

Abstract
Introduction:
Prevention of oral diseases can be achieved by preventive measures. There is an educational component associated to the preventive aspect. Health education is a cornerstone to the success of a preventive programme. Health education has always been regarded as a primary tool in imparting awareness, bringing changes in healthy behaviors and improved life.
Aim:
To assess the effectiveness of an Educational Video in improving oral health knowledge of subjects in a hospital setting.
Methodology:
The study was conducted in Outpatient Department, CDER, AIIMS. This was a cross sectional interventional study. In the present study a total of 109 subjects were considered those who completed pre and post intervention questionnaire. In order to assess baseline oral health knowledge, a-14 itemed questionnaire was specially designed, based on the contents of video and was pre-tested on 10 patients. Pre-intervention knowledge was assessed and then the 30-minute video was shown. Following this, post-exposure knowledge was assessed using the same questionnaire. Change in the knowledge score amongst the subjects was assessed pre and post-intervention (showing the video film).
Results:
Paired t- test was used to analyze the data. Pre-intervention mean knowledge score was 9.49±2.09 which increased to 11.55±1.60 post-intervention; the difference was statistically significant (P < 0.001).
Conclusions:
It was found that increase in knowledge score was statistically significant after exposure to an educational video film in a hospital setting. Incorporation of video in imparting oral health education can be an effective tool in improving oral health knowledge, which can impact the oral health behavior of people and community.
Keywords: Audio–visual aid, educative video, knowledge score, oral health education
INTRODUCTION
Oral diseases qualify as major public health problem owing to their high prevalence and incidence in all regions of the world (WHO Report 2003). India is no exception and due to its large population size, the absolute burden of oral diseases is immense.[1] The irony of the problem is that most oral diseases are preventable to a great extent, but unfortunately, adequate efforts are lacking in that direction. The etiology of oral diseases can easily be related to various known risk factors and therefore can easily be controlled. The model for risk factor approach in the promotion of oral health as suggested by the World Health Organization emphasizes the role of modifiable risk behaviors such as oral hygiene practices, diet, tobacco, and alcohol abuse (WHO Report 2003). To tackle the overwhelming problem of oral diseases, effectively targeting modifiable risk behaviors through oral health education along with concurrent curative procedures can have a significant impact in reducing the burden of oral diseases in a country like India with a large population size.
Oral health education, an important component of oral health promotion, has been considered an essential part of dental health services.[2] It aims to promote oral health primarily by providing information to improve awareness, leading to adoption of a healthier lifestyle, positive attitudes, and good oral health behavior.[3,4,5,6] Health education and preventive dental care interventions not only reduce the incidence of oral diseases but are also cost-effective, easy to administer, and logical to use at community level.[4] Health education is a widely accepted approach in the prevention of oral diseases, a process of transmission of knowledge and skills are necessary for improvement in oral health and quality of life. The goal of planned health education program is not only to bring about new behaviors but also to reinforce and maintain healthy behaviors that will promote and improve individual, group, or community health.[7] It concentrates on developing such health practices as are believed to bring about the best possible state of well-being.[8] The presumption is that health education follows a knowledge, attitude, and behavior route, with information being transmitted, resulting in attitude and behavior change.[7]
Audiovisual aids are valuable tools in education, more so, in the field of health education, as these have a long-lasting impression on the target population. Studies utilizing audiovisual aids to improve oral health have found them to be effective in improving oral health knowledge of target groups.[9,10,11] Videotapes have been used as a teaching tool for many years; a major advantage being better visualization of practical techniques during small group teaching. Videotaped instructions have been shown to be more effective than traditional lectures, as means of teaching clinical skills. It was documented that videotaped recordings were as effective as live demonstration in teaching interventional skills, clinical methods, and practical techniques to medical and dental students.[12] Videos provide a practical and entertaining audiovisual medium for health education that is suitable for both group and individual learning. Videos offer a standardized level of teaching, and information on the video can be repeated according to the viewers' needs.[13,14]
The Ministry of Health and Family Welfare, Government of India, had initiated a pilot project on National Oral Health Care Programme (1999–2005). The Centre for Dental Education Research (erstwhile Department of Dental Surgery), AIIMS, New Delhi, was given the responsibility of developing and implementing the program strategy. A video film of 30 min duration, entitled “Smile please!” (“Kripya Muskuraiye” in National Hindi language) was produced with actors in different settings, combined with animation in an interesting narrative style. The video covered the following topics:
Anatomy, functions, and eruption pattern of teeth
Causes and prevention of common oral diseases: Dental caries, periodontal disease, malocclusion, trauma, and oral cancer
Correct method of oral hygiene maintenance
Importance of prevention and early diagnosis in cases of orofacial trauma.
