

Abstract
Web and mobile (mHealth) interventions have promise for improving health outcomes, but engagement and attrition may be reducing effect sizes. Because social networks can improve engagement, which is a key mechanism of action, understanding the structure and potential impact of social networks could be key to improving mHealth effects. This study (a) evaluates social network characteristics of four distinct communication channels (discussion board, chat, e-mail, and blog) in a large social networking intervention, (b) predicts membership in online communities, and (c) evaluates whether community membership impacts engagement. Participants were 299 cancer survivors with significant distress using the 12-week health-space.net intervention. Social networking attributes (e.g., density and clustering) were identified separately for each type of network communication (i.e., discussion board, blog, web mail, and chat). Each channel demonstrated high levels of clustering, and being a community member in one communication channel was associated with being in the same community in each of the other channels (φ = 0.56–0.89, ps < 0.05). Predictors of community membership differed across communication channels, suggesting that each channel reached distinct types of users. Finally, membership in a discussion board, chat, or blog community was strongly associated with time spent engaging with coping skills exercises (Ds = 1.08–1.84, ps < 0.001) and total time of intervention (Ds = 1.13–1.80, ps < 0.001). mHealth interventions that offer multiple channels for communication allow participants to expand the number of individuals with whom they are communicating, create opportunities for communicating with different individuals in distinct channels, and likely enhance overall engagement.
Introduction
As more and more psychological and health-related interventions are being developed for the web and mobile environments, with many of these making explicit use of social networks,1 it has become possible to measure and evaluate the role of the social context as it relates to health in ways that were previously impossible. However, very few studies to date have evaluated the structure of social networks in online interventions or the extent to which different communication channels might influence the development of social networks. These are vital questions given strong associations between social networking, the delivered dose of the intervention,2 and the heterogeneity of ways in which social communication can occur in online interventions (e.g., forums for posting messages to groups, mail-based exchanges between pairs of individuals, real-time chats, and SMS-based communications).
The most commonly used social networking channels include blogs or personal updates,3–5 discussion board forums for posting messages,3,6,7 real-time chat conversations,2,8,9 personal conversations via e-mail or web-based mail features,2 and personal pages.2,3 However, few studies offer more than one social networking channel, and our understanding of how participants engage with these types of social networking features is quite limited. For example, Brindal et al.3 provided an extensive social networking intervention for overweight adults, but measures of use for each channel were limited to the proportion of participants who used each component. The purposes of this study were to address existing gaps in the literature by characterizing social networking across four distinct channels of social communication and better understand how participant characteristics influence the type and nature of social networking within these types of interventions.
Social networking with individuals who share common attributes (e.g., having the same health condition or having undergone similar treatments) has substantial potential to strengthen behavioral interventions given that (a) individuals often report a greater sense of being understood by similar others,10,11 (b) involvement of similar others can improve intervention adherence,12–14 (c) they provide repeated opportunities for social modeling of adaptive skills or strategies,15 (d) they can serve to “normalize” ego-dystonic feelings of distress,16 and (e) most importantly, they may result in improved outcomes relative to individual interventions.11,13 One of the most promising facets of social networking may be its ability to improve social support, and the positive relationship between perceived social support and health outcomes has been widely established.17 With respect to those with a history of cancer, social networking is particularly relevant to behavioral interventions because patients commonly seek out other survivors for companionship, information, and advice.18,19 Recent research suggests that cancer survivors who are more disinclined to use social networks and resources have worse health-related quality of life,20 and those with low social support may be the most likely to turn to the Internet to seek out health information and support.21 In a large sample of the impact of social networking on breast cancer survivors, each additional member in a given person's social network independently predicted higher quality of life.22 Social networking components are likely to motivate those with cancer to participate in online communities23–25 and have been linked with positive health outcomes.26,27
Given the popularity of sites, such as Facebook, there is a high level of user demand for social networking features in eHealth interventions, and understanding how to marry these features with established eHealth intervention components has substantial promise for increasing the efficacy of these kinds of interventions. The development of eHealth interventions is both expensive and time consuming, and understanding how different channels of social networking communications can impact engagement and intervention dose has the potential to maximize the cost-effectiveness of these types of interventions. Because one role of a professional facilitator in this intervention was to encourage communication between participants, we hypothesized that communication channels requiring more extensive professional facilitation (chat and discussion board) would be associated with stronger social networks (i.e., higher density, connectedness, and lower path length) between community participants. Additionally, we sought to evaluate whether participants use available communication channels to develop novel (vs. overlapping) social connections in each of the channels. Given differences in participants' level of familiarity or comfort with different ways of communicating online,28 we hypothesized that social connections in each channel would be relatively distinct. Finally, given previous research demonstrating the importance of “fit” between the intervention and participants' personal needs,28 we also hypothesized that those participants whose needs best matched the format of the intervention (i.e., high distress, significant cancer burden, low social support, and frequent use of technology) would be more likely to be integrated into a strong social networking community within the intervention.
