

Abstract
Purpose:
The purpose of this in vitro study was to compare four methods of root canal obturation in primary teeth using conventional radiography.
Materials and Methods:
A total of 96 root canals of primary molars were prepared and obturated with zinc oxide eugenol. Obturation methods compared were endodontic pressure syringe, insulin syringe, jiffy tube, and local anesthetic syringe. The root canal obturations were evaluated by conventional radiography for the length of obturation and presence of voids. The obtained data were analyzed using Chi-square test.
Results:
The results showed significant differences between the four groups for the length of obturation (P < 0.05). The endodontic pressure syringe showed the best results (98.5% optimal fillings) and jiffy tube showed the poor results (37.5% optimal fillings) for the length of obturation. The insulin syringe (79.2% optimal fillings) and local anesthetic syringe (66.7% optimal fillings) showed acceptable results for the length of root canal obturation. However, minor voids were present in all the four techniques used.
Conclusions:
Endodontic pressure syringe produced the best results in terms of length of obturation and controlling paste extrusion from the apical foramen. However, insulin syringe and local anesthetic syringe can be used as effective alternative methods.
Key words: Primary teeth, pulpectomy, root canal obturation, zinc oxide eugenol
INTRODUCTION
The main objective of pulp therapy in primary dentition is to retain each primary tooth as a fully functional component in the dental arch. This helps in proper mastication, phonation, swallowing, preservation of the space required for eruption of permanent teeth, and prevention of detrimental psychological effects due to loss of teeth.[1] Thus, Lewis and Law succinctly stated that, “The successful treatment of a pulpally involved tooth is to retain that tooth in a healthy condition so that it may fulfill its role as a useful component of the primary and young permanent dentition.”
Treatment of pulpally inflamed primary teeth in children presents a unique challenge to the dental clinician. Pulp diagnosis in the child is imprecise, as clinical symptoms do not correlate well with the histologic pulpal status. Age and behavior can compromise the reliability of pain as an indicator of the extent of pulp inflammation.[2] Pulp therapy in deciduous teeth is different in the sense that the medicaments used and the obturation technique used are to a large extent different from those of permanent teeth. The complex morphology of the root canal system in deciduous teeth makes it difficult to achieve proper cleansing by mechanical instrumentation and irrigation. This is achieved by careful cleaning and shaping followed by the complete obturation of the canal space. It has been observed that the general dentists and pedodontists differ in their treatment recommendations. Many a times, the treatment done remains incomplete either due to the lack of knowledge of the dentist or due to noncooperation on the part of the child.[3]
According to the Guidelines of the American Academy of Pediatric Dentistry, pulpectomy is indicated in primary teeth with carious pulp exposures, in which, following coronal pulp amputation, the radicular pulp exhibits clinical signs of hyperemia or evidence of necrosis of the radicular pulp with or without caries involvement.[4] The treatment consists of removing the pulp tissue associated with micro-organisms and debris from the canal and obturating with resorbable filling material. The mixing technique of the obturating material as well as the obturation method also influences the success rate.[5] The ultimate goal of endodontic obturation is to create a fluid-tight seal along the length of the root canal system from the coronal opening to the apical termination.[6] Several techniques have been used to fill the material into the root canals of primary teeth. An ideal filling technique should assure complete filling of the canal without overfill and with minimal or no voids.[5] Thus, the aim of this in vitro study was to compare and evaluate the effectiveness of four obturation methods; endodontic pressure syringe, insulin syringe, jiffy tube, and local anesthetic syringe for obturation of root canals of primary teeth.
MATERIALS AND METHODS
The present in vitro study was conducted in the Department of Pedodontics and Preventive Dentistry. The study protocol was approved by the Institutional Ethical Committee. Forty-eight extracted human primary maxillary and mandibular molars were collected from the Department of Pedodontics and Preventive Dentistry based on the following inclusion and exclusion criteria.[2,7]
Inclusion criteria
Exclusion criteria
Teeth with more than one-third of root resorption.
Teeth with signs of root canal obstruction.
Teeth which are grossly decayed and having root caries.
