

Abstract
The number of cases of coccidioidomycosis and associated hospitalizations increased in California during 2000–2013. During that period, a total of 1,098 death records listed coccidioidomycosis as a cause, averaging 78 deaths annually (range: 43–108). The death rate peaked in 2006 and was significantly higher among males than among females, among African American patients than among white patients, and among residents of the coccidioidomycosis–endemic region of California than among residents of the less endemic regions (p<0.001). A higher death rate was associated with increasing age and was highest (8.8 per 1 million population) among adults aged ≥75 years. Of coccidioidomycosis-associated deaths, 31.9% had a contributing cause of death of severe/disseminated disease, 31.8% of unspecified -coccidioidomycosis, and 28.3% of pulmonary unspecified coccidioidomycosis, per International Classification of Diseases codes. Diabetes was a contributing cause in 19.3% of deaths, and other immunocompromising conditions were a contributing cause in 15.9% of deaths. Populations at higher risk for coccidioidomycosis--associated deaths are similar to those at higher risk for coccidioidomycosis-associated hospitalizations and infection. Awareness for coccidioidomycosis among these groups and their providers is important for proper diagnosis and care.
Coccidioidomycosis is primarily a respiratory infection caused by inhaling spores of Coccidioides fungi, which are endemic in dirt and soil of some areas of the southwestern United States.1,2 Approximately 40% of people who are infected develop symptoms, and approximately 1% develop disseminated disease.3,4 Severe disease is rare, but can be fatal. A review of 3,089 coccidioidomycosis-associated deaths in the United States during 1990–2008 found that California had the most deaths (n=1,451, 47.0%).5 The objective of our study was to describe the epidemiology of coccidioidomycosis-associated deaths in California from 2000 through 2013, to identify potential demographic and clinical risk factors for death, and to describe how they compare with risk factors for infection and hospitalization. Because the rates of new infections and initial hospitalizations of coccidioidomycosis increased in California during 2000–2011,6–9 we also sought to learn whether or not coccidioidomycosis-associated deaths increased during those years.
METHODS
We reviewed California multiple-cause-of-death files, a database of resident death certificates, to identify coccidioidomycosis-associated deaths, which we defined as deaths (1) during the study period, January 1, 2000, through December 31, 2013; and (2) with an underlying or contributing cause-of-death diagnosis code for coccidioidomycosis (International Classification of Diseases, 10th Revision [ICD-10] B38.0–B38.9).10 Separately, we analyzed data on coccidioidomycosis-associated cases and hospitalizations in California during 2000–2013. We obtained these data from the California Department of Public Health's coccidioidomycosis surveillance system, a database of provider and laboratorian reports of confirmed coccidioidomycosis cases among California residents. We reviewed data on hospitalized patients from the California Patient Discharge Dataset, which contains administrative inpatient data reported by all California nonfederal hospitals.11 We extracted hospitalization data on all patients whose records indicated a primary or secondary discharge diagnosis code for coccidioidomycosis.9