The present study was conducted with an aim to assess the effectiveness of this audiovisual film in improving oral health knowledge of subjects attending the Centre for Dental Education and Research, AIIMS, New Delhi, in the waiting area of the Oral Medicine and Radiology Department, the first contact point, where all the patients must report for screening, before referral to the other departments.
Objective
The objective of this study is to assess the effectiveness of an oral health educational video in improving oral health knowledge of subjects in a dental hospital setting.
METHODOLOGY
The methodology for the present study was approved by the Institutional Ethics Committee of AIIMS, New Delhi.
A 14-item questionnaire was designed by the investigators, based on the content of the video film. The Hindi translation of the same was validated as per standard method. A pilot study was conducted with ten subjects to assess the comprehensibility of the questionnaire and the relevant necessary changes were incorporated in the questionnaire.
Sample size was determined based on the anticipated difference in pre- and post-intervention knowledge scores. Assuming mean ± standard deviation (SD) preintervention knowledge score as 7.0 ± 3.0 and anticipating at least 30% improvement due to intervention, i.e. postintervention mean ± SD knowledge score as 9 ± 4. To detect this difference with 90% power and 95% confidence level, the required minimum number of subjects was calculated to be 28. However, to improve the validity of study findings, the pro forma was distributed among 126 subjects. Of these, 109 pre- and post-intervention questionnaires could be collected, as some of the patients were short of time and could not complete the postintervention questionnaire.
Inclusion criteria
Subjects aged >18 years
Those who gave positive informed consent.
Exclusion criteria
Subjects not willing to participate in the study
Subjects who had already seen the video earlier during the previous visit to the center.
Data collection
A self-administered preintervention questionnaire was distributed to the subjects. The questionnaire was distributed in two languages: Hindi and English, depending on the patients' preferred language. Sufficient time was given to every patient to fill the details and mark the correct option of every item of the questionnaire. After collection of preintervention questionnaire, the subjects were shown the video for its full duration of 30 min. The above-mentioned video film is displayed on a regular basis in the waiting area of the outpatient department (OPD). The setting in which the video is displayed is a waiting area with continuous movement of people which is inevitable. Keeping the normal seating in any waiting area of the hospital in mind, the study was planned in the same natural setting. The sitting arrangement in the area is such that the screen is fixed on one wall, and the waiting seats are placed in rows of 3 each. In this arrangement, the audibility is better among the first few rows compared to back rows.
A total of 109 subjects could complete filling both, the pre- and post-viewing pro forma. Data entry was carried out in MS Excel sheet and analyzed using software Stata 11.0, (Stata Corp. LP, USA).
RESULTS
The distribution of the subjects according to gender is listed in Table 1.
Table 1.
Distribution of sample according to the gender

A score of 1 was assigned to every correct answer thereby the maximum score possible was 14. Equal weightage was given to all the questions. The knowledge score of pre and post intervention have been depicted in Graph 1.
Graph 1.
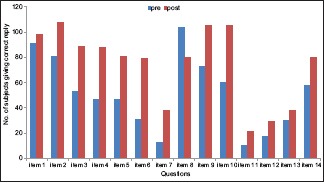
Item-wise pre- and post-intervention knowledge score
To compare the difference in knowledge, pre- and post-intervention, paired t-test was applied and P < 0.05 was considered statistically significant. It was observed that the mean ± SD preintervention knowledge score was 9.49 ± 2.09, whereas postintervention was 11.55 ± 1.60. The difference was found to be statistically significant with P < 0.001 [Table 2].