Methods
Participants
Participants (n = 299) were derived from a larger study of the effect of a web-based social networking intervention for cancer survivors experiencing significant distress (health-space.net).2,28 Eligibility criteria included having a previous diagnosis of cancer, reporting distress ≥4 on the Distress Thermometer,29 having reliable access to the Internet, and being willing to complete baseline and followup surveys. Participants were primarily female (77.7 percent), well educated (mean of 15.7 years of education, SD = 2.7), and middle aged (mean age = 53.8 years, SD = 10.8). Most reported having an early stage versus late-stage cancer (75.3 percent vs. 24.7 percent), and a number of cancer types were represented (45.3 percent breast cancer, 13.9 percent prostate cancer, 7.1 percent multiple cancers, 6.1 percent female reproductive cancer, 4.1 percent colorectal cancer, and 23.5 percent others).
Procedure
Participants were randomized to receive immediate or delayed access to a 12-week social networking intervention,2 although the present study included all those with access to the intervention, regardless of randomization condition (i.e., including those participants who were assigned to the wait-list control group and elected to join the social networking intervention after the 12-week waiting period). There were no differences on any observed variables between those assigned to the immediate intervention group and those assigned to receive the intervention after 12 weeks. The health-space intervention included access to a confidential community of other cancer survivor participants and professional facilitators and a structured, 12-week coping skills training intervention. The intervention provided opportunities for participants to interact in four distinct social networking channels: asynchronous discussion board, personal pages and blogs, confidential web-based mail messages, and a real-time, 90-minute weekly chat (Fig. 1). Additional details about each social networking channel and engagement with each of the channels are provided by Owen et al.30 All dyadic interactions between participants (i.e., “actors” in the social networking analysis) were recorded by time stamp and activity on the study server. Participants' identities were held in strict confidence, so participants did not have any opportunity to interact with one another outside the health-space study Web site.
FIG. 1.

Screenshot of the health-space.net. (A) Discussion board and (B) chatroom. Color images available online at www.liebertpub.com/cyber
Measures
Participants completed a detailed self-report questionnaire prior to receiving the health-space intervention and again 12 weeks later. The study used validated measures to assess depression (Center for Epidemiologic Studies Depression Scale [CES-D]; α = 0.77),31,32 trauma symptoms (Impact of Events Scale—Revised [IES-R]; α = 0.79–0.92),33 social support (Yale Social Support Survey [YSS]; α = 0.73),34,35 and social constraints (Social Constraints Inventory [SCI]; α = 0.88).36,37 Participants also provided self-reports of their demographics and cancer history.
A number of specific network attributes were measured for each type of network communication (i.e., discussion board, blog, web mail, and chat), including network density, clustering, path length, average degree, and connectedness. Density was calculated as the proportion of possible ties that were present in the overall network. Clustering was measured by calculating the number of actors with whom each ego was connected and then determining the proportion of those actors connected to one another (i.e., if actor A is connected to actors B, C, D, and E, the clustering coefficient is equal to the number of connections between actors B, C, D, and E divided by the total number of possible connections). Path length was specified as the average distance between any two nodes in the network, and average degree represented the average number of connections shared by each actor in each channel (e.g., if actor 1 shared three connections with other participants, the degree for this actor = 3). Connectedness was calculated as the proportion of all nodes that could be reached from one another. Triad census was measured by calculating the proportion of participants in each communication channel who had connections with each of all possible triads of actors (i.e., zero, one, or two connections within the triad; n = 4,151,022).38 The results of the triad census are presented in Table 3.
Table 3.
