

Abstract
Unilateral posterior crossbite is a widespread, asymmetric malocclusion characterized by an inverse relationship of the upper and lower buccal dental cusps, in the molar and premolar regions, on one side only of the dental arch. Patients with unilateral posterior crossbite exhibit an altered chewing cycles and the crossbite side masseter results to be less active with respect to the contralateral one. Few studies about morphological features of masticatory muscle in malocclusion disorders exist and most of these have been performed on animal models. The aim of the present study was to evaluate morphological and protein expression characteristics of masseter muscles in patients affected by unilateral posterior crossbite, by histological and immunofluorescence techniques. We have used antibody against PAX-7, marker of satellite cells, and against α-, β-, γ-, δ-, ε- and ζ-sarcoglycans which are transmembrane glycoproteins involved in sarcolemma stabilization. By statistical analysis we have evaluated differences in amount of myonucley between contralateral and ipsilateral side. Results have shown: i) altered fibers morphology and atrophy of ipsilateral muscle if compared to the contralateral one; ii) higher number of myonuclei and PAX-7 positive cells in contralateral side than ipsilateral one; iii) higher pattern of fluorescence for all tested sarcoglycans in contralateral side than ipsilateral one. Results show that in unilateral posterior crossbite hypertrophic response of contralateral masseter and atrophic events in ipsilateral masseter take place; by that, in unilateral posterior crossbite malocclusion masticatory muscles modify their morphology depending on the function. That could be relevant in understanding and healing of malocclusion disorders; in fact, the altered balance about structure and function between ipsilateral and contralateral muscles could, long-term, lead and/ or worsen skeletal asymmetries.
Key words: Sarcoglycans, satellite cells, skeletal muscle, fluorescence antibody technique, histological techniques, confocal microscopy
Introduction
Interactions between cell and extracellular matrix play a key role in mechanotransduction transmitting forces across the plasma membrane of muscle fibers and they are important for muscular development during somitogenesis, cell migration from somites, correct innervation, and muscle patterning.1-4 Several studies have shown that integrins play a key role in myoblast migration from the somite and in myotube formation.5,6 In the adult muscle, an intact basement membrane-cytoskeletal linkage is important for skeletal muscle stability and integrity. In agreement with several reports,7,8 we have supported a role of integrins in the function of human adult skeletal muscle9) and they have demonstrated a bidirectional signaling between sarcoglycans and integrins;10 this reciprocal control may determine the prevalence of one system over another with a consequent transmission of different messages to the sarcolemma-associated cytoskeleton.9-11 We have shown the correlation between sarcoglycans and integrins and force of contraction in masticatory muscle of primates.12,13 Sarcoglycans are transmembrane glycoproteins which connect extracellular matrix to cytoskeleton; these proteins have been long investigated in muscle tissue because of their role in sarcolemma stabilization during muscle activity; they are considered as important as dystrophin because a mutation in genes encoding α-, β-, γ- and d-sarcoglycans determines limb girdle muscular dystrophy (LGMD).14-17 Adult muscle fibers are provided with quiescent mononucleated myogenic cells, Satellite cells, that are located between the sarcolemma and basement membrane of terminally-differentiated muscle fibers. These are normally quiescent in adult muscle, but act as a reserve population of cells able to proliferate in response to injury or exercises, playing a role in routine maintenance, repair and hypertrophy of adult muscle; thus, satellite cells could give informations about muscle plasticity in response to different work load. Quiescent satellite cells express the paired box transcription factor family member Pax7.18 When activated, they coexpress Pax7 with MyoD,19-21 a key transcription factor for myogenic differentiation and a member of the myogenic regulatory factor (MRFs) family, comprising MyoD, Myf5, myogenin and Mrf4.22 Most activated satellite cells then proliferate, downregulate Pax7 and differentiate. By contrast, other proliferating cells maintain Pax7 but lose MyoD.