Table 2.
Comparison of knowledge score before and after intervention

Among the 14 items, it was observed that maximum difference was obtained with the following items:
It is not necessary to treat tooth decay in milk teeth as they will fall out after sometime and new teeth will come
When should the mother start brushing a child's teeth?
What should be done in case a tooth falls out due to injury?
What are the signs of oral cancer?
DISCUSSION
Every person has a different learning style or characteristic for processing information. Based on differences in learning style, various educational methods can have a role in oral health education programs.[12] It has been well recognized that a single mode of health education can never suit all learners. With the advancement in technology and the improvement in literacy rate, there is a need for amalgamation of various newer methods in imparting oral health education. Audiovisual demonstration through illustration clarifies any point better than other techniques, and an educational film makes use of this fact.[15]
In the present study, the questionnaire had components from various aspects of oral health, and it was difficult to assign weightage to different questions. Therefore, the investigators had assigned a score of 1 for every correct and 0 for an incorrect answer. A significant difference was found in the pre- and post-intervention knowledge scores, signifying the fact that there is a need for oral health education program in the general population. Various other studies have also documented effective improvement in attitude of subjects, using video instruction.[16,17]
Health messages through educational materials such as leaflets can change individuals' behaviors.[15] However, it has been recommended that pamphlet is more effective if used with some other intervention method.[18] Although web-based audiovisual programs are found effective and can be updated periodically, they may not be feasible in all settings, due to various reasons such as computer literacy, affordability, and access. With the increase in application of computer technology in India, a DVD-based video film can be an effective mode of oral health education in an oral health-care setting such as dental hospitals, schools, nursing homes, or private clinics. Eaton et al., 2008, concluded that even a slight gain in skill or improvement in knowledge is an indicator of success.[19] Like any other health education, oral/dental health education is plagued with the problem of retention of knowledge and transferring the information to practice. Thus, reinforcement is the key for retention of new knowledge or acquiring a skill.
In the present study, the major difference in knowledge among 14 items was associated with the following items:
-
Is there a necessity to treat tooth decay in milk teeth as they fall out after sometime and new teeth will erupt?
It has been known that people do not attach much importance to care of primary teeth with the belief that these will eventually fall out. In the present study, also it was found that only 31 of 109 subjects were aware of importance of milk teeth preintervention. After the intervention, almost 2-fold increase was observed in the subject's knowledge. Awareness needs to be brought to the general population regarding the importance of milk teeth and their care and importance of their retention. Tooth decay can reduce the masticatory efficiency and esthetics; the developing tooth bud may develop hypoplasia, besides causing malocclusion in permanent dentition. The knowledge score has shown improvement since this aspect has been highlighted properly in the video.
-
When should a mother start brushing a child's teeth?
Lack of knowledge regarding the brushing skill exists since ages. It was observed in this study that merely ten subjects had knowledge regarding the accurate age to start brushing preintervention, whereas postintervention, a significant change was observed. As per the American Dental Association guidelines, the mother should start brushing a child's teeth, as soon as the first tooth erupts in the oral cavity, to prevent the accumulation of plaque on the erupting tooth.
What should be done in case a tooth falls out due to injury?
Injury to primary and permanent teeth and their supporting structures is one of the common dental problems seen in children. Dental injuries can result in functional and esthetic impairment and lead to great concerns, both for the parents and for the child. Informing about possibility of an avulsed (tooth fallen out of its socket) can be reimplanted and how to store the tooth, importance of immediate replantation without time loss, etc., can save many avulsed teeth and prevent psychological trauma, physical morbidity, and cost of prosthetic rehabilitation. Self-management of avulsed tooth was shown very effectively in the video; thereby it could bring about a significant change in knowledge.
-
Signs of oral cancer
Although one-to-one counseling for quitting tobacco is considered to be the most effective method for producing behavior change, AV film depicting early and late stages of oral cancer resulting after tobacco use can also have a powerful impact. Gordon et al., 2004, conducted a study to compare the effect of tobacco education program by dentist, telephonic conversation, and utilizing 5 As (ask, advice, assess, assist, and arrange) and concluded that interactive educational program is engaging, easy to use, and increases the knowledge in tobacco cessation.[20] Thus, it can be ascertained that knowledge about the harmful effects of tobacco, self-examination of oral cavity leading to early detection, can bring a major difference in the incidence of oral cancer.
