

U.S. Liaison Committee for Medical Education-accredited medical schools offer many joint advanced-degree programs, including doctor of medicine (MD)-master of public health (MPH) programs.1 During the past 20 years, the number of MD-MPH programs has increased substantially. In 1992–1993, MD-MPH programs were offered at 31 of 126 (24.6%) medical schools.2 By 2004–2005, the number of programs had risen to 64 of 125 medical schools (51.2%),3 and by 2012–2013, the most recent year for which data are available, to 81 of 136 (59.6%) medical schools (Personal communication, Sylvia Etzel, American Medical Association, March 2014, April 2014, and May 2014). National tracking data from the Association of American Medical Colleges (AAMC) indicate that the annual number of MD-MPH program graduates doubled from 2002–2003 to 2012–2013, from approximately 100 graduates to more than 200 graduates.4
Only a few studies have described MD-MPH-program graduates' career plans. Recent studies included a descriptive study of a single-institution's MD-MPH program participants with comparative demographic data for MD program participants;5 a study of medical students from several institutions who completed the MPH program either as MD-MPH program participants or independently with MD and MPH degrees awarded by different institutions;6 and another single--institutional, retrospective cohort study of medical-school graduates that compared characteristics and careers of MD-MPH program graduates and MD graduates who subsequently completed the MPH program with MD-only or MD-other degree graduates, but without MPH degrees.7 To date, no national studies have been reported.
To address this gap in the literature, we conducted a retrospective, national cohort study of Medical College Admission Test (MCAT) examinees who enrolled in medical school to (1) determine the extent of MD-MPH program participation and graduation from U.S. medical schools and (2) compare demographic characteristics, attitudes, academic achievement, and career plans of MD-MPH program and MD program graduates.
METHODS
Our study sample included graduates from MD and MD-MPH programs identified in the AAMC Student Records System. The cohort included graduates who had entered medical school in 2003–2007 and who had graduated by the end of 2012. During 2012–2013, 81 of 136 (60%) medical schools offered MD-MPH programs (Personal communication, Sylvia Etzel, American Medical Association, March 2014, April 2014, and May 2014). We obtained data on these graduates from the AAMC, including data from the Pre-MCAT Questionnaire (PMQ), the Graduation Questionnaire (GQ), the AAMC Student Records System, and the National Board of Medical Examiners.
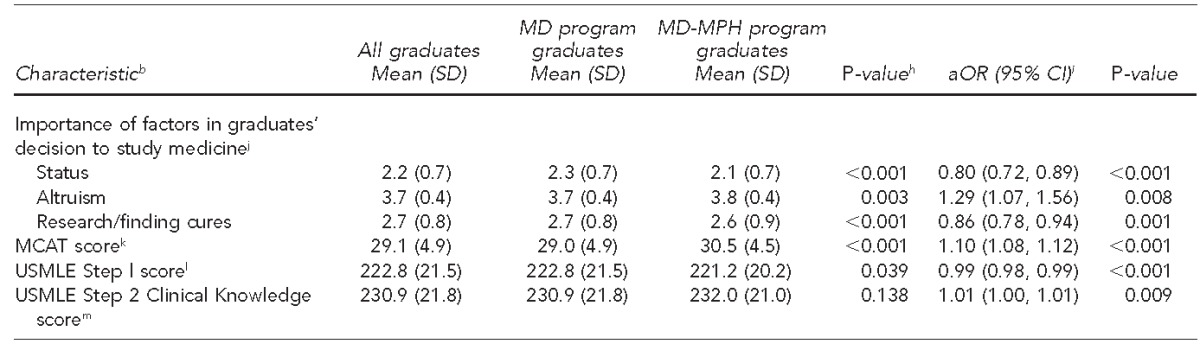
The PMQ was offered to all MCAT examinees in 2001–2006 before their initial MCAT attempt. The PMQ included many items about the areas of medicine that examinees found most interesting and the importance of various items in their decision to study medicine.8 Responses to the item “Indicate the area of medicine in which you are most interested” included public health aspects of disease, biomedical research, or patient management. Response options on the importance of 15 different items in a student's decision to study medicine ranged from 1 (not important) to 4 (extremely important). As previously described,9 we derived three of these factors—altruism, status, and research/finding cures—from 10 of the 15 items for use in our study. We derived the altruism factor from the mean of responses to three items: “profession offers the opportunity to serve community needs,” “coworkers share desire to help people,” and “profession offers opportunity to make a difference in people's lives.” We derived the status factor from the mean of responses to five items: “profession offers opportunity to satisfy personal desire for authority,” “profession represents achievement higher than any other profession,” “physicians receive immediate status and prestige,” “profession offers the possibility of a high income,” and “physicians are rarely unemployed.” We derived the research/finding cures factor from the mean of responses to two items: “profession provides chance to pursue interest in research” and “profession offers opportunity to discover a great cure.”
The GQ is offered to all medical students during the spring of their final year and is completed voluntarily.10 We analyzed responses to items about graduates' career intentions (full-time university faculty; other, including response options of state/federal or medical/health-care administration, part-time faculty, part-time practice, and other; undecided; and missing [i.e., no response to the GQ item] or full-time, non-academic clinical practice); total debt at graduation; age at graduation; and plan for specialty-board certification. Based on responses to the specialty-board certification and specialty-choice items, we created a nine-category specialty-choice variable (internal medicine, family medicine, obstetrics-gynecology, pediatrics, surgical specialties, emergency medicine, no/undecided about specialty-board certification plans, missing [no response to the GQ item(s)], and all other specialties).