Unilateral posterior crossbite is a widespread, asymmetric malocclusion characterized by an inverse relationship of the upper and lower buccal dental cusps, in the molar and premolar regions, on one side only of the dental arch. Patients with unilateral posterior crossbite exhibit an altered kinematics of the mandible – reverse chewing cycles, and altered coordination of the masseter muscles, during mastication on the affected side, being the masseter of the crossbite side less active with respect to the contralateral and to controls.23,24
Few studies have observed morphological features of masticatory muscle in malocclusion conditions; some of these have been performed on rat models showing an increment in extracellular matrix remodeling in contralateral side, probably in response to masticatory muscle remodeling and the presence of atrophic events in crossbite side25 in addition to another study that has observed altered fiber morphology in ipsilateral masseter after occlusal wear.26 In human it has been shown that types of malocclusion may have different masseter lengths and orientations and these differences may have implications for the mechanical advantage in bite force.27 Previous results, carried out on masseter muscle of unilateral posterior crossbite patients, have shown that the expression of integrins was significantly lower in the crossbite side muscle than contralateral masseter suggesting that integrins could play a key role regulating the functional activity of muscle and allowing the optimization of contractile forces.28
Considering the important functional role of the masseter during chewing and the serious alterations of the muscular activation in conditions of posterior crossbite malocclusion, we planned, on the basis of the clinical findings, an histological and immunohistochemical study of the masseter to evaluate the morphological and protein expression aspects.
Materials and Methods
The work has been conducted in accordance with the Declaration of Helsinki (1964) and it has been performed with the understanding and the consent of the human subjects. The work was also approved by local ethics committee, the Institutional Review Board of the University Hospital Health and Science Complex Turin-Italy.
Patients
Ten patients, 5 male and 5 females, 22.5±7 years old (mean ± standard deviation), with severe skeletal class III (point-Nasion-B point angle = – 2.6±1.5 mean ± standard deviation) and unilateral posterior crossbites were recruited to participate in this study. Patients showed left (6 patients) and right (4 patients) unilateral, posterior crossbite involving the molar teeth; five of them were open bite and five were deep bite. Inclusion criteria were as follows: skeletal and dental severe, surgical class III; posterior crossbite and presence of all teeth (with the exception of the third molars). Exclusion criteria were as follows: presence of fixed or removable dental prosthesis; periodontal disease; presence of craniofacial syndromes or clefts; presence of inflammatory or neuromuscular disorders.
The patients received bilateral sagittal split (BSSO) to reduce the mandibular excess. Biopsies of masseter muscle have been withdrawn from left and right sides for each patients
Histological procedures
After withdrawal, the specimens were post-fixed in 2% glutaraldehyde12.5% formaldehyde, buffered in 0.1 M sodium cacodylate, pH 7.4 at room temperature for 4 h. After rinses in phosphate buffer 0.13 mol/L, pH 7.3, the specimens dehydrated in ethanol and embedded in paraffin. Five-µm-thick sections were obtained in a LEICA microtome and stained with hematoxylin and eosin (H&E).
Using H&E stained sections we have performed a count of myonuclei within 200 fibers both of ipsi- and contralateral side.
Immunofluorescence
The muscle biopsies were extracted and were fixed in 3% paraformaldehyde in 0.2 mol/L phosphate buffer, pH 7.4. After numerous rinses in 0.2 mol/L phosphate buffer and phosphate buffered saline, 0.2 mol/L, pH 7.6 with 0.9% NaCl (PBS), they were infiltrated with 12% and 18% saccharose and then they were frozen in liquid nitrogen and were stored at -20°C. By cryotomy, specimens have been cut in 30 µm sections collected on glass slides coated with 0.5% gelatine and 0.005% chromium potassium sulphate. Two series of single localization reactions have been performed: 1) single localization for α-, β-, γ-, δ-, ε- and ζ-sarcoglycans; 2) single localization for PAX-7 positive cells (satellite cells). To block non-specific sites and to make the membranes permeable, the sections were pre-incubated with 1% bovine serum albumin (BSA) and 0.3% Triton X-100 in PBS at room temperature for 15 min. Finally the sections were incubated with primary antibodies at room temperature for 2 h. The following primary antibodies obtained from Santa Cruz Biotechnology, Inc. (Santa Cruz, CA, USA) were used: goat polyclonal anti α-sarcoglycan (diluted 1:100); goat polyclonal anti β-sarcoglycan (diluted 1:100); goat polyclonal anti γ-sarcoglycan (diluted 1:100); goat polyclonal anti δ-sarcoglycan (diluted 1:100); goat polyclonal anti ε-sarcoglycan (diluted 1:100); goat polyclonal anti ζ-sarcoglycan (diluted 1:100); mouse monoclonal anti PAX-7 (diluted 1:100). All primary antibodies were demonstrated with Texas-Red-conjugated IgG anti goat (1:100 dilution; Jackson Immuno-Research Lab., West Grove, PA, USA). The fluorochrome was applied for 1 h at room temperature. After numerous rinses in phosphate buffer and PBS the sections were incubated with DAPI, diluted 1:1000 in PBS (Sigma Aldrich, St. Louis, USA), for 10 min at room temperature to label nuclei. Finally, the slides were washes in PBS and sealed with mounting medium.