In the present study, the difference in mean knowledge was found to be more in males compared to females though it was statistically not significant. This could be attributed to the unequal distribution of sample according to gender in the study. Yazdani et al. conducted a cluster randomized trial in a school health education program, in which health education was given either by a leaflet or by videotape.[15] At an interval of 12 weeks, a significant reduction was obtained in plaque and gingival index. Fifty percent improvement in oral cleanliness measured by plaque index occurred in 58% (P < 0.001) of those students in the leaflet group, in 37% (P < 0.001) in the videotape group, and in 10% in the control group. A minimum 50% improvement in gingival health appeared in 72% (P < 0.001) of those students in the leaflet group, in 64% (P < 0.001) of those in the videotape group. It was found in the study that boys showed more improvement in their oral cleanliness and gingival health than the girls, a result perhaps related to gender preferences in educational materials and to sociocultural factors.
The details on sociodemographic factors were voluntary, and 91 subjects gave the information on education status. Thus, the results have not been tabulated for the same. Being a mixed population, the baseline knowledge score was high in many patients and hence corresponding increase after exposure to the video could not be appreciated. In few subjects, no difference in knowledge was observed, as they scored the maximum score in the preintervention itself, leading to no scope in increase in knowledge score.
One potential reason for the low postintervention knowledge score among few subjects was that subjects were in a hurry to get the advised treatment done in the same visit. Thus, due concentration could not be given at a part of the film, leading to reduction in the postknowledge score among subjects. This study of a single exposure to videotape-based educational tool revealed that such intervention can be an effective tool in improving oral health knowledge.
Advantages
It is a practical and easy to understand medium for imparting health education
It offers a standardized level for teaching
Information can be repeated as many times as desired[21]
Video is a convenient tool for educating audiences with low literacy level and have limited learning skills, as level of literacy will have very little effect on learning through video.
Limitations of the study
The sample was drawn from the patients visiting the OPD in a tertiary care center; thus, it does not represent the entire population. The video was shown only once; thus, the impact of reinforcement could not be evaluated.
CONCLUSION
The oral health educational film was found to be effective in increasing oral health-related knowledge of the subjects waiting in a tertiary care hospital. In the rapidly advancing scientific era, educational videos have emerged as relatively popular tool for imparting health education. The embedding of video in bringing oral health awareness can make a significant difference in the knowledge and attitude of the public. Video enhances, dramatizes, and brings a sense of realism, which can have a great impact on the population. Hence, videotape can be a useful adjunct in teaching about oral health in Indian setup/population.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
We sincerely thank all the participants for giving their valuable time in watching the educational video and filling the questionnaire.
REFERENCES
- 1.Shah N. NCMH Background Papers-Burden of Disease in India. National Commission on Macroeconomics and Health. New Delhi: Ministry of Health and Family Welfare, Govt. of India; 2005. [Last accessed on 2015 Feb 10]. Oral and dental diseases: Causes, prevention and treatment strategies. Available from: http://www.mohfw.nic.in/reports_on_ncmh.htm . [Google Scholar]
