

Abstract
Background
Various surgical strategies have been described for the treatment of cubital tunnel syndrome, including medial epicondylectomy. This aims to decompress the ulnar nerve and allow a ‘mini anterior transposition’. The major concern over medial epicondylectomy is the potential for postoperative iatrogenic valgus instability.
Methods
We utilized a surgical landmark for medial epicondylectomy based on the medial aspect of the ulnar nerve with the elbow in 90° of flexion in 12 cadaveric upper limbs. The size of the resultant fragment was measured and, subsequently, the medial collateral ligament was dissected and the elbow stressed to assess its integrity.
Results
This technique resulted in the excision of a fragment of mean width 8 mm (range 6 mm to 11 mm) and allowed the ulnar nerve to smoothly translate anteriorly in flexion. The anterior band of the ulnar collateral ligament was macroscopically preserved in all cases and there was no valgus instability.
Conclusions
The medial border of the ulnar nerve is a simple, safe and reliable surgical landmark for medial epicondylectomy. This technique offers advantages over other described methods of assessing the location at which to perform a medial epicondylectomy.
Keywords: Cubital tunnel syndrome, surgery, medial epicondylectomy, technique
Introduction
Cubital tunnel syndrome is the second most common entrapment neuropathy [1]. Several surgical strategies exist if non-operative treatments have failed: in situ decompression (ISD), in situ decompression and medial epicondylectomy (ISD and ME) and anterior transposition (which may be submuscular, intramuscular or subcutaneous). Multiple review articles and meta-analyses demonstrate largely equivalent results with these techniques [2–6]. The most serious potential complication after ME is iatrogenic valgus instability as a result of resection of the anterior band of the ulnar collateral ligament (UCL). To avoid this complication, a partial ME has been described that preserves the UCL [7]. The recommended amount of bone to be excised has varied: on the basis of an anatomical study, it was recommended to excise less than 20% of the epicondyle, whereas other studies have recommended dissecting the ligament and making an osteotomy level with its medial margin or removing a fragment of bone of a specific size [7–13]. During surgery, it is time-consuming to dissect out the entire width of the epicondyle and perform measurements to plan the osteotomy based on the percentage of epicondyle to be removed. The size of the medial epicondyle is subject to significant variation [12] and therefore it is not reliable to recommend the removal of a certain thickness of bone in all cases. It is somewhat technically difficult and time consuming to dissect the flexor pronator mass from the anterior band of the UCL so as to make the osteotomy at the medial edge of the ligament origin. Therefore, it would be beneficial to use a simple landmark that allows an osteotomy to be made that reliably allows anterior translation on flexion at the same time as preserving the ligament. We hypothesized that an osteotomy level with the medial border of the ulnar nerve in the sagittal plane would satisfy these requirements.
Materials and methods
Local ethics committee approval was obtained. Twelve thawed, paired previously fresh frozen cadaveric upper limbs that had not undergone any prior surgery around the elbow were utilized (two male, four female cadavers; mean age at death 82.8 years, range 70 years to 91 years). Each elbow was examined for the presence of a subluxating ulnar nerve by palpation prior to the incision when bringing the elbow into full flexion. A posteromedial incision was the performed and an ulnar nerve release was performed from the medial intermuscular septum up to and including the fascia overlying the two heads of the flexor carpi ulnaris (FCU). The motor branches to FCU were preserved. All dissection was performed on the dorsomedial surface of the nerve, whereas the remainder of its bed was left undisturbed. A longitudinal incision was performed through the flexor pronator origin at the medial epicondyle. The insertion was reflected subperiosteally both anteriorly and posteriorly until level with the medial border of the nerve in 90° of elbow flexion. The nerve was protected and an osteotomy was performed at the medial edge of the nerve (Fig.1). The resection plane was sagittal, specifically avoiding aiming lateral to this plane. Once the osteotomy had been performed, the width of the osteotomized fragment was measured (Fig. 2). The anterior band of the UCL was then dissected both at its humeral insertion and also anterior and posterior to it (Fig. 3). In this way, the thickness of the ligament could be assessed and the articular surfaces could be visualized when performing a valgus stress test with the elbow in 30° of flexion and the forearm supinated (Fig. 4). Additionally, the osteotomized fragment was assessed for the presence of any fibres of the UCL attached to it. The flexor pronator mass was sutured to the epicondyle using simple absorbable sutures. The elbow was then taken from full extension to full flexion and the excursion of the ulnar nerve was visualized. The epicondylectomy was considered to be adequate if it smoothly translated anterior to the axis of rotation on flexion and returned posterior to the axis of rotation on extension.