Confocal microscopy observations
Samples were observed with a Zeiss LSM 510 confocal microscope equipped with Argon laser (458 nm and 488 nm) and two HeNe laser (543 nm and 633 nm). All images were digitized at a resolution of 8 bits into an array of 2048 x 2048 pixels. Optical sections of fluorescence specimens were obtained at 488 nm, at 62/s scanning shipped with up to 8 repetitions on average. The phinole was set for optimal resolution. Contrast and brightness were established by examining the most brightly labeled pixels and choosing settings that allowed clear visualization of structural details while keeping the highest pixel intensities near 200. Digital images were cropped and figure montages prepared using Adobe Photoshop 7.0.
Results
Contralateral masseter
Hematoxilin-eosin
In masseter muscle of contralateral side it is possible to observe a normal structure of muscle tissue. The fibers present a healthy rectilinear morphology (Figure 1 A,B), with a consistent number of nuclei arranged at the periphery and several myonuclei within the fibers (Figure 1B).
Figure 1.
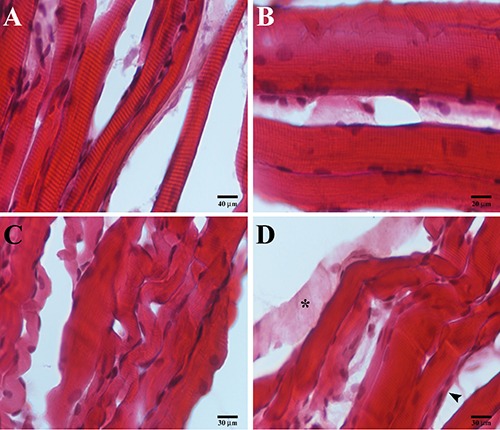
Compound panel of hematoxylin-eosin images of contralateral (A, B) and ipsilateral (C, D) masseter muscles. A) Low magnification of contralateral muscle showing normal and rectilinear fibers morphology. B) High magnification of contralateral muscle showing high number of nuclei within the fibers and along sarcolemma. C) Low magnification of ispilateral muscle showing non-healthy convolute fibers morphology, some atrophic fibers (arrowhead). D) Image of ipsilateral muscle showing the loss of contractile elements within the fiber (asterisk).
Immunofluorescence
The single localization reaction for PAX-7 show that in contralateral masseter muscle there is an high number of satellite cells per fiber which are located between the muscle fiber sarcolemma and the basal lamina (Figure 2 A,B). The transmitted light shows healthy morphology and orientation of fibers (Figure 2 A,B). Single localization reactions for α-sarcoglycans show the presence of an uniform staining pattern along the fibers (Figure 2C); the same result was observed for β-, γ-, δ-, ε- and ζ-sarcoglycans (images no shown)
Figure 2.