The AAMC provided data on sex, race/ethnicity, matriculation and graduation dates, degree program at matriculation, and graduation. We used self-reported PMQ or AAMC Student Records System data, as available, for sex and race/ethnicity (categorized as underrepresented racial/ethnic groups in medicine [i.e., black, Hispanic, and Native American/Alaska Native], Asian/Pacific Islander, other/multiple races/unknown, and non-Hispanic white). The AAMC also provided first-attempt scores on four standardized tests: MCAT (sum of verbal reasoning, biological sciences, and physical sciences sub-scores), National Board of Medical Examiners' U.S. Medical Licensing Examination (USMLE) three-digit Step 1 and Step 2 Clinical Knowledge (CK) scores, and pass-fail USMLE Step 2 Clinical Skills (CS) results. USMLE sequence completion is required for U.S. medical licensure.11
Our outcome of interest was which degree program, MD or MD-MPH, the student was in at the time of graduation. We compared MD-MPH program graduates with MD program graduates (including MD, bachelor of arts-MD, and bachelor of science-MD). We excluded all other MD-advanced-degree program graduates (e.g., MD-master of science, MD-master of arts, MD-juris doctorate, MD-master of business administration, and MD-doctor of philosophy) from analysis.
We report descriptive statistics for each variable examined in association with degree program at graduation (i.e., MD, MD-MPH). We used Pearson's χ2 tests and analysis of variance to measure between-group differences. We used multivariate logistic regression to identify independent predictors of MD-MPH program vs. MD program graduation, reporting adjusted odds ratios (aORs) and 95% confidence intervals (CIs) and controlling for all predictor variables shown in the tables. In addition to the overall model, we stratified the logistic regression analysis by sex and by race/ethnicity. We performed all statistical tests using SPSS® version 22.0,12 and considered two-sided p,0.05 to be significant.
Study sample derivation