Fig. 1.

Diagram showing a posterior view of an elbow in 90° flexion, illustrating the location of the osteotomy.
Fig. 2.
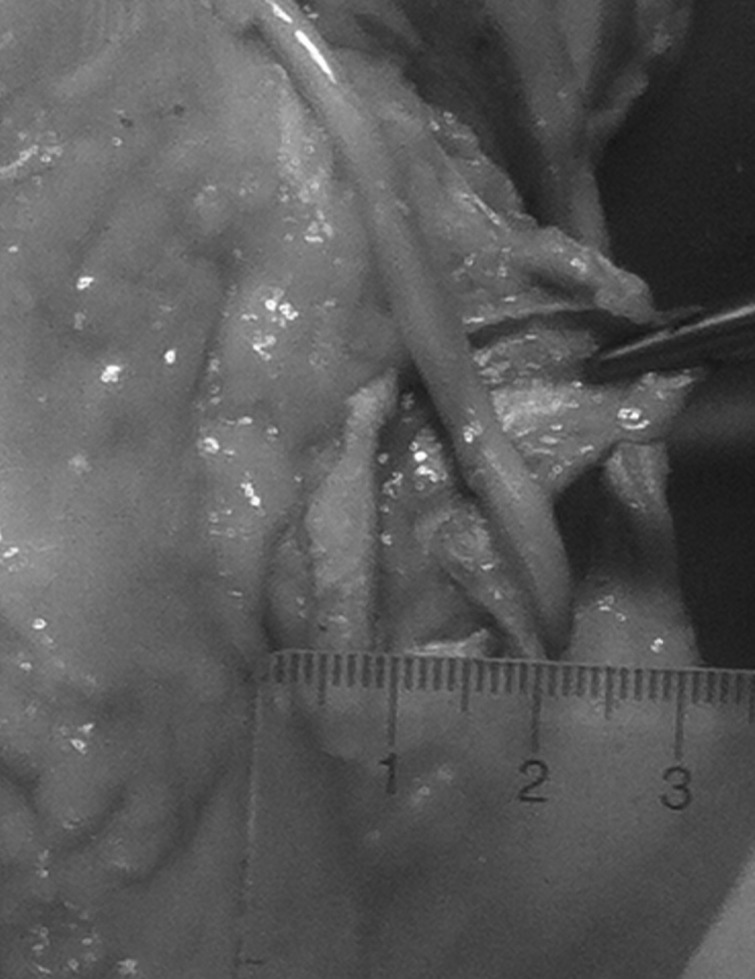
Measurement of the size of the osteotomy fragment.
Fig. 3.
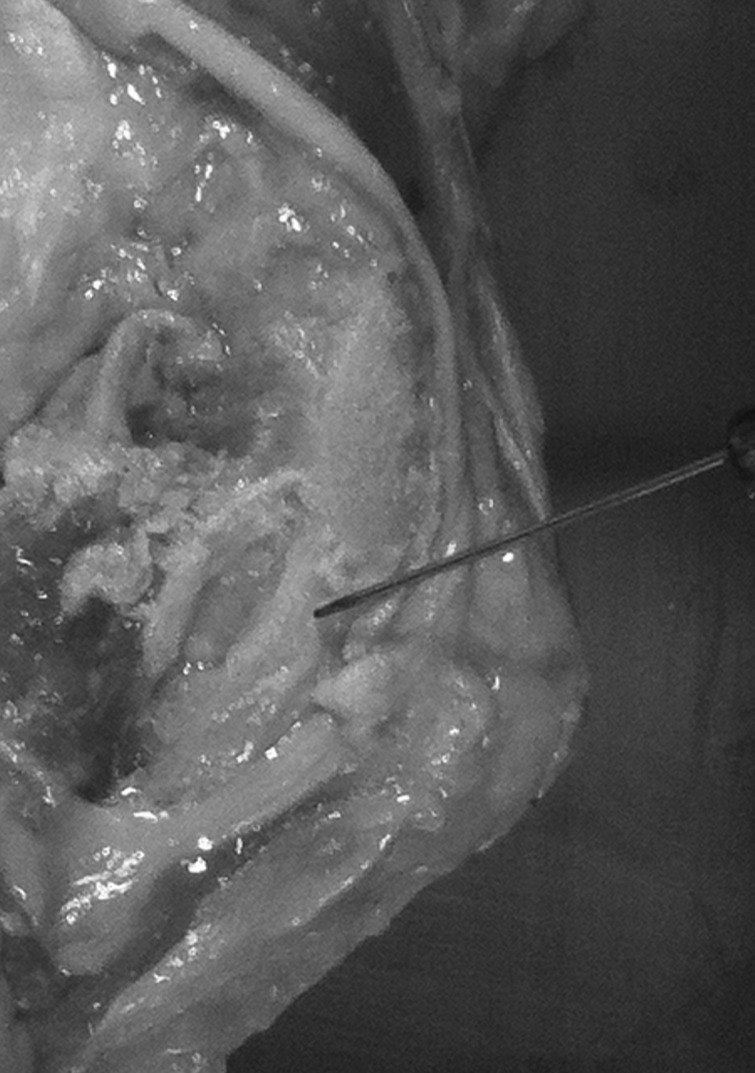
Location of the anterior band of the ulnar collateral ligament in relation to the osteotomy.