Compound panel of three images of immunofluorescence reactions performed in contralateral masseter muscle. A) Longitudinal section of masseter where it is possible to observe rectilinear morphology of fibers and the presence of high number of satellite cells, PAX-7 positive (red channel) which are located between sarcolemma and basal lamina; nuclei are evidenced by DAPI (blue channel); it is also possible to observe the presence of some PAX-7 positive cells within the fibers (arrowhead). B) Transversal section of masseter muscle: presence of high number of PAX-7 positive cells around sarcolemma (red channel). C) Image of single localization reaction for alpha-sarcoglycan: the protein has been detected uniformly along the fibers (red channel) and also in the satellite cells (arrowhead). Bars: 20 μm
Ipsilateral masseter
Hematoxilin-eosin
The masseter muscle of crossbite side show an altered structure as evidenced by the presence of fibers which show to have a convolute morphology and loss of contractile elements. By that, fibers appear chopped in small elements and each of them seem to have different orientation (Figure 1 C,D). Moreover, it is possible to observe signs of atrophy, as evidenced by the presence of very small fibers if compared to the average size of the other fibers, and low number of myonuclei within the fibers (Figure 1C).
Immunofluorescence
In the masseter muscle of crossbite side few PAX-7 positive cells on the periphery of the fibers have been observed, if compared to contralateral side (Figure 3 A,B); transmitted light confirm the convolute morphology of fibers (Figure 3). Moreover, images show a strong reduction of fluorescence pattern along the fibers for a-sarcoglycans (Figure 3C); the same result was observed for β-, γ-, δ-, ε- and ζ-sarcoglycans (images not shown).
Figure 3.
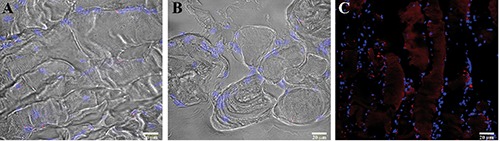
Compound panel of three images of immunofluorescence reactions performed in ipsilateral masseter muscle. A) Longitudinal section of masseter where it is possible to observe an altered, non-rectilinear morphology of fibers and the presence of a lower number of satellite cells PAX-7 positive (red channel) along sarcolemma; nuclei are evidenced by DAPI (blue channel). B) Transversal section of masseter muscle: presence of a very low number of PAX-7 positive cells around sarcolemma (red channel). C) Image of single localization reaction for alpha-sarcoglycan: the protein has not been detected uniformly along the fibers and its fluorescence pattern is almost absent (red channel); satellite cells were positive for alpha-sarcoglycan. Bars: 20 μm
Discussion
In this report we have observed morphological and protein expression aspects of the masseter muscles of both sides of unilateral posterior crossbite patients. Our results, have shown relevant differences in muscle tissue morphology and protein compositions between ipsilateral and contralateral side.
In ipsilateral side we found convolute and chopped muscle fibers which appear as small elements not oriented in the same direction; serious signs of atrophy have been detected as the loss of contractile elements in several fibers and strong reduction of fiber’s size. In our opinion, the morphological characteristics of ipsilateral muscle tissue could depend on reduction of muscle tension exerted by less mechanical loading. By contrast, in contralateral side we found a normal muscle tissue’s structure.
These results are in accordance with Piancino et al.,18 who have demonstrated, by electrognatography and electromyography techniques, that when chewing on the cross-bite side, the chewing patterns show a reverse direction of closure and a reduced activity of the masseter of the same side, while on the non-affected side the chewing pattern and the masseter amplitude are unaltered or increased. Moreover, we have found that between the ipsilateral and contralateral masseters there is a difference in numbers of myonuclei per fibers; in detail we found a greater number of myonuclei in contralateral muscle than ipsilateral muscle. Different studies have suggested that the myonuclei number in the myofiber play an important role during the skeletal muscle size adaptation, since during muscle hypertrophy the myonuclei number are increased (probably through fusion of myogenic cells) while during muscle atrophy the total myonuclei number within muscle fibers are significantly reduced, hypothetically through apoptosis/necrosis.29,30
On this basis, our results show that the increase of myonuclei’s number in contralateral masseter could be an adaptive hypertrophic response to the higher work load exercised on this muscle. That is also supported by results which show higher number of PAX-7 positive cells in contralateral side than ipsilateral side. It is well known that satellite cells are muscle stem cells located between the sarcolemma and the basement membrane of the muscle fiber.31 In humans, satellite cell nuclei are slightly smaller than muscle nuclei and are mostly in a quiescent state.32 Satellite cells are responsible for myonuclear addition during post-natal muscle growth. In addition, their proliferation can be evoked following acute injury33 and in response to muscle overuse and increased tension.34 Our results suggest that the higher mechanical loading exercised on contralateral masseter muscle could determine the satellite cells’ proliferation and myonuclei donation to existing fibers. The satellite cells proliferation in contralateral side could be evidenced by the increase of PAX-7 positive cells if compared to the ipsilateral side and myonuclei donation is evidenced by the higher number of myonuclei detected in contralateral side than ispilateral.