Triad Census: Number of Connections Within All Possible Actor Triads by Channel and Percent Deviation from Expected Values
| Blog | Chat | Discussion board | Overall | ||
|---|---|---|---|---|---|
| Unconnected triads | 4,334,010 (+0.4%) | 4,297,986 (−0.5%) | 4,340,826 (+0.5%) | 4,300,071 (−0.4%) | 4,151,022 |
| Triads with 1 connection | 75,266 (−14.6%) | 110,341 (+25.2%) | 68,680 (−22.1%) | 98,290 (+11.5%) | 241,461 |
| Triads with 2 connections | 974 (−74.3%) | 1,474 (−61.1%) | 826 (−78.2%) | 11,896 (+213.7%) | 16,182 |
| Triads with 3 connections | 299 (−23.1%) | 748 (+92.3%) | 217 (−44.2%) | 292 (−24.9%) | 1,884 |
Note: χ2 test (9) = 36,884, p < 0.0001.
Analysis
Unique dyadic interactions for each communication channel were counted. Dyadic interactions consisted of any interaction between two individuals in the study for that communication channel. Replies to a threaded interaction (i.e., an interaction with several participants) were turned into dyadic form by assuming a tie between the replier and every participant to whom they replied in the thread. Social network data sets were generated using UCINET and the Statnet package in R. Isolates (i.e., individuals enrolled in the study who did not participate online) were identified and added into the data set to calculate the network statistics. We removed any duplicate interactions; therefore, multiple interactions between the same two participants were not counted more than once for the purpose of this study.
We used a combination of UCINET and Statnet to calculate the network attributes described in the “Methods” section. We produced network statistics for each communication channel separately. We also identified the communities in each channel. Chi-square analysis was used to test the null hypothesis that communication channels had similar levels of network connectedness. The association between respondents being in the same community in one channel and being in the same community in another is assessed with Cramer's phi coefficients. We used the Girvan–Newman algorithm in UCINET,39 which is a partitioning process that identifies communities by removing edges between communities from the original network. In each communication channel, participants who belonged to a Girvan–Newman community with more than two other participants were classified as belonging to a strong community. Membership in a strong community was then regressed onto demographic, medical, and psychosocial characteristics using logistic regression.
Results
Descriptive network characteristics
Network attributes associated with the health-space intervention are provided in Table 1. Density was quite low overall and in each of the four channels, suggesting that only a small proportion of the total number of participants connected with one another over the course of the intervention. Density in the discussion board and mail channels was higher than that in the blog and chat. However, clustering was relatively high in all channels aside from mail, with 44–60 percent of each participant's ties connected to each other. Path lengths were shorter in the blog, chat, and discussion board relative to the mail channel, although the degree, or number of connections, for each participant was higher in the chat and mail than that in the blog or discussion board. Finally, level of connectedness demonstrated in the mail channel was two to five times higher than that in the other three channels.
Table 1.
Symmetrized Network Statistics for the Overall Network and Each Communication Channel
| Density | Clustering | Path length | Average degree | Connectedness | |
|---|---|---|---|---|---|
| Discussion board | 0.005 | 0.441 | 3.677 | 1.599 | 0.091 |
| Blog | 0.006 | 0.479 | 3.447 | 1.759 | 0.070 |
| 0.009 | 0.069 | 5.045 | 2.769 | 0.395 | |
| Chat | 0.009 | 0.604 | 3.583 | 2.602 | 0.092 |
| Overall | 0.021 | 0.259 | 6.294 | 6.294 | 0.586 |
Note: Network statistics limited to participants (i.e., professional facilitators excluded).
Correlations between channels
To test the hypothesis that having connections in one communication channel would be associated with having similar shared connections in other communication channels, Cramer's phi coefficients were calculated. Being in the same community in one communication channel (e.g., chat) was significantly associated with being in the same community in each of the other communication channels (e.g., blog, discussion board, and mail; see Table 2). These associations were generally quite high (all ps < 0.05), ranging from φ = 0.558 (mail and chat) to φ = 0.887 (discussion board and chat).
Table 2.
Association of Community Comembership by Channel (Cramer's V)
| Blog | Chat | Discussion board | ||
|---|---|---|---|---|
| Blog | 1.000 | |||
| Chat | 0.852* | 1.000 | ||
| Discussion board | 0.852* | 0.887* | 1.000 | |
| 0.722* | 0.558* | 0.792* | 1.000 |
All coefficients are significant at p < 0.05, one tail, by χ2 test.