Of 262,813 PMQ respondents in 2001–2006, a total of 100,440 (38.2%) respondents entered medical school. Of these respondents, 77,718 (77.4%) matriculated during 2003–2004 through 2007–2008, comprising 91.1% of all 85,312 matriculants in U.S. LCME-accredited medical schools during the cohort years of interest.13 Of these 77,718 matriculants, 72,674 (93.5%) had graduated by the end of 2012, including 69,787 (96.0%) in MD programs, 972 (1.3%) in MD-MPH programs, 904 (1.2%) in MD programs combined with other advanced degrees, and 1,011 (1.4%) in MD-PhD programs. Of the 70,759 MD program and MD-MPH program graduates eligible for study inclusion (100% of whom had completed the PMQ, at least in part), we excluded 10,717 (15.1%) graduates without complete data for all PMQ items of interest and 245 (0.3%) graduates who were missing standardized test data. Our final sample of 59,797 graduates included 58,975 MD program graduates (84.5% of 69,787 MD program graduates) and 822 MD-MPH program graduates (84.6% of 972 MD-MPH program graduates) who met the inclusion criteria and had complete data for all PMQ items and standardized tests of interest (Figure).
Figure.
Flow diagram of Pre-Medical College Admission Test Questionnaire (PMQ) respondents during 2001–2006 in an analysis of MD program graduates and MD-MPH program graduates in the United States through 2012
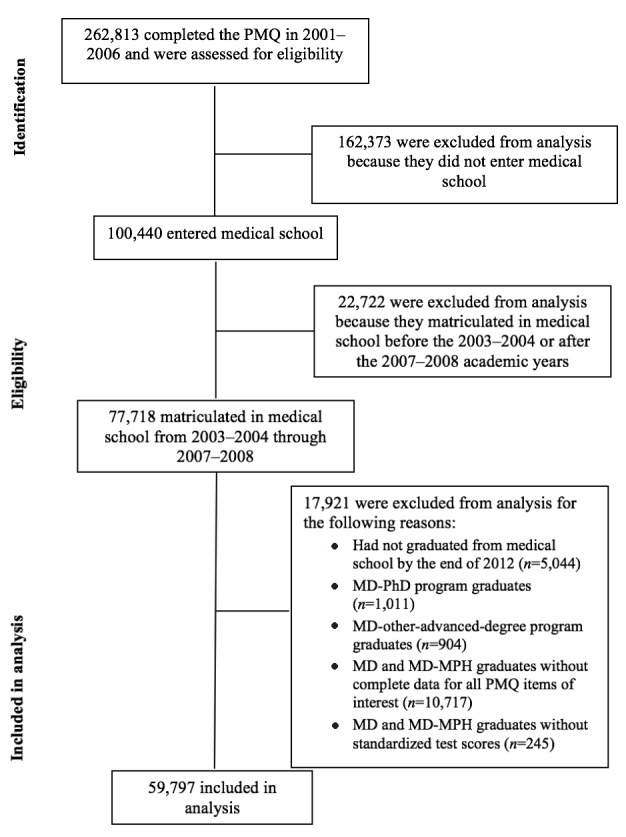
MD = doctor of medicine
MPH = master of public health
PhD = doctor of philosophy
RESULTS
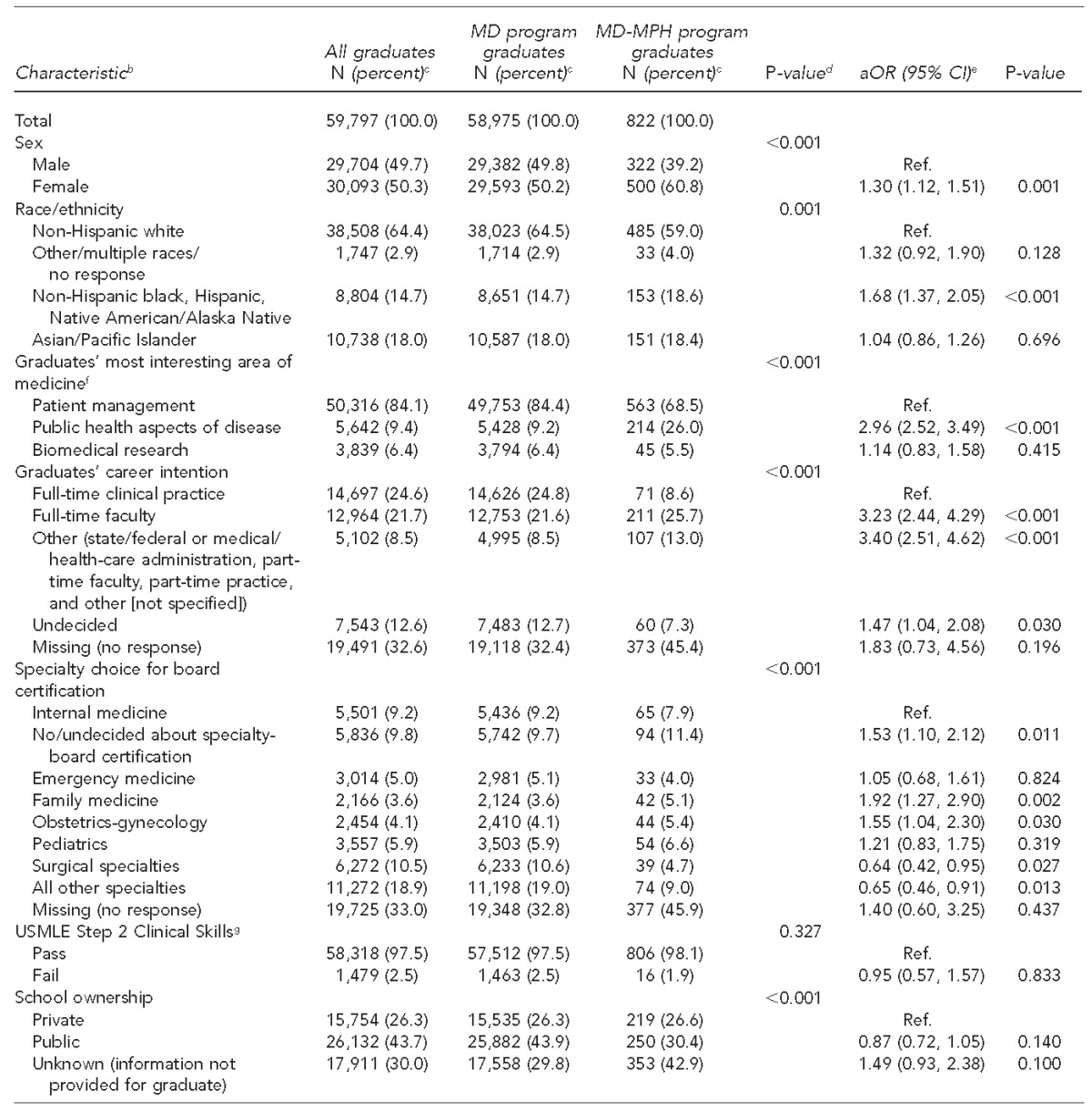
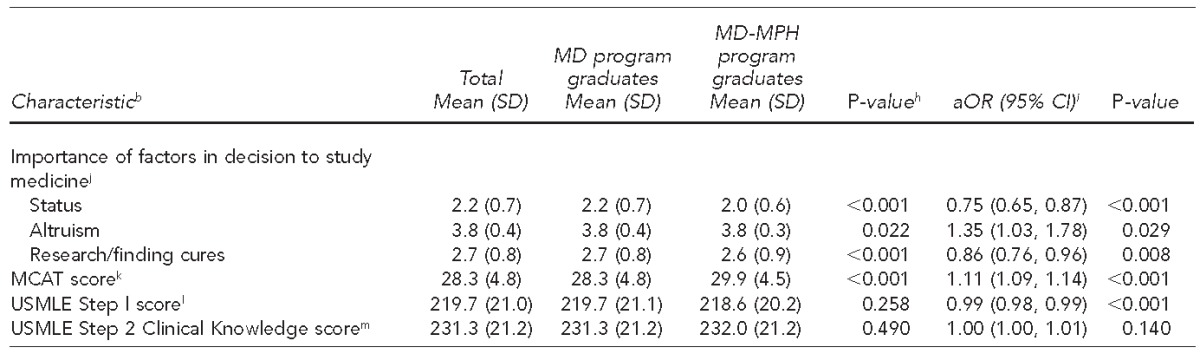
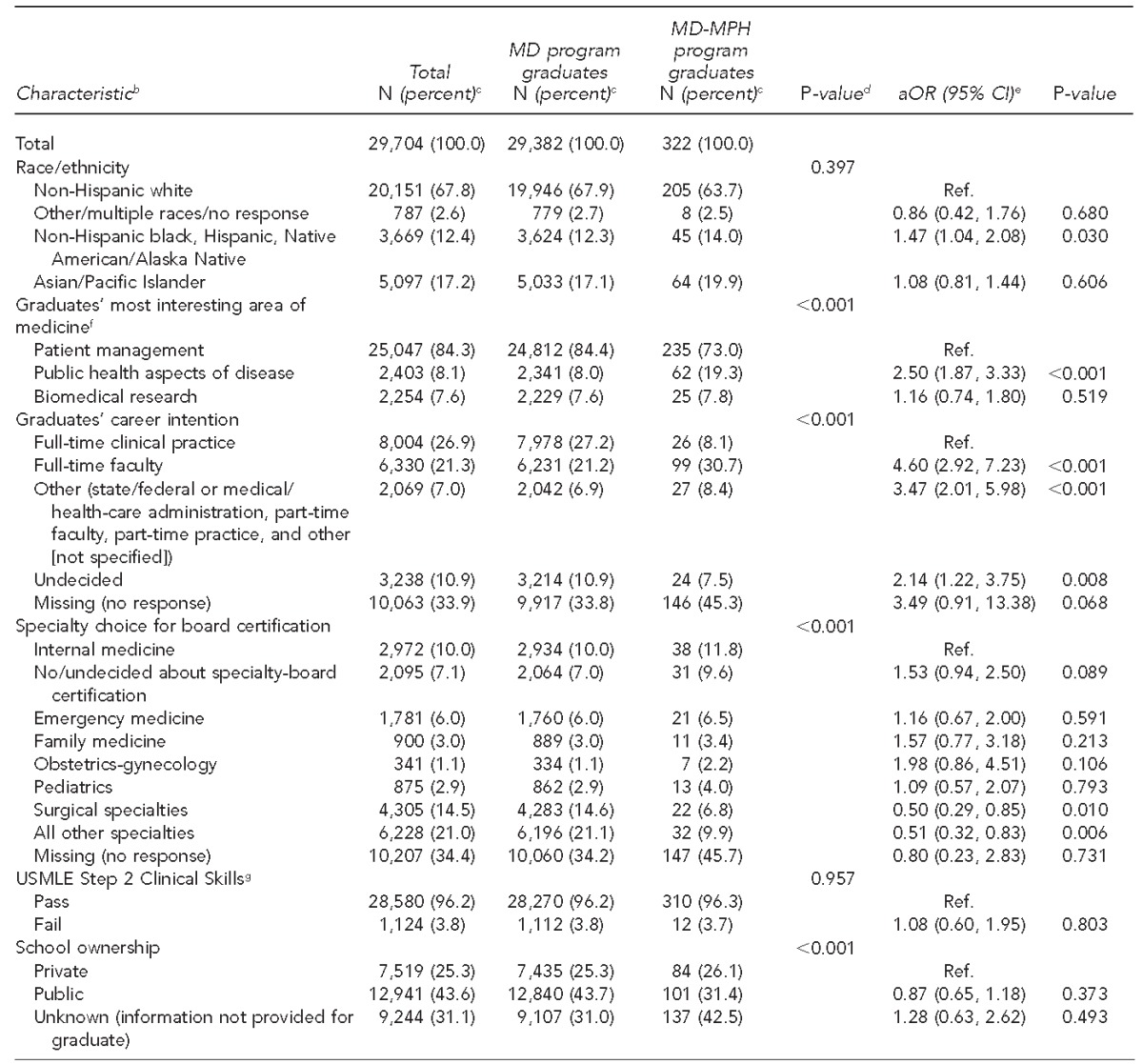
Of the 59,797 medical-school graduates included (Figure), 822 (1.4%) were MD-MPH program graduates and 58,975 (98.6%) were MD program graduates. We found significant between-group differences in all variables except Step 2 CK scores and Step 2 CS results (Table 1). Not shown, of 294 MD-MPH program enrollees at matriculation, 262 (89.1%) completed the MD-MPH program and comprised 31.9% of all 822 MD-MPH program graduates in the sample. The mean (standard deviation [SD]) duration of medical school enrollment was longer for MD-MPH program graduates than for MD program graduates (MD-MPH: 4.9 [0.5] vs. MD: 4.2 [0.4] years; p,0.001); and, based on data available for 41,875 graduates, MD-MPH program graduates were older than MD program graduates (MD-MPH: 28.0 [2.3] vs. MD: 27.3 [2.7] years of age; p,0.001). Also, based on GQ data available for 33,840 graduates, mean (SD) total debt at graduation did not differ significantly between MD-MPH program and MD program graduates overall (MD-MPH: $145,161 [$90,787] vs. MD: $142,224 [$86,890]; p=0.516) or only graduates of private schools (MD-MPH: $153,562 [$101,444] vs. MD: $158,827 [$96,805]; p=0.480) or public schools (MD-MPH: $138,049 [$80,249] vs. MD: $132,406 [$78,827]; p=0.311).