Method of allocation of data
Immediately following extraction, each tooth was placed in 10% formalin (Formaldehyde Solution, Spectrum Reagents and Chemicals Pvt. Ltd., Edayar, Cochin, Kerala, India). Teeth were prepared by removing all soft tissue remnants and then placed in normal saline (Sodium Chloride Injection IP, Punjab Formulations Ltd., Maharashtra, India) until use. Ninety-six primary maxillary and mandibular molar root canals were selected for the study. Root canals were equally and randomly divided into four groups [Figure 1] with 24 root canals per group.
Figure 1.

Teeth samples in four groups: Group 1, Group 2, Group 3, and Group 4
Group 1: Endodontic pressure syringe (Pulpdent, root canal pressure syringe).
Group 2: Insulin syringe (DispoVan).
Group 3: Jiffy tube (Waterpik).
Group 4: Local anesthetic syringe (disposable 2 ml syringe, DispoVan).
Method of study
For all the tooth samples, standard endodontic access to the pulp chamber was prepared using diamond round burs (Horico). All the root canals were checked for apical patency and root canal conditions by inserting a #10 K-file (Mani Co., Tokyo, Japan). All the root canals were prepared and filled by a single operator. First, the working length was recorded manually by direct visual examination as the length of #10 K-file at the apical foramen at −1 mm.[8] For the purpose of proper radiographic assessment, mesio-buccal and distal root canals were chosen for mandibular primary molars and mesio-buccal and disto-buccal root canals were chosen for maxillary primary molars. Root canals were instrumented manually with K-files [Figure 3a] initiated with size 15 K-file and canals were enlarged sequentially to size 30-35 K-file. In all the experimental groups, the canals were irrigated with normal saline. Next, the canals were dried with absorbent paper points (Diadent). After the preparations, the apical parts of the roots (from 1 mm below the cement-enamel junction) were covered with modeling wax (Golden Dental Products) to produce a halo space to serve as a collection area for any extruded canal filling material. The apical parts of the roots were then mounted in the center of cold-cured acrylic resin (DPI-RR Cold Cure, Acrylic Repair Material) blocks measuring 2 cm Χ 2 cm.
Figure 3.
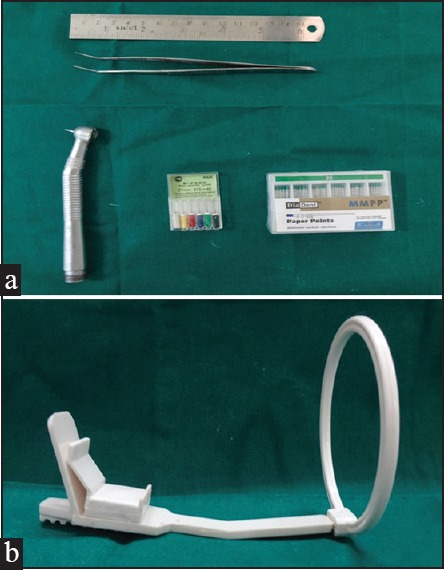
(a) Armamentarium. (b) Rinn XCP instrument for radiographic film positioning
Root canal obturation
The prepared root canals were filled with slow setting pure zinc oxide and eugenol (ZOE) paste (Deepak Enterprises) with four different methods [Figure 2]. To achieve a similar creamy consistency of ZOE, the paste was obtained by mixing one volume unit of powder with two volume units of liquid.[9]
Figure 2.