Connections by channel
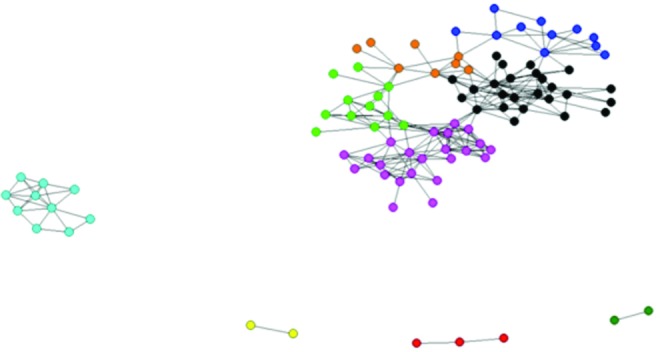
In each of the channels, we noted a substantial tendency toward the formation of fairly dense local clusters and somewhat more loosely connected communities of participants (Figs. 2–5). One way of comparing the “texture” of these connections across channels is to examine the triad census for each channel, that is, what proportion of all triads had no connections, a single dyad and isolated individual, a “line” structure (three actors with two ties), or a fully closed triad. Table 3 displays the results and tests for differences among the channels. It is particularly notable that chat communications had a strong tendency toward clique-like (closed triads) structures, while e-mail communications were very likely to form serial (forwarding) kinds of ties rather than closed ones. In Table 3, the chat communications show a higher number of triads with three connections (the clique-like structure) than the rest of the channels. Mail communications display more triads with two connections, which indicate more serial ties, than the rest of the channels.
FIG. 2.
Network structure of the health-space.net intervention: blogs. Note. 14 communities. Graphics of non-moderated networks. Isolates removed; spring-embedding (default) layout; symmetrized (maximum); node size set by eigen-centrality; node color set by Newman-Girvan community (maximum Q solution). Color images available online at www.liebertpub.com/cyber
FIG. 3.

Network structure of the health-space.net intervention: chat. Note. 6 communities. Graphics of non-moderated networks. Isolates removed; spring-embedding (default) layout; symmetrized (maximum); node size set by eigen-centrality; node color set by Newman-Girvan community (maximum Q solution). Color images available online at www.liebertpub.com/cyber
FIG. 4.

Network structure of the health-space.net intervention: discussion board. Note. 13 communities. Graphics of non-moderated networks. Isolates removed; spring-embedding (default) layout; symmetrized (maximum); node size set by eigen-centrality; node color set by Newman-Girvan community (maximum Q solution). Color images available online at www.liebertpub.com/cyber
FIG. 5.

Network structure of the health-space.net intervention: mail. Note. 5 communities. Graphics of non-moderated networks. Isolates removed; spring-embedding (default) layout; symmetrized (maximum); node size set by eigen-centrality; node color set by Newman-Girvan community (maximum Q solution). Color images available online at www.liebertpub.com/cyber
Participant characteristics associated with community membership
Demographic, medical, and psychosocial characteristics associated with strong community membership in each of the communication channels are displayed in Table 4. Strong discussion board community membership was associated with being recruited via cancer registry instead of the Internet, being assigned to an immediate treatment group, having greater educational attainment, having more severe social constraints, having greater levels of fatigue, and having greater depression and anxiety. Membership in a strong chat community was associated with cancer registry recruitment, being female, and more frequent use of the Internet. Membership in a strong e-mail community was associated with being recruited via the Internet, being assigned to immediate treatment, lower educational attainment, being male, and having fewer days of restricted activities due to cancer. Finally, strong blog community membership was associated with cancer registry recruitment, greater educational attainment, being female, and more days per month of restricted activities due to cancer.
Table 4.