Table 1.
Characteristics of medical-school graduates in the sample, by degree program at graduation, and results of the multivariate logistic regression model predicting MD-MPH program graduation vs. MD program graduation in the United States through 2012a
The study sample comprised U.S. Liaison Committee for Medical Education-accredited medical school MD-MPH and MD program graduates who had completed the Association for American Medical Colleges Pre-MCAT Questionnaire during 2001–2006, entered medical school during 2003–2007, and graduated by the end of 2012.
bData sources included the Association of American Medical Colleges Student Records System, Pre-MCAT Questionnaire, and Graduation Questionnaire; and the National Board of Medical Examiners.
cPercentages may not total to 100 because of rounding.
dTests of significance were Pearson's χ2 tests comparing each categorical variable with degree program at graduation (MD-MPH program graduates vs. MD program graduates).
eHosmer and Lemeshow goodness-of-fit test p50.209.
fResponse options to the item “Indicate the area of medicine in which you are most interested” included public health aspects of disease, biomedical research, or patient management.
gUSMLE Step 2 Clinical Skills is a standardized patient examination testing information-gathering, physical examination, and communication skills; scores are reported on a pass/fail basis.
hTests of significance were one-way analysis of variance testing differences in scores by degree program at graduation (MD-MPH program vs. MD program).
iFor each unit increase, aOR, 1.00 indicates a lower likelihood and aOR .1.00 indicates a greater likelihood of MD-MPH program graduation vs. MD program graduation.
jResponse options about the importance of each item in graduates' decision to study medicine ranged from 1 (not important) to 4 (extremely important).
kMCAT is a multiple-choice examination on verbal reasoning, biological sciences, and physical sciences, with scores ranging from 0 to 45.
lUSMLE Step l is a multiple-choice examination on basic medical sciences, with scores ranging from 1 to 300.
mUSMLE Step 2 Clinical Knowledge is a multiple-choice examination on clinical medical sciences, with scores ranging from 1 to 300.
