Ali MK, Narayan KM. Associations of beta-cell function and insulin resistance with youth-onset type 2 diabetes and prediabetes among Asian Indians. Diabetes Technol Ther. 2013;15:315–322. doi: 10.1089/dia.2012.0259. [DOI] [PubMed] [Google Scholar]
- 27.Koo BK, Roh E, Yang YS, Moon MK. Difference between old and young adults in contribution of beta-cell function and sarcopenia in developing diabetes mellitus. J Diabetes Investig. 2016;7:233–240. doi: 10.1111/jdi.12392. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.de Miguel-Yanes JM, Shrader P, Pencina MJ, Fox CS, Manning AK, Grant RW, Dupuis J, Florez JC, D'Agostino RB, Sr, Cupples LA, Meigs JB MAGIC Investigators; DIAGRAM+ Investigators. Genetic risk reclassification for type 2 diabetes by age below or above 50 years using 40 type 2 diabetes risk single nucleotide polymorphisms. Diabetes Care. 2011;34:121–125. doi: 10.2337/dc10-1265. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Wong J, Molyneaux L, Zhao D, Constantino M, Gray RS, Twigg SM, Xu ZR, Yue DK. Different accelerators to early-onset type 2 diabetes: a comparison of Anglo-Celtic and Chinese patients. J Diabetes Complications. 2008;22:389–394. doi: 10.1016/j.jdiacomp.2007.04.003. [DOI] [PubMed] [Google Scholar]
- 30.Robbins JM, Vaccarino V, Zhang H, Kasl SV. Socioeconomic status and type 2 diabetes in African American and non-Hispanic white women and men: evidence from the Third National Health and Nutrition Examination Survey. Am J Public Health. 2001;91:76–83. doi: 10.2105/ajph.91.1.76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Rabi DM, Edwards AL, Southern DA, Svenson LW, Sargious PM, Norton P, Larsen ET, Ghali WA. Association of socio-economic status with diabetes prevalence and utilization of diabetes care services. BMC Health Serv Res. 2006;6:124. doi: 10.1186/1472-6963-6-124. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Kim SH. International statistics yearbook. Daejeon: Statistics Korea; 2011. [Google Scholar]
- 33.Koo BK, Kim SW, Yi KH, Moon MK. Low economic status is identified as an emerging risk factor for diabetes mellitus in Korean men aged 30 to 59 years in Korean National Health and Nutrition Examination Survey 2008 to 2010. Diabetes Metab J. 2015;39:137–146. doi: 10.4093/dmj.2015.39.2.137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Hwang J, Shon C. Relationship between socioeconomic status and type 2 diabetes: results from Korea National Health and Nutrition Examination Survey (KNHANES) 2010-2012. BMJ Open. 2014;4:e005710. doi: 10.1136/bmjopen-2014-005710. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Kim SR, Han K, Choi JY, Ersek J, Liu J, Jo SJ, Lee KS, Yim HW, Lee WC, Park YG, Lee SH, Park YM. Age- and sex-specific relationships between household income, education, and diabetes mellitus in Korean adults: the Korea National Health and Nutrition Examination Survey, 2008-2010. PLoS One. 2015;10:e0117034. doi: 10.1371/journal.pone.0117034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Ning F, Pang ZC, Dong YH, Gao WG, Nan HR, Wang SJ, Zhang L, Ren J, Tuomilehto J, Hammar N, Malmberg K, Andersson SW, Qiao Q Qingdao Diabetes Survey Group. Risk factors associated with the dramatic increase in the prevalence of diabetes in the adult Chinese population in Qingdao, China. Diabet Med. 2009;26:855–863. doi: 10.1111/j.1464-5491.2009.02791.x. [DOI] [PubMed] [Google Scholar]
- 37.Deepa M, Anjana RM, Manjula D, Narayan KM, Mohan V. Convergence of prevalence rates of diabetes and cardiometabolic risk factors in middle and low income groups in urban India: 10-year follow-up of the Chennai Urban Population Study. J Diabetes Sci Technol. 2011;5:918–927. doi: 10.1177/193229681100500415. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Caiazzo A, Cardano M, Cois E, Costa G, Marinacci C, Spadea T, Vannoni F, Venturini L. Inequalities in health in Italy. Epidemiol Prev. 2004;28(3 Suppl):i–ix. 1–161. [PubMed] [Google Scholar]
- 39.van Lenthe FJ, Schrijvers CT, Droomers M, Joung IM, Louwman MJ, Mackenbach JP. Investigating explanations of socio-economic inequalities in health: the Dutch GLOBE study. Eur J Public Health. 2004;14:63–70. doi: 10.1093/eurpub/14.1.63. [DOI] [PubMed] [Google Scholar]