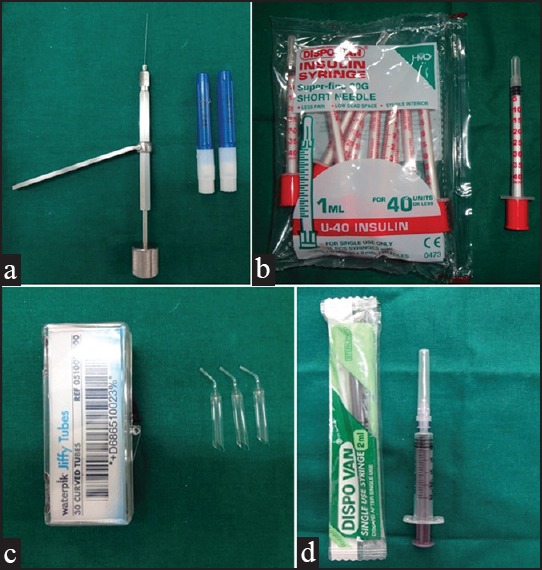
Four different obturation methods: (a) Endodontic pressure syringe. (b) Insulin syringe. (c) Jiffy tube. (d) Local anesthetic syringe
Group 1
Twenty-four prepared root canals were filled with ZOE paste mixed to a creamy consistency as described previously using an endodontic pressure syringe (Pulpdent, Root Canal Pressure Syringe) with a 30-gauge needle, according to the manufacturer's instructions. The mechanical nature of the pressure syringe (which operates by a screw mechanism) expressed the mixture through a 30-gauge needle. The needle was inserted into the root canal and using a slow, withdrawing-type of motion, the needle was withdrawn in 3 mm intervals with each quarter turn of the screw until the canal was visibly filled at the orifice.[10]
Group 2
Twenty-four prepared root canals were obturated with ZOE paste mixed to a creamy consistency as described previously using insulin syringe (needle; 30-gauge, 8 mm length; DispoVan). The homogeneous mixture of ZOE was loaded into the insulin syringe and the needle was inserted into the canal. The material was then pressed into the canal and while doing so, the needle was retrieved from the canal outward while continuing to press the material inside. Finally, at the orifice, more materials were pressed using a moist cotton pellet.[11]
Group 3
Twenty-four prepared root canals were filled with ZOE paste mixed to a creamy consistency as previously described using jiffy tube (Waterpik) according to the manufacturer's instructions. The standardized mixture of ZOE paste was back-loaded into the tube. The tube tip was placed into the root canal orifice and the material was pressed into the canal with a downward squeezing motion until the orifice appeared visibly filled.[10]
Group 4
Twenty-four prepared root canals were obturated using a local anesthetic syringe. A local anesthetic syringe (Disposable 2-ml syringe DispoVan, Hindustan Syringes and Medical Devices Ltd., New Delhi, India) with 27-gauge, 1.5-inch length needle was used. The needle was bent so as to get easy access up to the apical foramina for each of the root canals taking care that the length of the needle from tip to the bend was equal to the measured working length of the roots. Approximately, 1 ml of the material was loaded in the syringe, which was tapped on a solid surface, after fixing the piston keeping the needle side vertically upward till the bubbles entrapped get removed and the material reaches the orifice of the syringe. The needle was fixed and flow of the material was checked. The needle was inserted into the root canal right up to 1 mm short of apical foramina and the material was gently pushed into the root canal till the material was seen flowing out of the canal orifice. Now, the needle was gradually withdrawn while pushing the material till the needle reaches the pulp chamber.[12]
To control paste delivery in all the four groups, a rubber stop was placed around each instrument at a distance determined by preoperative measurements. In all the four groups, when the canal was assumed to be completely filled, a moist cotton pellet was used to lightly tamp the material into the canals. Next, the pulp chamber was filled with a thick mixture of ZOE.
Radiographic technique
To obtain accurate radiographs that would permit good visualization of tooth structure as well as reproducibility, the Rinn XCP [Figure 3b] instrument (Safe plus Panoramic X-Ray Positioner), radiographic parallelism, and standard exposure techniques were used. One postobturation intraoral periapical (IOPA) radiograph was made buccolingually for each sample in all the four groups using same X-ray unit (Kodak 2100 Intra-Oral X-ray System) and standardized kilovolts (60 kV), milliamperes (7 mA), and exposure time (0.320 ms) so that radiographic errors were minimized.
Radiographic evaluation
The radiographs were mounted on an X-ray view box for assessment. Two blinded, calibrated observers assessed the quality of the filled root canals, according to distance of the ZOE filling from the apex. They scored the obturation quality based on the following criteria as given by Coll and Sadrian:[13]
Under filling (score — 1): All canals filled more than 2 mm short of the apex.
Optimal filling (score — 2): Canals having zinc oxide eugenol ending at the radiographic apex or up to 2 mm short of apex.
Over filling (score — 3): Any canal showing zinc oxide eugenol outside the root apex.
Voids: Obturated root canals showing voids (presence/absence).
When disagreement arose during evaluations, final evaluations were determined by a third observer.