Immunofluorescence results also show that all tested sarcoglycans are more expressed in contralateral muscle than ipsilateral; that is in accordance with previous study which demonstrated an increase of muscle specific integrins expression in contralateral muscle of unilateral posterior crossbite patients where we have hypothesized that integrins could play as markers of muscle strength.23 Since a bidirectional signaling between sarcoglycans and integrins has been found,11 even sarcoglycans could play as markers of muscle strength. On these basis we suggest that in unilateral posterior crossbite an hypertrophic response of contralateral masseter takes place; we explain that by the following events: we hypothesize that the major work load exercised on the non-crossbite side may determine the activation of satellite cells that would proliferate and give nuclei to existent fibers; the increase of myonuclei would determine an improvement of transcription, according to the myonuclear domain theory, with a consequent increase of sarcoglycans which play a key role in sarcolemma stabilization during muscle activity. At the same time ipsilateral side show morphological and protein expression characteristics typical of atrophic or dystrophic muscle, probably for the absence of an adequate stimuli. These results show that in unilateral posterior cross-bite malocclusion masticatory muscles modify their morphology depending on the function. That could be relevant in understanding and healing of malocclusion disorders. In fact, masseter of crossbite side seems to have morphological feature which could anticipate atrophic conditions and the mechanical load exercised by contralateral muscle on skeletal structures could long-term worsen skeletal asymmetries. These results highlight the importance of early therapeutic or surgeon intervention in malocclusion disorders, especially in young patients with unilateral posterior crossbite.
Figure 4.
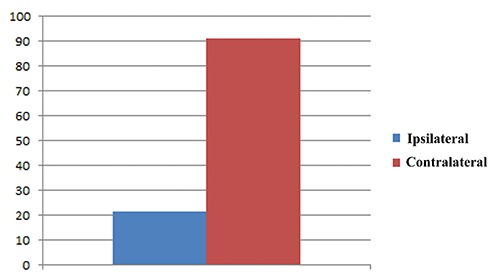
The graphic based on the results obtained by a count of myonuclei within 200 fibers both ipsilateral and contralateral muscle revealed an higher number of myonuclei in contralateral side than ipsilateral one.
Acknowledgments
The present work has been supported by the Department of Biomedical and Dental Sciences and Morphofunctional Imaging, University of Messina, Italy.