Fig. 4.

Anterior band of the ulnar collateral ligament after dissection.
Results
There was no evidence of ulnar nerve subluxation is any of the specimens prior to the incision. The mean (SD) width of the bone resected was 8 mm (1.33 mm) (range 6 mm to 11 mm). In all 12 cases, a stout anterior band of UCL was present after the epicondylectomy had been performed. There was no evidence of valgus instability. None of the osteotomized fragments had any visible fibres of the UCL attached to them. Once the flexor pronator origin had been replaced, the ulnar nerve was able to smoothly move anteriorly and posteriorly with flexion and extension in all cases. No kinking or entrapment of the nerve occurred during range of motion.
Discussion
Multiple options exist for the surgical treatment of cubital tunnel syndrome. The rationale for ISD is that, on flexion, the shape of the cubital tunnel changes and this leads to neurological compression. Because of its high success rate and simplicity, ISD is usually the procedure of choice [14]. It is not generally recommended to perform ISD if the floor of the cubital tunnel is abnormal or if the ulnar nerve is unstable or in the presence of significant cubitus valgus and, in these situations, ME or anterior transposition is favoured. Anterior transposition acknowledges that the ulnar nerve lies posterior to the axis of rotation of the elbow and therefore it stretches during flexion. By rerouting the nerve anterior to the axis of rotation, the traction forces on the nerve are neutralized [15]. The major concern over anterior transposition is that the significant dissection required may jeopardize the blood supply to the nerve [16,17]. ISD and ME decompresses the cubital tunnel, as well as allowing a ‘mini anterior transposition’, enabling the nerve to slide slightly anterior without excessive dissection or devascularization [18]. Concerns about ME are pain at the site of the osteotomy, vulnerability of the ulnar nerve after resection, weakness as a result of detachment of the flexor pronator mass and, in particular, the potential for instability of the elbow as a result of release of the anterior band of the UCL. King and Morgan first described ME with the aim of completely excising the epicondyle and some of the medial supracondylar ridge [19]. In an anatomical study, O’Driscoll et al. estimated that only 20% of the width of the ME could be resected without violating the ligament [12]. The risk of clinical valgus instability after ME is low, although the radiological incidence is higher [1,8,14]. This may be a result of the inherent stability of the elbow and also because, even when the aim of surgery is a complete medial epicondylectomy, this is often not actually performed [8,14]. Although there is limited evidence that a larger bony resection yields superior clinical results [18], an incomplete epicondylectomy is an effective technique [8–11,13,14,20–23]. A subtotal (partial) epicondylectomy was first described by Kaempfe and Farbach [7]. Subsequently, the description of what constitutes a partial epicondylectomy has varied: Amako et al. defined a partial epicondylectomy as one in which >40% of the epicondyle was excised [8]. If <20% was excised, it was termed a minimal epicondylectomy. Other studies have dissected the anterior band of the UCL and performed the osteotomy at its medial margin [14,21,24]. An alternative description is to excise a fragment of a particular size; this is variable, ranging from 2 mm to 8 mm [7–11,13].