Individual Characteristics Associated with Strong Community Membership in Each Communication Channel
| Discussion board OR (95% CI) | E-mail OR (95% CI) | Chat OR (95% CI) | Blog OR (95% CI) | |
|---|---|---|---|---|
| Recruitment source (Internet vs. registry) | 0.43** (0.23, 0.78) | 4.68*** (2.79, 7.87) | 0.54* (0.31, 0.94) | 0.25*** (0.13, 0.49) |
| Randomized to treatment group | 2.46** (1.39, 4.36) | 1.70* (1.06, 2.73) | 1.66 (0.99, 2.80) | 1.08 (0.64, 1.82) |
| Age (decades) | 0.99 (0.78, 1.26) | 1.14 (0.92, 1.41) | 0.97 (0.77, 1.23) | 0.90 (0.71, 1.14) |
| Education | 1.10* (1.00, 1.21) | 0.89* (0.82, 0.97) | 1.03 (0.94, 1.13) | 1.14** (1.04, 1.26) |
| Gender (female vs. male) | 1.43 (0.74, 2.76) | 0.27*** (0.15, 0.49) | 2.05* (1.06, 3.99) | 2.77** (1.30, 5.91) |
| Frequency of Internet use | 1.11 (0.91, 1.35) | 0.92 (0.79, 1.08) | 1.26* (1.02, 1.57) | 1.17 (0.95, 1.45) |
| Activities restricted due to cancer (days/month) | 1.03 (1.00, 1.06) | 0.95** (0.92, 0.98) | 0.99 (0.96, 1.03) | 1.04** (1.01, 1.08) |
| Advanced stage of disease | 1.15 (0.66, 2.02) | 1.34 (0.80, 2.22) | 1.44 (0.84, 2.44) | 1.28 (0.74, 2.21) |
| Social support | 0.96 (0.89, 1.04) | 1.03 (0.96, 1.11) | 1.02 (0.94, 1.10) | 1.02 (0.94, 1.10) |
| Social constraints | 1.03* (1.00, 1.05) | 0.99 (0.97, 1.00) | 1.02 (0.99, 1.04) | 1.01 (0.99, 1.04) |
| Fatigue | 1.06* (1.01, 1.11) | 0.98 (0.94, 1.02) | 1.04 (0.99, 1.08) | 1.04 (1.00, 1.09) |
| Vigor | 0.97 (0.92, 1.03) | 1.01 (0.96, 1.06) | 1.01 (0.96, 1.07) | 0.99 (0.94, 1.05) |
| Anxiety | 1.06* (1.01, 1.11) | 1.01 (0.97, 1.05) | 1.02 (0.98, 1.06) | 1.03 (0.98, 1.07) |
| Depression | 1.02* (1.00, 1.05) | 1.01 (0.99, 1.03) | 1.00 (0.98, 1.03) | 1.01 (0.99, 1.03) |
| Traumatic stress symptoms | 1.02 (1.00, 1.03) | 1.01 (1.00, 1.03) | 1.01 (0.99, 1.02) | 1.00 (0.99, 1.02) |
| Overall psychological well-being | 1.00 (0.99, 1.01) | 1.00 (0.99, 1.01) | 1.00 (0.98, 1.01) | 1.00 (0.99, 1.01) |
p < 0.05, **p < 0.01, ***p < 0.001.
Community membership and engagement
For three of the four communication channels (discussion board, blog, and chat), membership in a strongly connected community was strongly associated with greater total time spent engaged in the health-space.net intervention, time spent using the structured intervention content, and time spent engaged in any of the social networking features of the intervention Web site (Table 5). Effect sizes were strongest for those who were strongly connected to a chat community (Ds = 1.40–1.84). Being connected to a strong chat community was associated with significantly more time spent using structured intervention content, t(294) = 18.5, p < 0.001, more time spent engaged with any social networking components, t(294) = 13.8, p < 0.001, and more overall time spent using the health-space.net intervention, t(294) = 17.8, p < 0.001. Strong community membership in the e-mail channel was not associated with any measures of engagement with the intervention.
Table 5.
Differences in Intervention Engagement By Membership in a Strong Community Across Each of the Four Communication Channels
| Total time spent using intervention (minutes) | Cohen's D | Time engaged with structured intervention content (minutes) | Cohen's D | Time engaged with any social networking component (minutes) | Cohen's D | |
|---|---|---|---|---|---|---|
| Discussion board | ||||||
| Strong community | 1,048.5 (927)*** | 1.15 | 404.7 (390)*** | 1.08 | 643.8 (610)*** | 1.03 |
| No strong community | 219.9 (431) | 73.9 (188) | 145.9 (309) | |||
| Chat | ||||||
| Strong community | 1,204.1 (846)*** | 1.80 | 488.0 (359)*** | 1.84 | 716.1 (619)*** | 1.40 |
| No strong community | 103.6 (176) | 18.3 (42) | 85.3 (150) | |||
| Blog | ||||||
| Strong community | 1,033.1 (921)*** | 1.13 | 413.1 (398)*** | 1.12 | 620.0 (603)*** | 0.97 |
| No strong community | 221.6 (439) | 69.3 (173) | 152.3 (323.4) | |||
| Strong community | 438.3 (700) | 0.00 | 134.9 (271) | −0.17 | 303.3 (489) | 0.11 |
| No strong community | 438.2 (709) | 184.2 (314) | 253.9 (442) | |||
p < 0.05, **p < 0.01, ***p < 0.001.