References
- 1.Ervasti JM, Ohlendieck K, Kahl SD, Gaver MG, Campbell KP. Deficiency of a glycoprotein component of the dystrophin complex in dystrophic muscle. Nature 1990;345:315-9. [DOI] [PubMed] [Google Scholar]
- 2.Yoshida M, Suzuki A, Yamamoto H, Noguchi S, Mizuno Y, Ozawa E. Dissociation of the complex of dystrophin and its associ-ated proteins into several unique groups by n-octyl β-D-glucoside. Eur J Biochem 1994;222:1055-61. [DOI] [PubMed] [Google Scholar]
- 3.Yoshida M, Ozawa E. Glycoprotein complex anchoring dystrophin to sarcolemma. J Biochem. 1990;108:748-52. [DOI] [PubMed] [Google Scholar]
- 4.Ervasti JM, Campbell KP. A role for the dystrophin-glyco-protein complex as a transmembrane linker between laminin and actin. J Cell Biol 1993;122:809-23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Jaffredo T, Horwitz AF, Buck CA, Rong PM, Dieterlen-Lievre F. Myoblast migration specifically inhibited in the chick embryo by grafted CSAT hybridoma cells secreting an anti- integrin antibody. Development 1988;103:431-46. [DOI] [PubMed] [Google Scholar]
- 6.Menko AS, Boettiger D. Occupation of the extracellular matrix receptor, integrin, is a control point for myogenic differentiation. Cell 1987;51:51-7. [DOI] [PubMed] [Google Scholar]
- 7.Song WK, Wang W, Foster RF, Bielser DA, Kaufman SJ. H36-α7 is a novel integrin alpha chain that is developmentally regulated during skeletal myogenesis. J Cell Biol 1992;117:643-57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Monemi M, Kadi F, Liu JX, Thornell LE, Eriksson PO. Adverse changes in fibre type and myosin heavy chain composition of human jaw. Acta Physiol Scand 1999;167:339-45. [DOI] [PubMed] [Google Scholar]
- 9.Anastasi G, Cutroneo G, Rizzo G, Arco A, Santoro G, Bramanti P, et al. Sarcoglycan and integrin localization in normal human skeletal muscle: a confocal laser scanning microscope study. Eur J Histochem 2004;48:245-52. [PubMed] [Google Scholar]
- 10.Anastasi G, Amato A, Tarone G, Vita G, Monici MC, Magaudda L, et al. Distribution and localization of vinculin-talin-integrin system and dystrophin-glycoprotein complex in human skeletal muscle. Cells Tissues Organs 2003;175:151-64. [DOI] [PubMed] [Google Scholar]
- 11.Yoshida T, Pan Y, Hanada H, Iwata Y, Shigekawa M. Bidirectional signaling between sarcoglycans and the integrin adhesion system in cultured L6 myocytes. J Biol Chem 1998;273:1583-90. [DOI] [PubMed] [Google Scholar]
- 12.Favaloro A, Speranza G, Rezza S, Gatta V, Vaccarino G, Stuppia L, et al. Muscle-specific integrins in masseter muscle fibers of chimpanzees: an immunohistochemical study. Folia Histochem Cytobiol 2009;47:551-8. [DOI] [PubMed] [Google Scholar]
- 13.Cutroneo G, Centofanti A, Speciale F, Rizzo G, Favaloro A, Santoro G, et al. Sarcoglycan complex in masseter and sternocleidomastoid muscles of baboons: an immunohistochemical study. Eur J Histochem 2015;59:2509. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Bönnemann CG, Modi R, Noguchi S, Mizuno Y, Yoshida M, Gussoni E, et al. Beta-sarcoglycan (A3b) mutations cause autosomal recessive muscular dystrophy with loss of the sarcoglycan complex. Nat Genet 1995;11:266-73. [DOI] [PubMed] [Google Scholar]
- 15.Noguchi S, McNally EM, Ben Othmane K, Hagiwara Y, Mizuno Y, Yoshida M, et al. Mutations in the dystrophin-associated protein gamma-sarcoglycan in chromosome 13 muscular dystrophy. Science 1995;270:819-22. [DOI] [PubMed] [Google Scholar]
- 16.Duggan DJ, Manchester D, Stears KP, Mathews DJ, Hart C, Hoffman EP. Mutations in the delta-sarcoglycan gene are a rare cause of autosomal recessive limb-girdle muscular dystrophy (LGMD2). Neurogenetics 1997;1:49-58. [DOI] [PubMed] [Google Scholar]