RESULTS
Data analysis was carried out using Statistical Package for Social Sciences (SPSS version 10.5, IBM Corporation software) package. The results for each parameter (numbers and percentages) for discrete data are presented in tables. Proportions were compared using Chi-square test of significance. The length of root canal obturation was expressed as under filling [Figure 4a], optimal filling [Figure 4b], and over filling [Figure 4c] along with presence or absence of voids and were subjected to appropriate statistical analysis. The “P” value was calculated. When P < 0.05, it was taken as significant. When P > 0.05, it was taken as not significant.
Figure 4.
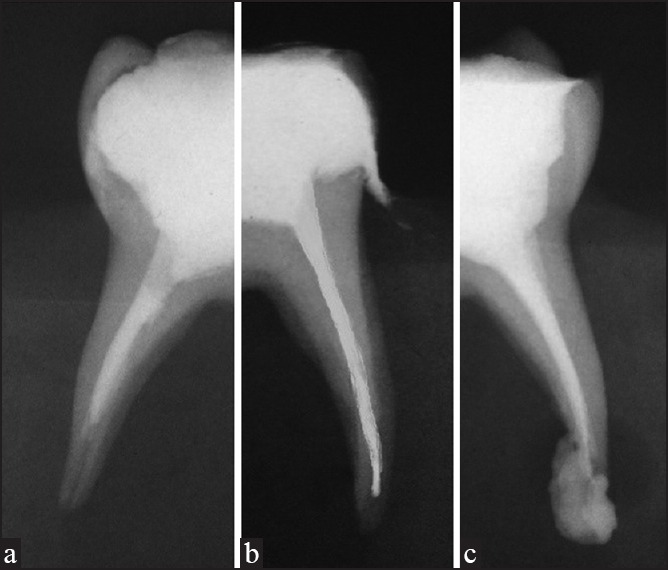
Intraoral periapical radiographs showing the quality of obturation. (a) Under fill. (b) Optimum fill. (c) Over fill
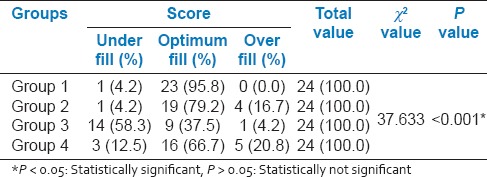
For the overall comparison of quality of root canal obturation, Chi-square test was used which detected significant differences (P < 0.001) between the four groups. Table 1 shows the frequencies of each root canal filling score in all four groups. The endodontic pressure syringe scored best (score — 2) for the length of root canal filling (95.8% optimal fillings) and the jiffy tube scored poor (37.5% optimal fillings). The insulin syringe (79.2% optimal fillings) and anesthetic syringe (66.7% optimal fillings) showed acceptable results for the length of root canal obturation.
Table 1.
Overall comparison between four groups for the quality of root canal obturation in primary molars
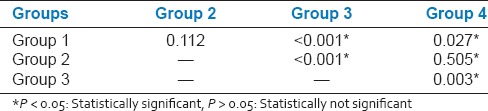
The results of paired comparisons between four experimental groups for the quality of root canal obturation in primary molars are shown in Table 2. The results indicate the following facts; statistically significant differences were found between endodontic pressure syringe and jiffy tube (P < 0.001), between endodontic pressure syringe and anesthetic syringe (P = 0.027), between insulin syringe and jiffy tube (P < 0.001), and between jiffy tube and anesthetic syringe (P = 0.003). However, no statistically significant differences were found between endodontic pressure syringe and insulin syringe (P = 0.112) and between insulin syringe and anesthetic syringe (P = 0.505).
Table 2.
Two-paired comparison between four groups for the quality of root canal obturation quality in primary molars
Radiographs were also assessed for the presence of minor voids in all the four groups and were graded as “presence” or “absence” of voids. One or two small voids were present in all the four groups studied. The frequency distribution of voids was more in local anesthetic syringe (45.8%) and insulin syringe (37.5%) compared to endodontic pressure syringe (29.1%) and jiffy tube (25%). However, the comparison done using Chi-square test showed no significant differences (P > 0.05) among the four groups for the presence/absence of voids.