MD - doctor of medicine
MPH = master of public health
aOR = adjusted odds ratio
CI = confidence interval
Ref. = reference group
USMLE = U.S. Medical Licensing Examination
SD = standard deviation
MCAT = Medical College Admission Test
Graduates who were female or from underrepresented racial/ethnic groups in medicine (i.e., black, Hispanic, and Native American/Alaska Native) reported public health aspects of disease as the most interesting area of medicine on the PMQ; attributed greater importance to altruism as a reason to study medicine on the PMQ; had higher MCAT and Step 2 CK scores; listed GQ specialty category as “family medicine,” “obstetrics-gynecology,” or “no/undecided about specialty-board certification plans;” and reported “full-time faculty,” “other,” or “undecided” GQ career intentions were more likely to be MD-MPH program graduates than to be MD program graduates. Graduates who attributed greater importance to the status of medicine and to research/finding cures on the PMQ as reasons to study medicine, had higher Step l scores, and whose GQ specialty category was “surgical specialties” or “all other specialties” were less likely to be MD-MPH program graduates than to be MD program graduates (Table 1). Seventy percent of graduates in the sample had completed the GQ, at least in part; for each GQ item analyzed, findings for graduates who were missing data for the item did not differ significantly from findings for the reference group.
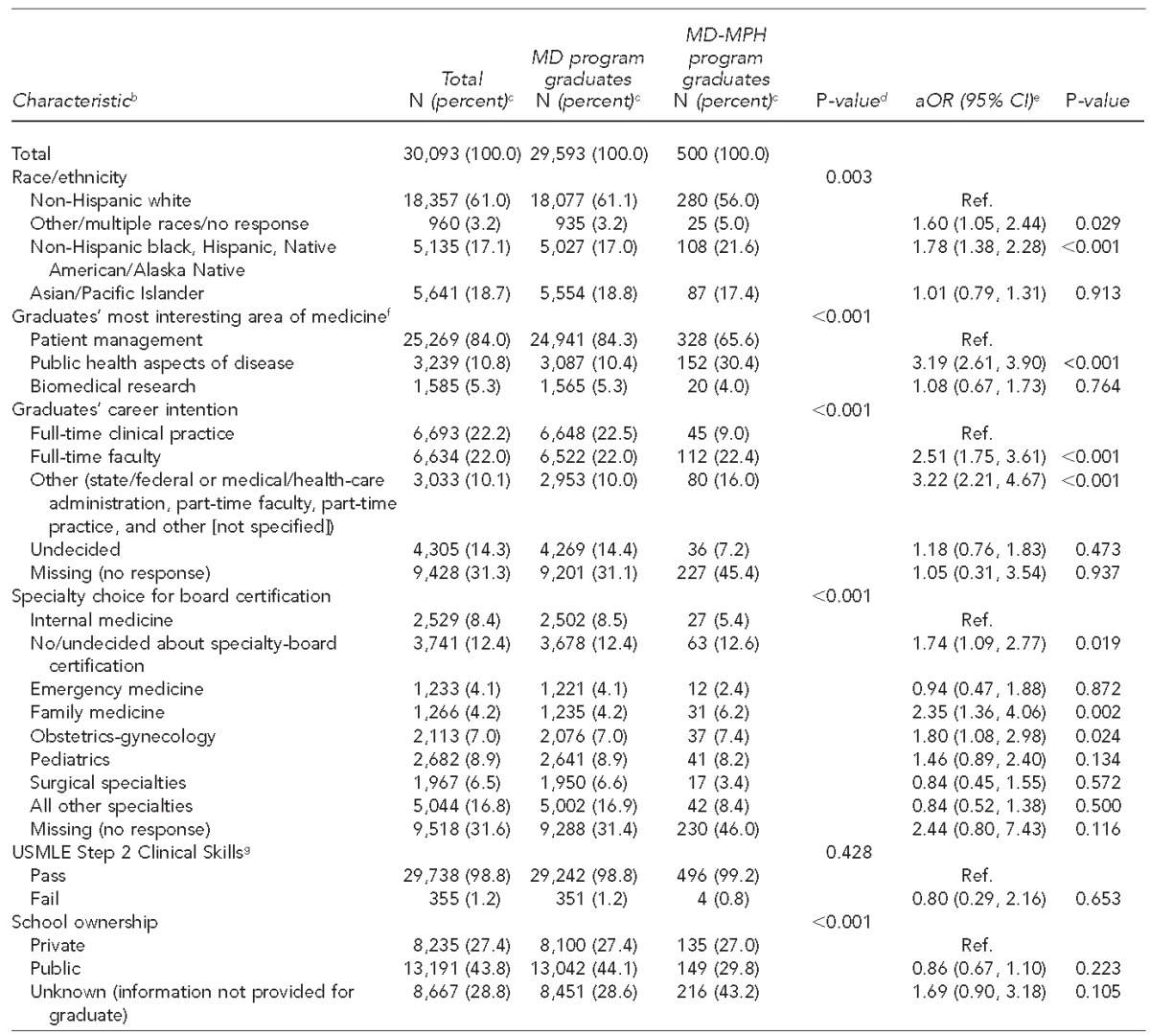
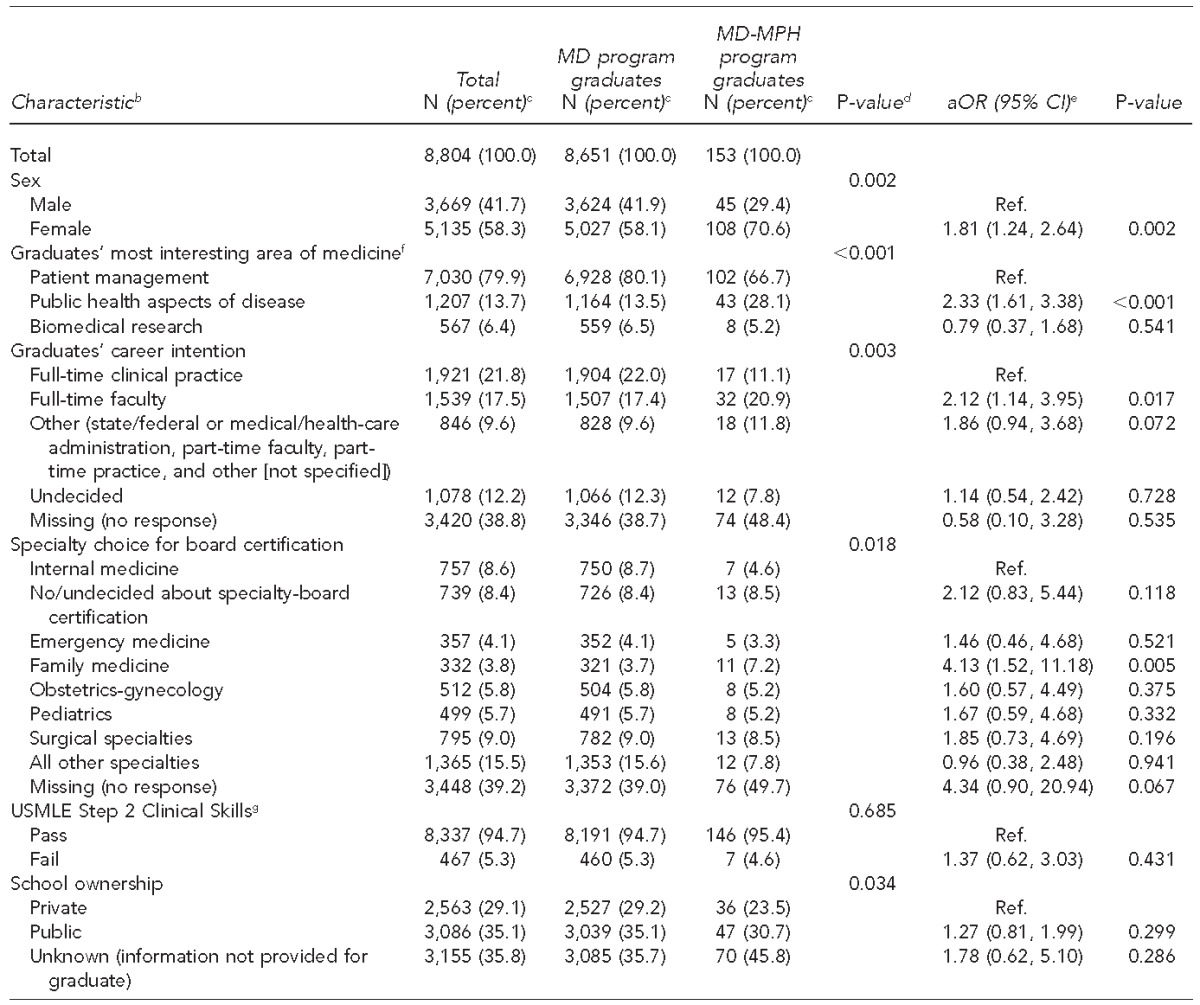
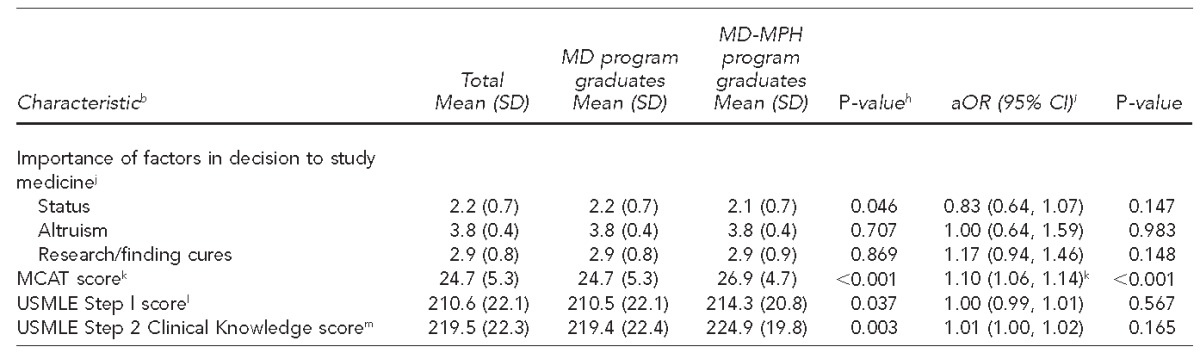
We grouped descriptive statistics by degree program at graduation and ran multivariate logistic regression models separately for women (Table 2) and men (Table 3) to determine if variables independently associated with MD-MPH program (vs. MD program) -graduation differed by sex. Findings for most variables in these two models were generally similar to findings among all graduates (Table 1), although associations between the importance of each of three factors in the decision to study medicine (i.e., status, altruism, and research/finding cures) and MD-MPH program graduation were attenuated and no longer significant among men (Table 3).
Table 2.
