

Abstract
Background and Objective:
In the contemporary scenario of both parents employed, there seems to be limited focus on the dietary habits and dental health of their children. Hence, we attempted to correlate the socioeconomic and working status of the parents to the incidence of their children's dental caries.
Materials and Methods:
One thousand school children aged between 3 and 12 years were enrolled in the study. Socioeconomic and working status of their parents was obtained by a pretested questionnaire following which these children were examined for their dental caries status. The data collected were statistically analyzed using logistic regression analysis and calculation of odds ratio.
Results:
A significant correlation was observed between working status of the parents and dental caries status of their children. Though, the socioeconomic status and dental caries had a weak correlation, the odds ratio was high, indicating that the children of lower socioeconomic status or family with both parents employed were at a higher risk for dental caries.
Conclusion:
Efforts are needed to implement programs at the school level to enhance the oral and dental health among children, as parental responsibilities toward this maybe inadequate due to economic or time constraints.
Key words: Dental caries, parents, socioeconomic status, working status
INTRODUCTION
Physical and emotional health, cognitive development, as well as social functioning in children are strongly influenced by the social status and functioning of their family. A family's functioning reflects its composition and the characteristics of its members, their talents, disposition, and daily activities. Social status is reported to be a powerful determinant to affect child's health. However, the mechanisms by which social status might influence health remain underspecified. By and large, three measures of social status as predictors of adverse health outcomes are assessed, i.e., income, education, and occupation or a combination of these factors.[1]
In addition to the social status, the quality of time parents dedicate toward upbringing their child/children can also impact health and developmental outcomes. This is specifically relevant in developing good oral hygiene practices among children.[2] A comprehensive review of the literature revealed, lack of adequate information, on the effect of working and socioeconomic status of the parents on the dental caries of the children. Hence, this study was conducted with the objective of correlating the working and socioeconomic status of parents with the dental caries status of their children.
MATERIALS AND METHODS
Nellore district, according to 2011 census has a total population of 29,63,557. To calculate the sample size with the confidence level being set at 99% and confidence interval of ± 4.5 the sample size needed was 822. However, considering the drop outs a sample of 1000 children was taken. Sample size formula used was
Where:
Z = Z value (99% confidence level).
p = percentage picking a choice, expressed as decimal.
c = confidence interval, expressed as decimal.
Thus, 1000 school going children aged 3-12 years from various schools in Nellore District, Andhra Pradesh, India, were randomly selected for this study. The study was approved by the institutional ethics committee. Pretested questionnaire forms to be filled by parents were distributed to the children. Questions regarding the socioeconomic and the working status of the parents were included; the socioeconomic division was based on the Kuppuswamy classification.[3] The selected children were examined by a single calibrated examiner (principal investigator) for dental caries, using the criteria as given by Klein et al.,[4] and the caries were recorded onto a standardized density functional theory and dynamical mean field theory recording form by a trained assistant.
Data analysis
The data collected was analyzed with the SPSS software 18.0 version (IBM SPSS Statistics 18, SPSS South Asia, Bangalore, India), using multiple logistic regression analysis, odds ratio and Chi-square test with the level of significance set at 0.05.
RESULTS
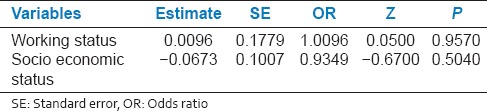
Out of the 1000 children examined, 443 (44.3%) were boys and 557 (55.7%) were girls. Out of the 1000 respondent parents, 701 (70.1%) were both working, whereas 299 (29.9%) were with only one parent working. Children from families, where both parents were employed had significantly (P = 0.0170) increased the prevalence of caries in primary dentition [Table 1a] and the odds ratio showed a higher risk for caries in permanent dentition [Table 1b].
Table 1a.
Representation of working and socioeconomic status of parents and decayed filled teeth of their children
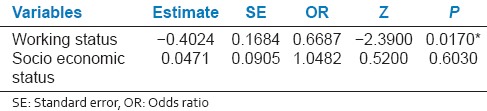
Table 1b.
Representation of working and socioeconomic status of parents and decayed missing filled teeth of their children
DISCUSSION
Prevalence of dental caries is on the rise, in many developing countries. In India, the National Oral Health Survey and Fluoride Mapping found a high prevalence (51.9%) of caries in primary dentition of 5-year-old children.[5]
Dental caries is multifactorial, but the two main factors that can have a devastating effect on oral health of children are the social status and the parental care. The socioeconomic status will have an impact on the knowledge and attitude of parents[3] and hence, can impact parental care. In the present study, children of higher socioeconomic group were at a lower risk of caries (6.4%), which was evident by the odds ratio; however, children from lower socioeconomic status family showed a greater risk for developing dental caries (46%), which is consistent with previous reports.[6,7]
Individuals from lower socioeconomic status experience financial, social, and material disadvantages. The access to healthy environment, social resources such as medical and dental care is compromised. This, together with fatalistic beliefs about their health and lower perceived need for dental care, leads to neglected self-care, and lower utilization of preventive health services.[8,9,10] Socioeconomic status is such a robust finding that it is a “critical determinant of health” and has been emphasized to be included in planning interventions.[11,12] However, in India, access to dental care varies among children.[13]
Economic status has significant influences on a child's development. The income of parent or parents directly influences the quality of care and the quality of life a child has. Although parental employment will fulfill the basic needs of a child, nevertheless, when both parents work, they must seek nonparental care of some type including day-care, care by extended family, or self-care.[14] When both the parents are employed, they hardly find time to spare for their children and to look after their general health and specifically the oral health care.[15] In the present study, the children from families, where both parents were employed had increased caries prevalence, which was statistically significant for primary dentition (P = 0.0170) and the odds ratio showed higher risk for caries in permanent dentition. Hence, better attention should be paid to the child's oral health and the parents must try to strike a balance between work and providing care to their children.