Discussion
In general, our results paint a picture of four very different kinds of communication channels that create independent opportunities for participants to interact with one another. Although participants communicated with many of the same people in each of the communication channels, the composition and pattern of interactions varied across communication channels. Taken as a whole, these results suggest that having multiple channels for communication allows participants to expand the number of individuals with whom they are communicating, creates opportunities for communicating with different individuals in distinct channels, and likely enhances overall engagement with the intervention. However, given that distances between members of a community were similar across channels, the flow of information from one participant to another is also likely to be similar across channels, so having at least one channel that is acceptable and engaging for each participant (i.e., one that “works for them”) could be sufficient for effectively communicating relevant intervention content.
For example, in a previous qualitative evaluation of this intervention,24 a number of participants noted that the chat communication channel was “not for me.” For these types of participants, making sure that alternative communication channels are available is key to providing an adequate dose of the intended intervention. There are other clear differences between channels that support this idea that multiple channels may be necessary for delivering intervention content. Web mail was associated with very small clusters and longer path lengths (suggesting that mail was effective in directly connecting pairs of participants and ineffective for fostering communication across clusters or groups of participants), but mail was also associated with the highest number of connections, in terms of both degree and connectedness, between participants. In contrast, chat was associated with relatively strong clustering and connections with other participants, but relatively small numbers of participants became connected to one another through this channel of communication. Although many participants will become connected across multiple communication channels, effective transmission of intervention content may be achieved as long as participants connect to a community in at least one of the available channels.
Our hypothesis that those channels that more heavily used professional facilitation (i.e., chat and discussion board) would be associated with stronger social networks relative to channels requiring less facilitation (i.e., mail and blog) was partially supported. Clustering occurred most strongly in the chat, discussion board, and blog channels, and path length was also shortest in these channels. These results suggest that these channels fostered greater solidarity among participants and stronger community formation. Density was similar across the four channels, but average degree was highest in the mail and chat channels, showing the unevenness of connection in the mail and chat channels compared with the other two channels. On average, participants had more shared connections in the mail and chat channels. Mail was also associated with higher levels of connectedness. These results reflect a greater ease of use or comfort level with the mail channel.
The hypothesis that those participants with higher levels of psychological distress, cancer burden, previous use of technology, and social constraints would be more likely to be integrated into a strong social networking community was also only partially supported. Having more social constraints and worse symptoms of depression and anxiety was associated with membership in a strong discussion board community but not with membership in a strong community in any of the other three channels. Because the discussion board served as the landing or home page for the intervention, it was the most prominent channel for participants, and it did seem that those with greater levels of need for the intervention were most likely to engage with this particular channel. Helping to facilitate engagement with the other channels, particularly for those people who are most in need, is a directive that comes out of the current findings. However, other participant characteristics that had little to do with need for the intervention were associated with strong community memberships in general. With respect to e-mail in particular, its use was associated with Internet recruitment, being male, and having lower educational attainment, suggesting that there is something about this channel that is particularly appealing to these types of users. These findings again highlight the importance of providing multiple channels for interaction, particularly when the population of interest may be diverse with respect to education, gender, and other personal characteristics. Single-channel interventions may be more effective for populations that are less heterogeneous than that in the current study.
This study also clearly demonstrates the importance of strong social communities for promoting utilization and engagement with these kinds of interventions. Being connected to a strong discussion board, chat, or blog community was associated with much higher rates of intervention utilization overall. Those that were connected to one of these communities spent 466 percent to 1,162 percent (i.e., 12–18 hours) more time using the intervention overall. Being connected to a strong chat community was associated very strongly with use of the structured intervention content in particular, suggesting that those who connected with a chat community were much more likely to get a stronger dose of the intended intervention (i.e., exposure to coping skills training exercises and practice) than those who did not.
A notable limitation of the present study is that social networking attributes may be overly conservative given the rolling recruitment used in this study. Because participants could enter a social networking group at any point in time but only had access to the intervention for 12 weeks, participants who entered the study earlier would not have been able to interact with participants who entered later. It is important to note that rolling recruitment would not affect comparisons across channels or the ability to predict membership in strong communities, but a subsequent study will attempt to provide more accurate measures of density, connectedness, degree, path length, and clustering by focusing on specific participant cohorts.