We calculated annual case counts and rates by year of death, initial hospitalization admission, or symptom onset, and we stratified cases by sex, age group, race/ethnicity, and region of patient residence (endemic or less endemic). We defined the endemic region in California to include Fresno, Kern, Kings, Madera, San Luis Obispo, and Tulare counties, which had annual incidence rates from 2001–2013 that were higher than the overall state rate.10,11 We defined the less endemic region of the state to include all other counties. We calculated death rates per 1 million population and incidence rates and initial hospitalization rates per 100,000 population by using population estimates from the California Department of Finance based on the 2010 U.S. Census.12,13 We age-adjusted rates to the 2000 U.S. standard population. For each dataset, we used Poisson regression to calculate bivariate relative risks (RRs) for sex, race/ethnicity, and region of residence. We then calculated RRs for race/ethnicity, controlling for sex and age group (<55 and ≥55 years). We considered p<0.05 to be statistically significant. We performed all analyses using SAS® version 9.4.14
We reviewed underlying and contributing causes of death listed on death certificates to identify the types of coccidioidomycosis and concurrent conditions associated with death. Types of coccidioidomycosis consisted of mutually exclusive categories ranked as follows: severe/disseminated (meningitis [ICD-10 B38.4]; cutaneous [ICD-10 B38.3], or disseminated [ICD-10 B38.7]); unspecified (other [ICD-10 B38.8]); pulmonary unspecified (chronic pulmonary [ICD-10 B38.1] or unspecified pulmonary [ICD-10 B38.2]); or acute pulmonary disease (ICD-10 B38.0). We identified death records with a diagnosis of diabetes (ICD-10 E08–E14) and other immunocompromising conditions, including malignant neoplasm, human immunodeficiency virus (HIV), rheumatologic disease, disorders of the blood or immune system, organ transplant, or severe malnutrition (ICD-10: C00–C797, C7A, D37–D48, B20–B24, M05–M06, M08, M12.0, M32–M36, M45–M49, L40.54, L40.59, D80–D89, D60, D61, D70–D72, T96, Z94, C80.2, D47.Z1, D89.81, and E40–E43).
RESULTS
During 2000–2013, a total of 1,098 coccidioidomycosis-associated deaths were recorded in California, yielding an average of 78 deaths (range: 43–108) annually. The mean annual age-adjusted death rate was 2.2 deaths per 1 million population (crude rate = 2.2 deaths per 1 million population) (Table). The number and rate of deaths peaked in 2006 (n=108 or 3.1 per 1 million population) and again in 2011 (n=101 or 2.7 per 1 million population). During the study period, a total of 39,201 cases and 18,521 hospitalized patients were reported; incidence rates increased from 2.4 to 8.5 per 100,000 population and hospitalization rates increased from 2.4 to 3.4 per 100,000 population, with both peaking in 2011 (Figure).
Table.
Characteristics of coccidioidomycosis-associated deaths, hospitalized patients, and case patients, California, 2000–2013a
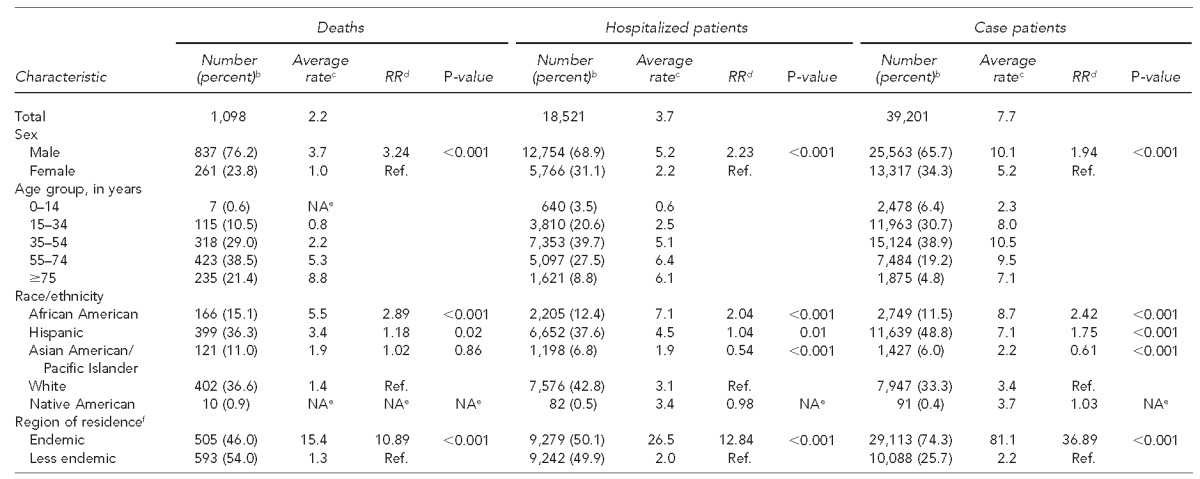
Data sources: Death data: State of California, California Department of Public Health. Multiple cause of death files, 2000–2013. Sacramento (CA): California Department of Public Health; 2013. Hospitalization data: State of California, Office of Statewide Health Planning and Development. Inpatient hospital discharge data set. Sacramento (CA): State of California, Office of Statewide Health Planning and Development; 2015. Case-patient data: California Department of Public Health's coccidioidomycosis surveillance dataset.