DISCUSSION
Pulpectomy refers to the complete removal of irreversibly inflamed or necrotic coronal and radicular pulp tissue followed by filling with a resorbable material in either single or double appointments.[14] Various materials are used to obturate root canals of primary teeth. However, in the present in vitro study, ZOE paste was used because it is the most commonly used root canal filling material and many investigations have assessed its performance.[15] Several laboratory methods have been used to evaluate the quality of root canal filling, such as the penetration of dye/bacteria/radioisotopes, clearing techniques following tooth sectioning and radiographic assessment.[7] In the present study, the quality of root canal obturation was assessed by conventional IOPA radiography.
In the present study, endodontic pressure syringe performed the best with maximum number of optimal fillings (95.8%). Aylard and Johnson have also reported significantly better results with endodontic pressure syringe when compared with the mechanical syringe for obturating the curved root canals.[10] However, the endodontic pressure syringe was not significantly better than the tuberculin syringe or jiffy tube.[10] This was in contrast with the present study in which endodontic pressure syringe showed better results and statistically significant differences with jiffy tube (P < 0.001) and local anesthetic syringe (P < 0.027). The advantage of endodontic pressure syringe is the screw mechanism which generates pressure that helps in pushing the material into the root canals. However, few drawbacks are also associated with endodontic pressure syringe, namely difficulties in placing the rubber stop correctly and removing the needle, the need to clean and refill the hub of the syringe several times makes this method more complex and time consuming.[16]
In the present study, insulin syringe group showed 79.2% optimum fillings. However, no statistically significant differences were found when compared to endodontic pressure syringe (P = 0.112) and local anesthetic syringe (P = 0.505). However, it showed better results when compared to jiffy tube (P < 0.001). The insulin syringe showed fewer voids (37.5%) than local anesthetic syringe (45.8%). These findings were in agreement with the study conducted by Nagar et al.[11] Jiffy tube is a disposable cellulose acetate or plastic tube with a straight or curved end. In the present study, curved jiffy tube was used and it performed poorly (37.5% optimal fillings). The intergroup comparison with the other three techniques showed statistically significant differences (P < 0.05), a result consistent with the findings of Aylard and Johnson.[10]
In the present study, the quality of root canal obturation with the local anesthetic syringe group was inferior to that of endodontic pressure syringe group. However, the results were comparable to insulin syringe group, but no statistically significant differences (P = 0.505) were found. According to Memarpour et al., the quality of root canal filling with the local anesthetic syringe was inferior to that of the lentulospiral and NaviTip groups,[16] a result consistent with the findings of Peters et al.[17] Limited flexibility and thicker tip of the needle can make complete filling of root canals difficult.[18]
In the present study, all the techniques used to obturate the root canals led to voids in the filling material, a finding consistent with earlier reports.[7,19] However, there were no significant differences (P > 0.05) in voids among the four groups studied. However, the frequency of voids were more in local anesthetic syringe group (45.8%) and insulin syringe group (37.5%) when compared with endodontic pressure syringe group (29.1%) and jiffy tube group (25%). Dandashi et al. reported fewer voids with pressure syringe technique when compared to the lentulospiral, tuberculin syringe, and packing method.[7] However, Memarpour et al. found the highest frequency of voids (87%) with pressure syringe and packing groups.[16] The discrepancies in the results among the studies probably reflects differences in the type of teeth, sample size, needle thickness, and technique used to quantify voids and operator experience.[19] In the present study, the assessment of root canal obturation quality and voids were done by conventional IOPA radiography, which gave a two-dimensional view only. This can be the potential limitation of the study. Therefore, it is recommended to conduct in vivo studies with large sample size and long-term follow-up. It is also recommended to use digital radiography or cone-beam computed tomography to accurately assess the quality of root canal obturation.
CONCLUSIONS
Based on the results of the present in vitro study, the following conclusions can be made:
Endodontic pressure syringe produced the best results (95.8% optimal fillings) and jiffy tube produced poor results (37.5% optimal fillings) in terms of length of root canal obturation.