Multiple channels for social interaction in a web-based intervention do contribute to engagement and the formation of different social structures within the intervention, and personal characteristics associated with use of each type of channel vary greatly across channels. These results suggest that providing multiple ways in which individuals can interact with one another, to find and connect with “others like me,” is an ideal strategy for maximizing the dose of intervention that can be provided with technology-based interventions. Additional research is needed to evaluate how community membership changes over time to better understand how to more effectively encourage early integration into a community and maintenance in that community over time and how social networking can impact outcomes over time.
Author Disclosure Statement
No competing financial interests exist.
References
- 1.Laranjo L, Arguel A, Neves AL, et al. The influence of social networking sites on health behavior change: a systematic review and meta-analysis. Journal of the American Medical Informatics Association 2015; 22:243–256 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Owen JE, Bantum EO, Criswell K, et al. Representativeness of two sampling procedures for an internet intervention targeting cancer-related distress: a comparison of convenience and registry samples. Journal of Behavioral Medicine 2014; 37:630–641 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Brindal S, Freyne J, Saunders I, et al. Features predicting weight loss in overweight or obese participants in a web-based intervention: randomized trial. Journal of Medical Internet Research 2012; 14:e173. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Prescott J, Gray NJ, Smith FJ, et al. Blogging as a viable research methodology for young people with arthritis: a qualitative study. Journal of Medical Internet Research 2015; 17:e61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Yu CH, Parsons JA, Mamdani M, et al. A web-based intervention to support self-management of patients with type 2 diabetes mellitus: effect on self-efficacy, self-care, and diabetes distress. BMC Medical Informatics and Decision Making 2014; 14:117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Lauder S, Chester A, Castle D, et al. Development of an online intervention for bipolar disorder: www.moodswings.net.au Psychology, Health & Medicine 2013; 18:155–165 [DOI] [PubMed]
- 7.Hoybe MT, Dalton SO, Deltour I, et al. Effect of internet peer-support groups on psychosocial adjustment to cancer: a randomised study. British Journal of Cancer 2010; 102:1348–1354 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Devi R, Powell J, Singh S. A web-based program improves physical activity outcomes in a primary care angina population: randomized controlled trial. Journal of Medical Internet Research 2014; 16:e186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Van der Zanden R, Curie K, Van Londen M, et al. Web-based depression treatment: associations of clients' word use with adherence and outcome. Journal of Affective Disorders 2014; 160:10–13 [DOI] [PubMed] [Google Scholar]
- 10.Mittal D, Drummond KL, Blevins D, et al. Stigma associated with PTSD: perceptions of treatment-seeking combat veterans. Psychiatric Rehabilitation Journal 2013; 36:86–92 [DOI] [PubMed] [Google Scholar]
- 11.Centola D. An experimental study of homophily in the adoption of health behavior. Science 2011; 334:1269–1272 [DOI] [PubMed] [Google Scholar]
- 12.Kelders SM, Kok RN, Ossebaard HC, et al. Persuasive system design does matter: a systematic review of adherence to web-based intervention. Journal of Medical Internet Research 2012; 14:e152. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Pfeiffer PN, Heisler M, Piette JD, et al. Efficacy of peer support interventions for depression: a meta-analysis. General Hospital Psychiatry 2011; 33:29–36 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Schubart JR, Stuckey HL, Ganeshamoorthy A, et al. Chronic health conditions and internet behavioral interventions: a review of factors to enhance user engagement. Computers Informatics Nursing 2011; 29:TC9-20 [DOI] [PubMed] [Google Scholar]
- 15.Carmack Taylor CL, Kulik J, Badr H, et al. A social comparison theory analysis of group composition and efficacy of cancer support programs. Social Science in Medicine 2007; 65:262–273 [DOI] [PubMed] [Google Scholar]
- 16.Yalom I. (2005) The theory and practice of group psychotherapy. New York: Basic Books [Google Scholar]
- 17.Uchino B. (2004) Social support and physical health: understanding the health consequences of relationships. New Haven, CT: Yale University Press [Google Scholar]