bPercentages may not total to 100 because of rounding.
cAverage annual rates per 1 million population for death and per 100,000 population for hospitalized patients and case patients. Crude rates reported for age group. All other rates were age-adjusted to the 2000 U.S. standard population.
dRR calculated by Poisson regression
eBecause of small numbers, annual rates and RRs were not calculated.
fThe endemic region was defined as counties with annual case rates from the previous 13 years that were higher than the state rates of California (Fresno, Kern, Kings, Madera, San Luis Obispo, and Tulare counties). The less endemic region was defined as all other California counties.
RR = relative risk
Ref. = reference group
NA = not available or not applicable
Figure.
Number of deaths and age-adjusted ratesa of deaths, initial hospitalizations, and case patients with coccidioidomycosis, by year, California, 2000 through 2013b

aRates per 1 million population for deaths and per 100,000 population for hospitalizations and patients with coccidioidomycosis. Rates were age-adjusted to the 2000 U.S. standard population.
bData sources: Death data: State of California, California Department of Public Health. Multiple cause of death files, 2000–2013. Sacramento (CA): California Department of Public Health; 2013. Hospitalization data: State of California, Office of Statewide Health Planning and Development. Inpatient hospital discharge data set. Sacramento (CA): State of California, Office of Statewide Health Planning and Development; 2015. Case-patient data: California Department of Public Health's coccidioidomycosis surveillance dataset.
The average coccidioidomycosis death rate per 1 million population was significantly higher among males (rate = 3.7, RR53.24, p<0.001) than among females (rate = 1.0), among African American (rate = 5.5, RR=2.89, p<0.001) or Hispanic (rate = 3.4, RR=1.18, p=0.02) patients than among white patients (rate=1.4), and among residents of the endemic region (rate = 15.4, RR=10.89, p<0.001) than among residents of the less endemic region (rate = 1.3) (Table). Controlling for sex and age group, the RRs for African American and Hispanic patients compared with white patients were 3.82 and 1.99 for deaths, 2.53 and 1.87 for case patients, and 2.29 and 1.28 for hospitalized patients (all p<0.001). Crude death rates generally increased with increasing age, with the highest death rate (8.8 per 1 million population) among those aged ≥75 years.
Of the 1,098 coccidioidomycosis-associated deaths, 350 (31.9%) had a contributing cause of death of severe/disseminated disease, 349 (31.8%) of unspecified coccidioidomycosis, 311 (28.3%) of pulmonary unspecified coccidioidomycosis, and 88 (8.0%) of acute pulmonary disease. Coccidioidal meningitis, a type of severe/disseminated disease, was listed as a cause of death on 120 of 1,098 (10.9%) death certificates.
Of the 1,098 deaths, 212 (19.3%) had diabetes as a contributing cause and 175 (15.9%) had other immunocompromising conditions, of which the most common were malignant neoplasm (93/1,098, 8.5%) and HIV (33/1,098, 3.0%).
DISCUSSION
During 2000–2013, California coccidioidomycosis--associated death rates, incidence rates, and hospitalization rates fluctuated; death rates peaked in 2006 and incidence and hospitalization rates peaked in 2011. Although we do not know what caused the decrease after 2011, it could be related to the California drought, which began in fall 2011. Coccidioides requires moist soil to grow.15
The death records show that death in California could occur in patients with any type of coccidioidomycosis, including acute pulmonary disease, although, not surprisingly, severe/disseminated (31.9%), including meningeal (10.9%), coccidioidomycosis comprises a substantial proportion of coccidioidomycosis-associated deaths. Patients with diabetes and other -immunocompromising conditions comprised only about 34% of those who died, leaving a majority of coccidioidomycosis-associated deaths without a known underlying contributing cause.