The insulin syringe (79.2% optimal fillings) and local anesthetic syringe (66.7% optimal fillings) showed acceptable results. However, small voids were present in all the four techniques used.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Ahmed HM. Pulpectomy procedures in primary molar teeth. Eur J Gen Dent. 2014;3:3–10. [Google Scholar]
- 2.Dummett CO, Kopel HM. Pediatric endodontics. In: Ingle JI, Bakland FK, editors. Endodontics. 5th ed. Hamilton: BC Decker Elsevier; 2002. pp. 861–902. [Google Scholar]
- 3.Togoo R, Nasim V, Zakirulla M, Yaseen S. Knowledge and practice of pulp therapy in deciduous teeth among general dental practitioners in Saudi Arabia. Ann Med Health Sci Res. 2012;2:119–23. doi: 10.4103/2141-9248.105657. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Moskovitz M, Sammara E, Holan G. Success rate of root canal treatment in primary molars. J Dent. 2005;33:41–7. doi: 10.1016/j.jdent.2004.07.009. [DOI] [PubMed] [Google Scholar]
- 5.Mahajan N, Bansal A. Various obturation methods used in deciduous teeth. Int J Med Dent Sci. 2015;4:708–13. [Google Scholar]
- 6.Garcia-Godoy F. Evaluation of an iodoform paste in root canal therapy for infected primary teeth. ASDC J Dent Child. 1987;54:30–4. [PubMed] [Google Scholar]
- 7.Dandashi MB, Nazif MM, Zullo T, Elliott MA, Schneider LG, Czonstkowsky M. An in vitro comparison of three endodontic techniques for primary incisors. Pediatr Dent. 1993;15:254–6. [PubMed] [Google Scholar]
- 8.Sigurdsson A, Stancill R, Madison S. Intracanal placement of Ca(OH)2: A comparison of techniques. J Endod. 1992;18:367–70. doi: 10.1016/s0099-2399(06)81220-3. [DOI] [PubMed] [Google Scholar]
- 9.Bawazir OA, Salama FS. Apical microleakage of primary teeth root canal filling materials. J Dent Child (Chic) 2007;74:46–51. [PubMed] [Google Scholar]
- 10.Aylard SR, Johnson R. Assessment of filling techniques for primary teeth. Pediatr Dent. 1987;9:195–8. [PubMed] [Google Scholar]
- 11.Nagar P, Araali V, Ninawe N. An alternative obturating technique using insulin syringe delivery system to traditional reamer: An in vivo study. J Dent Oral Biosci. 2011;2:7–19. [Google Scholar]
- 12.Bhandari SK, Anita A, Prajapati U. Root canal obturation of primary teeth: Disposable injection technique. J Indian Soc Pedod Prev Dent. 2012;30:13–8. doi: 10.4103/0970-4388.95566. [DOI] [PubMed] [Google Scholar]
- 13.Coll JA, Sadrian R. Predicting pulpectomy success and its relationship to exfoliation and succedaneous dentition. Pediatr Dent. 1996;18:57–63. [PubMed] [Google Scholar]
- 14.Allen KR. Endodontic treatment of primary teeth. Aust Dent J. 1979;24:347–51. doi: 10.1111/j.1834-7819.1979.tb05807.x. [DOI] [PubMed] [Google Scholar]
- 15.Kubota K, Golden BE, Penugonda B. Root canal filling materials for primary teeth: A review of the literature. ASDC J Dent Child. 1992;59:225–7. [PubMed] [Google Scholar]
- 16.Memarpour M, Shahidi S, Meshki R. Comparison of different obturation techniques for primary molars by digital radiography. Pediatr Dent. 2013;35:236–40. [PubMed] [Google Scholar]
- 17.Peters CI, Koka RS, Highsmith S, Peters OA. Calcium hydroxide dressings using different preparation and application modes: Density and dissolution by simulated tissue pressure. Int Endod J. 2005;38:889–95. doi: 10.1111/j.1365-2591.2005.01035.x. [DOI] [PubMed] [Google Scholar]
- 18.Torres CP, Apicella MJ, Yancich PP, Parker MH. Intracanal placement of calcium hydroxide: A comparison of techniques, revisited. J Endod. 2004;30:225–7. doi: 10.1097/00004770-200404000-00010. [DOI] [PubMed] [Google Scholar]
- 19.Guelmann M, McEachern M, Turner C. Pulpectomies in primary incisors using three delivery systems: An in vitro study. J Clin Pediatr Dent. 2004;28:323–6. doi: 10.17796/jcpd.28.4.j634167443m061n3. [DOI] [PubMed] [Google Scholar]