- 17.Endo T, Kawai H. [Adhalin(alpha-sarcoglycan) gene mutations in patients with malignant limb-girdle muscular dystrophy (MLGMD) (Miyoshi)]. [Article in Japanese]. Nihon Rinsho 1997;55:3159-64. [PubMed] [Google Scholar]
- 18.Seale P, Sabourin LA, Girgis-Gabardo A, Mansouri A, Gruss P, Rudnicki MA. Pax7 is required for the specification of myogenic satellite cells. Cell 2000;102:777-86. [DOI] [PubMed] [Google Scholar]
- 19.Grounds MD, Garrett KL, Lai MC, Wright WE, Beilharz MW. Identification of skeletal muscle precursor cells in vivo by use of MyoD1 and myogenin probes. Cell Tissue Res 1992;267:99-104. [DOI] [PubMed] [Google Scholar]
- 20.Yablonka-Reuveni Z, Rivera AJ. Temporal expression of regulatory and structural muscle proteins during myogenesis of satellite cells on isolated adult rat fibers. Dev Biol 1994;164:588-603. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Zammit PS, Heslop L, Hudon V, Rosenblatt JD, Tajbakhsh S, Buckingham ME, Beauchamp JR, Partridge TA. Kinetics of myoblast proliferation show that resident satellite cells are competent to fully regenerate skeletal muscle fibers. Exp Cell Res 2002;281:39-49. [DOI] [PubMed] [Google Scholar]
- 22.Tajbakhsh S, Buckingham M. The birth of muscle progenitor cells in the mouse: spatiotemporal considerations. Curr Top Dev Biol 2000;48:225-68. [DOI] [PubMed] [Google Scholar]
- 23.Piancino MG, Farina D, Talpone F, Merlo A, Bracco P. Muscular activation during reverse and non-reverse chewing cycles in unilateral posterior crossbite. Eur J Oral Sci 2009;117:122-8. [DOI] [PubMed] [Google Scholar]
- 24.Piancino MG, Comino E, Talpone F, Vallelonga T, Frongia G, Bracco P. Reverse-sequencing chewing patterns evaluation in anterior versus posterior unilateral crossbite patients. Eur J Orthod 2012;34:536-41. [DOI] [PubMed] [Google Scholar]
- 25.Guerra C de S, Carla Lara Pereira Y, Issa JP, Luiz KG, Guimarães EA, Gerlach RF, et al. Histological, histochemical, and protein changes after induced malocclusion by occlusion alteration of Wistar rats. Biomed Res Int 2014;2014:563463. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Bani D, Bani T, Bergamin M. Morphologic and biochemical changes of the masseter muscles induced by occlusal wear: studies in a rat model. J Dent Res 1999;78:1735-44. [DOI] [PubMed] [Google Scholar]
- 27.Becht MP, Mah J, Martin C, Razmus T, Gunel E, Ngan P. Evaluation of masseter muscle morphology in different types of malocclusions using cone beam computed tomography. Int Orthod 2014;2:32-48. [DOI] [PubMed] [Google Scholar]
- 28.Cutroneo G, Piancino MG, Ramieri G, Bracco P, Vita G, Isola G, et al. Expression of muscle-specific integrins in masseter muscle fibers during malocclusion disease. Int J Mol Med 2012;30:235-42. [DOI] [PubMed] [Google Scholar]
- 29.Allen DL, Roy RR, Edgerton VR. Myonuclear domains in muscle adaptation and disease. Muscle Nerve 1999;22:1350-60. [DOI] [PubMed] [Google Scholar]
- 30.Roy RR, Monke SR, Allen DL, Edgerton VR. Modulation of myonuclear number in functionally overloaded and exercised rat plantaris fibers. J Appl Physiol 1999;87:634-42. [DOI] [PubMed] [Google Scholar]
- 31.Mauro A. Satellite cell of skeletal muscle fibers. J Biophys Biochem Cytol 1961;9:493-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Watkins SC, Cullen MJ. A quantitative comparison of satellite cell ultrastructure in Duchenne muscular dystrophy, polymyositis, and normal controls. Muscle Nerve 1986;9:724-30. [DOI] [PubMed] [Google Scholar]
- 33.Bischoff R, Heintz C. Enhancement of skeletal muscle regeneration. Dev Dyn 1994;201:41-54. [DOI] [PubMed] [Google Scholar]
- 34.Hawke TJ, Garry DJ. Myogenic satellite cells: physiology to molecular biology. J Appl Physiol 1985;91:534-51. [DOI] [PubMed] [Google Scholar]