Characteristics of all female medical-school graduates in the sample, by degree program at graduation, and results of the multivariate logistic regression model predicting MD-MPH program graduation vs. MD-program graduation in the United States through 2012a
The study sample comprised U.S. Liaison Committee for Medical Education-accredited medical school MD-MPH and MD program graduates who had completed the Association for American Medical Colleges Pre-MCAT Questionnaire during 2001–2006, entered medical school during 2003–2007, and graduated by the end of 2012.
bData sources included the Association of American Medical Colleges Student Records System, Pre-MCAT Questionnaire, and Graduation Questionnaire; and the National Board of Medical Examiners.
cPercentages may not total to 100 because of rounding.
dTests of significance were Pearson's χ2 tests comparing each categorical variable with degree program at graduation (MD-MPH program graduates vs. MD program graduates).
eHosmer and Lemeshow goodness-of-fit test p50.638.
fResponse options to the item “Indicate the area of medicine in which you are most interested” included public health aspects of disease, biomedical research, or patient management.
gUSMLE Step 2 Clinical Skills is a standardized patient examination testing information-gathering, physical examination, and communication skills; scores are reported on a pass/fail basis.
hTests of significance were one-way analysis of variance testing differences in scores by degree program at graduation (MD-MPH program vs. MD program).
iFor each unit increase, aOR, 1.00 indicates a lower likelihood and aOR .1.00 indicates a greater likelihood of MD-MPH program graduation vs. MD program graduation.
jResponse options about the importance of each item in graduates' decision to study medicine ranged from 1 (not important) to 4 (extremely important).
kMCAT is a multiple-choice examination on verbal reasoning, biological sciences, and physical sciences, with scores ranging from 0 to 45.
lUSMLE Step l is a multiple-choice examination on basic medical sciences, with scores ranging from 1 to 300.
mUSMLE Step 2 Clinical Knowledge is a multiple-choice examination on clinical medical sciences, with scores ranging from 1 to 300.
MD = doctor of medicine
MPH = master of public health
aOR = adjusted odds ratio
CI = confidence interval
Ref. = reference group
USMLE = U.S. Medical Licensing Examination
SD = standard deviation
MCAT = Medical College Admission Test
Table 3.
Characteristics of all male medical-school graduates in the sample, by degree program at graduation, and results of the multivariate logistic regression model predicting MD-MPH program graduation vs. MD program graduation in the United States through 2012a

The study sample comprised U.S. Liaison Committee for Medical Education-accredited medical school MD-MPH and MD program graduates who had completed the Association for American Medical Colleges Pre-MCAT Questionnaire during 2001–2006, entered medical school during 2003–2007, and graduated by the end of 2012.
bData sources included the Association of American Medical Colleges Student Records System, Pre-MCAT Questionnaire, and Graduation Questionnaire; and the National Board of Medical Examiners.
cPercentages may not total to 100 because of rounding.
dTests of significance were Pearson's χ2 tests comparing each categorical variable with degree program at graduation (MD-MPH program graduates vs. MD program graduates).
eHosmer and Lemeshow goodness-of-fit test p50.706.
fResponse options to the item “Indicate the area of medicine in which you are most interested” included public health aspects of disease, biomedical research, or patient management.
gUSMLE Step 2 Clinical Skills is a standardized patient examination testing information-gathering, physical examination, and communication skills; scores are reported on a pass/fail basis.
hTests of significance were one-way analysis of variance testing differences in scores by degree program at graduation (MD-MPH program vs. MD program).
iFor each unit increase, aOR, 1.00 indicates a lower likelihood and aOR .1.00 indicates a greater likelihood of MD-MPH program graduation vs. MD program graduation.
jResponse options about the importance of each item in graduates' decision to study medicine ranged from 1 (not important) to 4 (extremely important).
kMCAT is a multiple-choice examination on verbal reasoning, biological sciences, and physical sciences, with scores ranging from 0 to 45.
lUSMLE Step l is a multiple-choice examination on basic medical sciences, with scores ranging from 1 to 300.
mUSMLE Step 2 Clinical Knowledge is a multiple-choice examination on clinical medical sciences, with scores ranging from 1 to 300.
MD = doctor of medicine
MPH = master of public health
aOR = adjusted odds ratio
CI = confidence interval
Ref. = reference group
UMSLE = U.S. Medical Licensing Examination
SD = standard deviation
MCAT = Medical College Admission Test
We also grouped descriptive statistics by degree program at graduation and ran multivariate logistic regression models separately for graduates in the underrepresented racial/ethnic groups in medicine (Table 4) and for graduates in all other racial/ethnic groups combined. Findings for most variables in these models were generally similar in magnitude and direction to findings among all graduates (Table 1). However, graduates in the underrepresented racial/ethnic groups in medicine who chose family medicine (vs. internal medicine) were four times more likely to be MD-MPH program graduates than to be MD program graduates (Table 4). Additionally, associations between the importance of each of the three factors in the decision to study medicine and MD-MPH program graduation were attenuated and no longer significant among graduates in the underrepresented racial/-ethnic groups in medicine (Table 4). In addition, graduates in all other racial/ethnic groups combined who graduated from public (vs. private) medical schools were 19% less likely (aOR50.81, 95% CI 0.66, 0.99) to be MD-MPH program graduates than to be MD program graduates.
Table 4.