Similar to our findings, the findings of a national study of coccidioidomycosis-associated deaths during 1990–2008 found higher death rates among males than among females and among older age groups than among younger age groups.8 The higher death and hospitalization rates among older age groups could be related to an increase in the number of comorbid conditions and a weakened immune system in older adults.16,17 The national study of coccidioidomycosis-associated deaths reported the highest death rates among Native American and Hispanic patients; however, our study found the highest rates among African American patients, a group with increased risk for severe coccidioidomycosis.18,19
Limitations
The death, case-patient, and hospitalization datasets did not share enough personal identifiers to be matched adequately for further analysis and comparison. It is likely that these datasets do overlap to some extent, particularly with a number of the hospitalizations reported among the cases. This overlapping may explain some of the similar findings between these datasets; however, compared with the case-patient data, the hospitalization and death datasets represent patients with more severe disease. The accuracy of death certificates is limited by the experience of the people completing them. For the hospitalization dataset, we included all primary and secondary hospital diagnoses for coccidioidomycosis, which may have overestimated the true burden of disease. In contrast, coccidioidomycosis may be underreported on death certificates, and underreporting would have underestimated the number of deaths caused by coccidioidomycosis. Lastly, data on type of coccidioidomycosis and concurrent conditions were not available for reported case patients.
CONCLUSION
In California, coccidioidomycosis-associated death rates peaked in 2006, increased in 2011, and decreased in 2012 and 2013. Similar to incidences and hospitalizations, coccidioidomycosis-associated deaths disproportionately affected males, African American and Hispanic people, older people, and those living in endemic areas. Population groups at higher risk for coccidioidomycosis and associated hospitalizations were also at higher risk for coccidioidomycosis-associated deaths. Raising awareness among these populations and their providers is important for proper diagnosis and care.
Footnotes
This study was supported by the Epidemiology and Laboratory Capacity for Infectious Diseases cooperative agreement #3U50CK000410 from the Centers for Disease Control and Prevention. Farzaneh Tabnak and Alyssa Nguyen from the California Department of Public Health's Infectious Diseases Branch prepared and provided the coccidioidomycosis surveillance data. This study was conducted as public health practice and did not require institutional review board approval.
REFERENCES
- 1.Chiller TM, Galgiani JN, Stevens DA. Coccidioidomycosis. Infect Dis Clin North Am. 2003;17:41–57. doi: 10.1016/s0891-5520(02)00040-5. [DOI] [PubMed] [Google Scholar]
- 2.Pappagianis D. Marked increase in cases of coccidioidomycosis in California: 1991, 1992, and 1993. Clin Infect Dis. 1994;19(Suppl 1):S14–8. doi: 10.1093/clinids/19.supplement_1.14. [DOI] [PubMed] [Google Scholar]
- 3.Rosenstein NE, Emery KW, Werner SB, Kao A, Johnson R, Rogers D, et al. Risk factors for severe pulmonary and disseminated coccidioidomycosis: Kern County, California, 1995–1996. Clin Infect Dis. 2001;32:708–15. doi: 10.1086/319203. [DOI] [PubMed] [Google Scholar]
- 4.Smith CE, Beard RR, Whiting EG, Rosenberger HG. Varieties of coccidioidal infection in relation to the epidemiology and control of the diseases. Am J Public Health Nations Health. 1946;36:1394–402. doi: 10.2105/ajph.36.12.1394. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Vugia DJ, Wheeler C, Cummings KC, Karon A. Increase in coccidioidomycosis—California, 2000–2007. MMWR Morb Mortal Wkly Rep. 2009;58(05):105–9. [PubMed] [Google Scholar]
- 6.California Department of Public Health. Yearly summaries of general communicable diseases in California, 2001–2010: coccidioidomycosis cases and rates [cited 2016 Jan 26] Available from: http://www.cdph.ca.gov/data/statistics/Documents/YearlySummaryReportsofSelectedGeneralCommDiseasesinCA2001-2010.pdf#page527.