- 2.Biesbrock AR, Walters PA, Bartizek RD. Initial impact of a national dental education program on the oral health and dental knowledge of children. J Contemp Dent Pract. 2003;4:1–10. [PubMed] [Google Scholar]
- 3.Astrøm AN, Samdal O. Time trends in oral health behaviors among Norwegian adolescents: 1985-97. Acta Odontol Scand. 2001;59:193–200. doi: 10.1080/00016350152509193. [DOI] [PubMed] [Google Scholar]
- 4.Hebbal M, Ankola AV, Vadavi D, Patel K. Evaluation of knowledge and plaque scores in school children before and after health education. Dent Res J (Isfahan) 2011;8:189–96. doi: 10.4103/1735-3327.86036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Honkala S, Honkala E, Rimpelä A, Vikat A. Oral hygiene instructions and dietary sugar advice received by adolescents in 1989 and 1997. Community Dent Oral Epidemiol. 2002;30:124–32. doi: 10.1034/j.1600-0528.2002.300206.x. [DOI] [PubMed] [Google Scholar]
- 6.Ostberg AL. Adolescents' views of oral health education. A qualitative study. Acta Odontol Scand. 2005;63:300–7. doi: 10.1080/00016350510020061. [DOI] [PubMed] [Google Scholar]
- 7.Pine CM. Community Oral Health. 2nd ed. Oxford: Wright; 1997. pp. 188–205. [Google Scholar]
- 8.Peter S. Essentials of Preventive and Community Dentistry. 2nd ed. New Delhi: Arya Publishing House; 2003. Health education; pp. 534–58. [Google Scholar]
- 9.Alsada LH, Sigal MJ, Limeback H, Fiege J, Kulkarni GV. Development and testing of an audio-visual aid for improving infant oral health through primary caregiver education. J Can Dent Assoc. 2005;71:241. [PubMed] [Google Scholar]
- 10.Lachapelle D, Desaulniers G, Bujold N. Dental health education for adolescents: Assessing attitude and knowledge following two educational approaches. Can J Public Health. 1989;80:339–44. [PubMed] [Google Scholar]
- 11.Rothe V, Kebriaei A, Pitner S, Balluff M, Salama F. Effectiveness of a presentation on infant oral health care for parents. Int J Paediatr Dent. 2010;20:37–42. doi: 10.1111/j.1365-263X.2009.01018.x. [DOI] [PubMed] [Google Scholar]
- 12.Packer ME, Rogers JO, Coward TJ, Newman PS, Wakeley R. A comparison between videotaped and live demonstrations, for the teaching of removable partial denture procedures. Eur J Dent Educ. 2001;5:17–22. doi: 10.1034/j.1600-0579.2001.005001017.x. [DOI] [PubMed] [Google Scholar]
- 13.Gagliano ME. A literature review on the efficacy of video in patient education. J Med Educ. 1988;63:785–92. doi: 10.1097/00001888-198810000-00006. [DOI] [PubMed] [Google Scholar]
- 14.Palin-Palokas T, Nordblad A, Remes-Lyly T. Video as a medium of oral health education for children with mental handicaps. Spec Care Dentist. 1997;17:211–4. doi: 10.1111/j.1754-4505.1997.tb00899.x. [DOI] [PubMed] [Google Scholar]
- 15.Yazdani R, Vehkalahti MM, Nouri M, Murtomaa H. School-based education to improve oral cleanliness and gingival health in adolescents in Tehran, Iran. Int J Paediatr Dent. 2009;19:274–81. doi: 10.1111/j.1365-263X.2009.00972.x. [DOI] [PubMed] [Google Scholar]
- 16.Bennell FB. Audio-visual aids in health education. J Sch Health. 1957;27:21–5. doi: 10.1177/001789694900700109. [DOI] [PubMed] [Google Scholar]
- 17.Machen JB, Johnson R. Desensitization, model learning, and the dental behavior of children. J Dent Res. 1974;53:83–7. doi: 10.1177/00220345740530013701. [DOI] [PubMed] [Google Scholar]
- 18.Bonevski B, Newell S. Development of Written Health Education Materials: A Review. 1999. [Last accessed on 2015 Feb 10]. Available from: http://www.epubs.scu.edu.au/cgi/pdf .
- 19.Eaton KA, Reynolds PA, Cox MJ. Top of the pops – CD-ROM and DVDs in dental education. Br Dent J. 2008;204:203–7. doi: 10.1038/bdj.2008.106. [DOI] [PubMed] [Google Scholar]
- 20.Gordon JS, Severson HH, Seeley JR, Christiansen S. Development and evaluation of an interactive tobacco cessation CD-ROM educational program for dental students. J Dent Educ. 2004;68:361–9. [PubMed] [Google Scholar]
- 21.Stegeman CA, Zydney J. Effectiveness of multimedia instruction in health professions education compared to traditional instruction. J Dent Hyg. 2010;84:130–6. [PubMed] [Google Scholar]