- 18.Falagas ME, Zarkadoulia EA, Ioannidou EN, et al. The effect of psychosocial factors on breast cancer outcome: a systematic review. Breast Cancer Research 2007; 9:R44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Overberg R, Otten W, de Man A, et al. How breast cancer patients want to search for and retrieve information from stories of other patients on the internet: an online randomized controlled experiment. Journal of Medical Internet Research 2010; 12:e7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Rini C, Symes Y, Campo RA, et al. I keep my problems to myself: negative social network orientation, social resources, and health-related quality of life in cancer survivors. Annals of Behavioral Medicine 2016; 50:385–396 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Kim SC, Shah DV, Namkoong K, et al. Predictors of online health information seeking among women with breast cancer: the role of social support perception and emotional well-being. Journal of Computer-Mediated Communication 2013; 18:98–118 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Kroenke CH, Kwan ML, Neugut AL, et al. Social networks, social support mechanisms, and quality of life after breast cancer diagnosis. Breast Cancer Research Treatment 2013; 139:515–527 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Owen JE, Klapow JC, Roth DL, et al. Randomized pilot of a self-guided internet coping group for women with early-stage breast cancer. Annals of Behavioral Medicine 2005; 30:54–64 [DOI] [PubMed] [Google Scholar]
- 24.Winzelberg AJ, Classen C, Alpers GW, et al. Evaluation of an internet support group for women with primary breast cancer. Cancer 2003; 97:1164–1173 [DOI] [PubMed] [Google Scholar]
- 25.Gustafson DH, Hawkins R, Boberg E, et al. Impact of a patient-centered, computer-based health information/support system. American Journal of Preventive Medicine 1999; 16:1–9 [DOI] [PubMed] [Google Scholar]
- 26.Pinquart M, Duberstein PR. Associations of social networks with cancer mortality: a meta-analysis. Critical Reviews in Hematology/Oncology 2010; 75:122–137 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Zhou ES, Penedo FJ, Bustillo NE, et al. Longitudinal effects of social support and adaptive coping on the emotional well-being of survivors of localized prostate cancer. Journal of Supportive Oncology 2010; 8:196–201 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Gorlick A, Bantum EO, Owen JE. Internet-based interventions for cancer-related distress: exploring the needs of those whose needs are not met. Psycho-Oncology 2014; 23:452–458 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Donovan KA, Grassi L, McGinty HL, et al. Validation of the distress thermometer worldwide: state of the science. Psycho-Oncology 2014; 23:241–250 [DOI] [PubMed] [Google Scholar]
- 30.Owen JE, Bantum EO, Gorlick A, et al. Engagement with a social-networking intervention for cancer-related distress. Annals of Behavioral Medicine 2015; 49:154–164 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Radloff L. The CES-D scale: a self-report depression scale for research in the general population. Applied Psychological Measurement 1977; 3:385–401 [Google Scholar]
- 32.Hann D, Winter K, Jacobsen P. Measurement of depressive symptoms in cancer patients: evaluation of the Center for Epidemiological Studies Depression Scale (CES-D). Journal of Psychosomatic Research 1999; 46:437–443 [DOI] [PubMed] [Google Scholar]
- 33.Weiss D, Marmar C. (1996) The impact of event scale–revised. In Wilson J, Keane T, eds. Assessing psychological trauma and PTSD. New York: Guilford, pp. 399–411 [Google Scholar]
- 34.Seeman TE, Berkman LF. Structural characteristics of social networks and their relationship with social support in the elderly: who provides support. Social Science & Medicine 1988; 26:737–749 [DOI] [PubMed] [Google Scholar]
- 35.Butler LD, Koopman C, Classen C, et al. Traumatic stress, life events, and emotional support in women with metastatic breast cancer: cancer-related traumatic stress symptoms associated with past and current stressors. Health Psychology 1999; 18:555–560 [DOI] [PubMed] [Google Scholar]
- 36.Lepore SJ, Ituarte PHG. Optimism about cancer enhances mood by reducing negative social interactions. Cancer Research, Therapy and Control 1999; 8:165–174 [Google Scholar]
- 37.Lepore SJ. (2001) A social-cognitive processing model of emotional adjustment to cancer. In Baum A, Andersen B, eds. Psychosocial interventions for cancer. Washington, DC: American Psychological Association, pp. 99–118 [Google Scholar]
- 38.Hanneman RA, Riddle M. (2005) Introduction to social network methods. Riverside, CA: University of California, Riverside [Google Scholar]
- 39.Girvan M, Newman MEJ. Community structure in social and biological networks. Proceedings of the National Academy of Sciences 2002; 99:7821–7826 [DOI] [PMC free article] [PubMed] [Google Scholar]