Limitations of the study
As this is a questionnaire based study, the parents may try to under report the facts, which is the main drawback of questionnaire-based studies.
Only the representative population from different areas of the district was enrolled, and the entire population was not studied, as this is a cross-sectional study. Hence, a study with the inclusion of entire population should be taken up to assess the association of the working and socioeconomic factors of the parents on dental caries in their children.
CONCLUSION
The children of lower socioeconomic status and children with both the parents employed or working had increased the risk to dental caries. Efforts by the government and nongovernmental organizations are obligatory to implement programs at the school level to enhance oral and dental health care among children.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Amick B, Levine S, Tarlov A, Chapman D, editors. Society and Health. New York: Oxford University Press; 1995. pp. 18–22. [Google Scholar]
- 2.Ahmed S, Mistry M. Modern education and socio-economic change. J Arts Sci Commer. 2010;I:139–49. [Google Scholar]
- 3.Kumar N, Gupta N, Kishore J. Kuppuswamy's socioeconomic scale: Updating income ranges for the year 2012. Indian J Public Health. 2012;56:103–4. doi: 10.4103/0019-557X.96988. [DOI] [PubMed] [Google Scholar]
- 4.Klein H, Palmer CE, Knutson JW. Studies on dental caries. I. Dental status and dental needs of elementary school children. Public Health Rep. 1938;53:751–65. [Google Scholar]
- 5.Du MQ, Tai BJ, Jiang H, Lo EC, Fan MW, Bian Z. A two-year randomized clinical trial of chlorhexidine varnish on dental caries in Chinese preschool children. J Dent Res. 2006;85:557–9. doi: 10.1177/154405910608500615. [DOI] [PubMed] [Google Scholar]
- 6.Bali RK, Mathur VB, Talwar PP, Chanana HB. National Oral Health Survey and Fluoride Mapping 2002-2003 India. 1st ed. New Delhi: Dental Council of India and Ministry of Health and Family Welfare, Government of India; 2004. [Google Scholar]
- 7.Touger-Decker R, Mobley C. Academy of Nutrition and Dietetics. Position of the Academy of Nutrition and Dietetics: Oral health and nutrition. J Acad Nutr Diet. 2013;113:693–701. doi: 10.1016/j.jand.2013.03.001. [DOI] [PubMed] [Google Scholar]
- 8.Kaiser LL, Melgar-Quiñonez HR, Lamp CL, Johns MC, Sutherlin JM, Harwood JO. Food security and nutritional outcomes of preschool-age Mexican-American children. J Am Diet Assoc. 2002;102:924–9. doi: 10.1016/s0002-8223(02)90210-5. [DOI] [PubMed] [Google Scholar]
- 9.Vargas CM, Crall JJ, Schneider DA. Sociodemographic distribution of pediatric dental caries: NHANES III, 1988-1994. J Am Dent Assoc. 1998;129:1229–38. doi: 10.14219/jada.archive.1998.0420. [DOI] [PubMed] [Google Scholar]
- 10.Wardle J, Steptoe A. Socioeconomic differences in attitudes and beliefs about healthy lifestyles. J Epidemiol Community Health. 2003;57:440–3. doi: 10.1136/jech.57.6.440. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Chen M. Oral health of disadvantaged populations. In: Cohen L, Gift H, editors. Disease Prevention and Oral Health Promotion: Socio-Dental Sciences in Action. Copenhagen: Munksgaard; 1995. pp. 154–212. [Google Scholar]
- 12.Moses J, Rangeeth BN, Gurunathan D. Prevalence of dental caries, socio-economic status and treatment needs among 5 to 15 year old school going children of Chidambaram. J Clin Diagn Res. 2011;5:146–51. [Google Scholar]
- 13.Gambhir RS, Brar P, Singh G, Sofat A, Kakar H. Utilization of dental care: An Indian outlook. J Nat Sci Biol Med. 2013;4:292–7. doi: 10.4103/0976-9668.116972. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Mahesh Kumar P, Joseph T, Varma RB, Jayanthi M. Oral health status of 5 years and 12 years school going children in Chennai city – An epidemiological study. J Indian Soc Pedod Prev Dent. 2005;23:17–22. doi: 10.4103/0970-4388.16021. [DOI] [PubMed] [Google Scholar]
- 15.McMunn A, Kelly Y, Cable N, Bartley M. Maternal employment and child socio-emotional behaviour in the UK: Longitudinal evidence from the UK Millennium Cohort Study. J Epidemiol Community Health. 2012;66:e19. doi: 10.1136/jech.2010.109553. [DOI] [PubMed] [Google Scholar]