Because of the disadvantages of the various described techniques to elect a site of bony resection, we have investigated the efficacy and safety of a method utilizing the ulnar nerve itself as a landmark in 90° of elbow flexion. This position of flexion was selected because it is convenient for performing ISD and ME in both the supine and lateral positions. In the usual situation of electing to perform a ME (such as an unstable nerve, an abnormality of the floor of the tunnel or revision surgery), allowing the nerve to translate smoothly anteriorly on flexion is a fundamental requirement of ME. We consider that excising a fragment more medial than the medial border of the ulnar nerve would not allow a ‘mini anterior transposition’. Although the location of the ulnar nerve is affected by the degree of flexion (most significant with an unstable nerve), we have demonstrated that this technique allows for smooth anterior and posterior translation of the nerve with elbow flexion and extension, and also that this should apply equally to both stable and unstable nerves. However, in the present study, none of the cadaveric specimens had evidence of ulnar nerve instability prior to the procedure. Although the number of specimens utilized in the present study is small and thus may not account for all anatomic variations, it is comparable to other similar studies [12]. The size of the fragment created using this technique is at the upper end of the spectrum of that of the described partial epicondylectomies. We did not compare the width of the osteotomized fragment with the width of the residual medial epicondyle. Amako et al. noted that, after a minimal medial epicondylectomy (<20%), no nerve could be subluxed anteriorly, whereas, after a partial epicondylectomy (>40%), all of it could [8]. Therefore, it is likely that the resection created by this technique was >40% of the width of the medial epicondyle. Despite the size of the excised fragment using the described technique, a stout anterior band of UCL was always present. It may be that a small percentage of the ligament was resected, although this would appear to be clinically insignificant. Because the ligament lies anterior and inferior on the epicondyle, an oblique osteotomy (between the coronal and sagittal planes) was recommended by O’Driscoll et al. [12]. Although we avoided resection lateral to the sagittal plane, a potential modification of our technique would be to aim the osteotome medial to the sagittal plane. We elected not to do this here because it would have been difficult to standardize the plane of the osteotomy. Our results suggest that making an osteotomy level with the medial border of the ulnar nerve is a reliable and safe method for performing a ME that allows anterior translation of the ulnar nerve in flexion at the same time as preserving the anterior band of the ulnar collateral ligament.
Acknowledgements
We thank the Vesalius Centre and the Centre for Comparative and Clinical Anatomy at the University of Bristol. IRB/Ethics committee: Study Number 08/H0106/143; NRES Committee Southwest-Central Bristol.
Conflicts of interest
None declared
Level of evidence
Basic science study; anatomic study; cadaver model
References
- 1.Feindel W, Stratford J. Cubital tunnel compression in tardy ulnar palsy. Can Med Assoc J 1958; 78: 351–3. [PMC free article] [PubMed] [Google Scholar]
- 2.Bartels RH, Menovsky T, Van Overbeeke JJ, Verhagen WI. Surgical management of ulnar nerve compression at the elbow: an analysis of the literature. J Neurosurg 1998; 89: 722–7. [DOI] [PubMed] [Google Scholar]
- 3.Dellon AL. Review of treatment results for ulnar nerve entrapment at the elbow. J Hand Surg Am 1989; 14: 688–700. [DOI] [PubMed] [Google Scholar]
- 4.Geutjens GG, Langstaff RJ, Smith NJ, Jefferson D, Howell CJ, Barton NJ. Medial epicondylectomy or ulnar-nerve transposition for ulnar neuropathy at the elbow? J Bone Joint Surg Br 1996; 78: 777–9. [PubMed] [Google Scholar]