- 7.California Department of Public Health. Yearly summaries of general communicable diseases in California, 2011–2014: coccidioidomycosis cases and rates [cited 2016 Jan 26] Available from: http://www.cdph.ca.gov/data/statistics/Documents/YearlySummaryReportsofSelectedGeneralCommDiseasesinCA2011-2014.pdf#page529.
- 8.Sondermeyer G, Lee L, Gilliss D, Tabnak F, Vugia D. Coccidioidomycosis-associated hospitalizations, California, USA, 2000–2011. Emerg Infect Dis. 2013;19:1590–7. doi: 10.3201/eid1910.130427. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Huang JY, Bristow B, Shafir S, Sorvillo F. Coccidioidomycosis-associated deaths, United States, 1990–2008. Emerg Infect Dis. 2012;18:1723–8. doi: 10.3201/eid1811.120752. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.State of California, California Department of Public Health. Sacramento (CA): California Department of Public Health; 2013. Multiple cause of death files, 2000–2013. [Google Scholar]
- 11.State of California, Office of Statewide Health Planning and Development. Sacramento (CA): State of California, Office of Statewide Health Planning and Development; 2015. Inpatient hospital discharge data set. [Google Scholar]
- 12.California Department of Finance. Sacramento (CA): California Department of Finance; 2012. Population for California and its counties by age, gender, and race/Hispanics, 2000–2010. Also available from: http://www.dof.ca.gov/research/demographic/data/race-ethnic/2000-2010/intercensal_2000-2010_dbinput_csv.zip [cited 2014 May 30] [Google Scholar]
- 13.Sacramento: California Department of Finance; 2012. Projected California population by age, gender and race-ethnicity, July 1, 2011 [cited 2014 May 30] Available from: http://www.dof.ca.gov/research/demographic/reports/projections/p-3/p-3_caproj_database.zip. [Google Scholar]
- 14.SAS Institute, Inc. SAS®: Version 9.4. Cary (NC): SAS Institute, Inc.; 2013. [Google Scholar]
- 15.Kolivras KN, Johnson PS, Comrie AC, Yool SR. Environmental variability and coccidioidomycosis (valley fever) Aerobiologia. 2001;17:31–42. [Google Scholar]
- 16.Blair JE, Mayer AP, Currier J, Files JA, Wu Q. Coccidioidomycosis in elderly persons. Clin Infect Dis. 2008;47:1513–8. doi: 10.1086/593192. [DOI] [PubMed] [Google Scholar]
- 17.Castle SC, Uyemura K, Rafi A, Akande O, Makinodan T. Comorbidity is a better predictor of impaired immunity than chronological age in older adults. J Am Geriatr Soc. 2005;53:1565–9. doi: 10.1111/j.1532-5415.2005.53512.x. [DOI] [PubMed] [Google Scholar]
- 18.Ampel NM. What's behind the increasing rates of coccidioidomycosis in Arizona and California? Curr Infect Dis Rep. 2010;12:211–6. doi: 10.1007/s11908-010-0094-3. [DOI] [PubMed] [Google Scholar]
- 19.Louie L, Ng S, Hajjeh R, Johnson R, Vugia D, Werner SB, et al. Influence of host genetics on the severity of coccidioidomycosis. Emerg Infect Dis. 1999;5:672–80. doi: 10.3201/eid0505.990508. [DOI] [PMC free article] [PubMed] [Google Scholar]