- 5.Mowlavi A, Andrews K, Lille S, Verhulst S, Zook EG, Milner S. The management of cubital tunnel syndrome: a meta-analysis of clinical studies. Plast Reconstr Surg 2000; 106: 327–34. [DOI] [PubMed] [Google Scholar]
- 6.Palmer BA, Hughes TB. Cubital tunnel syndrome. J Hand Surg Am 2010; 35: 153–63. [DOI] [PubMed] [Google Scholar]
- 7.Kaempffe FA, Farbach J. A modified surgical procedure for cubital tunnel syndrome: partial medial epicondylectomy. J Hand Surg Am 1998; 23: 492–9. [DOI] [PubMed] [Google Scholar]
- 8.Amako M, Nemoto K, Kawaguchi M, Kato N, Arino H, Fujikawa K. Comparison between partial and minimal medial epicondylectomy combined with decompression for the treatment of cubital tunnel syndrome. J Hand Surg Am 2000; 25: 1043–50. [DOI] [PubMed] [Google Scholar]
- 9.Efstathopoulos DG, Themistocleous GS, Papagelopoulos PJ, Chloros GD, Gerostathopoulos NE, Soucacos PN. Outcome of partial medial epicondylectomy for cubital tunnel syndrome. Clin Orthop Relat Res 2006; 444: 134–9. [DOI] [PubMed] [Google Scholar]
- 10.Kim KW, Lee HJ, Rhee SH, Baek GH. Minimal epicondylectomy improves neurologic deficits in moderate to severe cubital tunnel syndrome. Clin Orthop Relat Res 2012; 470: 1405–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Muermans S, De Smet L. Partial medial epicondylectomy for cubital tunnel syndrome: outcome and complications. J Shoulder Elbow Surg 2002; 11: 248–52. [DOI] [PubMed] [Google Scholar]
- 12.O’Driscoll SW, Jaloszynski R, Morrey BF, An K-N. Origin of the medial ulnar collateral ligament. J Hand Surg Am 1992; 17: 164–8. [DOI] [PubMed] [Google Scholar]
- 13.Osterman AL, Spiess AM. Medial epicondylectomy. Hand Clin 2007; 23: 329–37. [DOI] [PubMed] [Google Scholar]
- 14.Heithoff SJ. Cubital tunnel syndrome does not require transposition of the ulnar nerve. J Hand Surg Am 1999; 24: 898–905. [DOI] [PubMed] [Google Scholar]
- 15.Kleinman WB. Cubital tunnel syndrome: anterior transposition as a logical approach to complete nerve decompression. J Hand Surg Am 1999; 24: 886–97. [DOI] [PubMed] [Google Scholar]
- 16.Ogata K, Manske PR, Lesker PA. The effect of surgical dissection on regional blood flow to the ulnar nerve in the cubital tunnel. Clin Orthop Relat Res 1985; 193: 195–8. [PubMed] [Google Scholar]
- 17.Prevel CD, Matloub HS, Ye Z, Sanger JR, Yousif NJ. The extrinsic blood supply of the ulnar nerve at the elbow: an anatomic study. J Hand Surg Am 1993; 18: 433–8. [DOI] [PubMed] [Google Scholar]
- 18.Heithoff SJ, Millender LH, Nalebuff EA, Petruska AJ., Jr Medial epicondylectomy for the treatment of ulnar nerve compression at the elbow. J Hand Surg Am 1990; 15: 22–9. [DOI] [PubMed] [Google Scholar]
- 19.King T, Morgan FP. Late results of removing the medial humeral epicondyle for traumatic ulnar neuritis. J Bone Joint Surg Br 1959; 41B: 51–5. [DOI] [PubMed] [Google Scholar]
- 20.Baek GH, Kwon BC, Chung MS. Comparative study between minimal medial epicondylectomy and anterior subcutaneous transposition of the ulnar nerve for cubital tunnel syndrome. J Shoulder Elbow Surg 2006; 15: 609–13. [DOI] [PubMed] [Google Scholar]
- 21.Gobel F, Musgrave DS, Vardakas DG, Vogt MT, Sotereanos DG. Minimal medial epicondylectomy and decompression for cubital tunnel syndrome. Clin Orthop Relat Res 2001; 393: 228–36. [DOI] [PubMed] [Google Scholar]
- 22.Schnabl SM, Kisslinger F, Schramm A, et al. Subjective outcome, neurophysiological investigations, postoperative complications and recurrence rate of partial medial epicondylectomy in cubital tunnel syndrome. Arch Orthop Trauma Surg 2011; 131: 1027–33. [DOI] [PubMed] [Google Scholar]
- 23.Schnabl SM, Kisslinger F, Schramm A, et al. Objective outcome of partial medial epicondylectomy in cubital tunnel syndrome. Arch Orthop Trauma Surg 2010; 130: 1549–56. [DOI] [PubMed] [Google Scholar]
- 24.Froimson AI, Anouchi YS, Seitz WH, Jr, Winsberg DD. Ulnar nerve decompression with medial epicondylectomy for neuropathy at the elbow. Clin Orthop Relat Res 1991; 265: 200–6. [PubMed] [Google Scholar]