Characteristics of medical-school graduates in underrepresented racial/ethnic groups in medicine (non-Hispanic black, Hispanic, Native American/Alaska Native) in the sample, by degree program at graduation, and results of a multivariate logistic regression model predicting MD-MPH program graduation vs. MD program graduation in the United States through 2012a
The study sample comprised U.S. Liaison Committee for Medical Education-accredited medical school MD-MPH and MD program graduates who had completed the Association for American Medical Colleges Pre-MCAT Questionnaire during 2001–2006, entered medical school during 2003–2007 and graduated by the end of 2012.
bData sources included the Association of American Medical Colleges Student Records System, Pre-MCAT Questionnaire, and Graduation Questionnaire; and the National Board of Medical Examiners.
cPercentages may not total to 100 because of rounding.
dTests of significance were Pearson χ2 tests comparing each categorical variable with degree program at graduation (MD-MPH program graduates vs. MD program graduates).
eHosmer and Lemeshow goodness-of-fit test p50.242.
fResponse options to the item “Indicate the area of medicine in which you are most interested” included public health aspects of disease, biomedical research, or patient management.
gUSMLE Step 2 Clinical Skills is a standardized patient examination testing information-gathering, physical examination, and communication skills; scores are reported on a pass/fail basis.
hTests of significance were one-way analysis of variance testing differences in scores by degree program at graduation (MD-MPH program vs. MD program).
iFor each unit increase, aOR, 1.00 indicates a lower likelihood and aOR .1.00 indicates a greater likelihood of MD-MPH program graduation vs. MD program graduation.
jResponse options about the importance of each item in graduates' decision to study medicine ranged from 1 (not important) to 4 (extremely important).
kMCAT is a multiple-choice examination on verbal reasoning, biological sciences, and physical sciences, with scores ranging from 0 to 45.
lUSMLE Step l is a multiple-choice examination on basic medical sciences, with scores ranging from 1 to 300.
mUSMLE Step 2 Clinical Knowledge is a multiple-choice examination on clinical medical sciences, with scores ranging from 1 to 300.
MD = doctor of medicine
MPH = master of public health
aOR = adjusted odds ratio
CI = confidence interval
Ref. = reference group
USMLE = U.S. Medical Licensing Examination
SD = standard deviation
MCAT = Medical College Admission Test
DISCUSSION
To our knowledge, this is the first national study of MD-MPH program graduates with comparative data for MD program graduates. MD-MPH program graduates comprised only about 1.4% of all medical-school graduates in our study sample, and they differed in numerous ways from MD program graduates. Our observation that women and those in underrepresented racial/ethnic groups in medicine were overrepresented among MD-MPH graduates is consistent with the results of a single-institution study of 173 MD-MPH program participants from 1997–2006,5 which showed that women and African American students were relatively overrepresented among medical students who entered the MD-MPH program compared with their representation among all medical students at their institution. To our knowledge, national PMQ and GQ data have not previously been examined in association with MD-MPH program graduation; thus, our findings regarding associations between the PMQ and GQ items we examined and MD-MPH program graduation contribute new knowledge to the literature.
Notably, medical-school graduates who identified public health aspects of disease as the most interesting area of medicine on the PMQ had nearly three times greater odds of being MD-MPH program graduates than being MD program graduates. This new observation supports efforts to promote early awareness about MD-MPH programs among students in the high school and early college years, when students are considering a broad range of career paths. We also observed that students who had placed greater importance on altruism in their decision to study medicine were more likely (aOR51.29) to be MD-MPH program graduates than MD program graduates, suggesting that fostering students' interest in public health aspects of medicine during high school and college may stimulate their interest in MD-MPH programs.
Our findings on standardized testing indicated that both MD program and MD-MPH program graduates performed well academically during medical school. We were not surprised that MD-MPH program graduates in our sample took almost an additional year to complete medical school than MD program graduates. This finding is consistent with information from AAMC indicating that, of 85 MD-MPH programs in place as of August 2014, 70 (82%) were five-year programs; 13 (15%) required <5 years to complete, most with four-year program options; and two (3%) were five- to six-year programs. The fact that many MD-MPH program graduates in our study had enrolled in MD-MPH programs after medical-school matriculation is consistent with the multiple program entry points reported by most MD-MPH programs (i.e., at the time of medical-school application, after medical-school acceptance but before matriculation, or at any time during medical school).14
Our finding that mean debt at graduation did not differ significantly between graduates of MD programs and MD-MPH programs despite a longer time to graduate seems counterintuitive. But any additional out-of-pocket costs incurred by MD-MPH program -graduates may be relatively small. According to the AAMC directory of MD-MPH educational opportunities, some MD-MPH programs offered discounted MPH tuition fees for medical students, reduced credit requirements, and/or scholarship and assistantship opportunities.14
Among all graduates in our study, those who chose family medicine (vs. internal medicine) had nearly twice the odds—and among graduates in the underrepresented racial/ethnic groups in medicine, more than four times the odds—of being MD-MPH program graduates. Conversely, the odds of being an MD-MPH program graduate among students who chose surgical specialties (aOR50.64) or all other specialties (aOR50.65) were significantly lower. A retrospective study of 1,108 physician graduates of a single medical school, including 17.1% with MPH degrees awarded either jointly with or subsequent to the MD degree, reported that medical-school graduates with an MPH were nearly twice as likely as their MD-degree counterparts to have completed a generalist primary-care residency only.7 Our findings suggest that MD-MPH programs might play a role in promoting interest among U.S. medical-school enrollees in specialties such as family medicine, which is aligned with the national need for more primary-care physicians.15–17
In our study, graduates indicating a full-time faculty career intention—a GQ variable with established predictive validity for full-time faculty appointment18—had much greater adjusted odds of being MD-MPH program graduates. This finding is aligned with another single-institution report indicating that its medical-school graduates with an MPH were more likely than its MD graduates without an MPH to obtain employment in an academic institution.7 In our study, graduates who reported “other” career intentions (including response options of state/federal or medical/health-care administration, part-time faculty, part-time practice, and other) had greater odds (aOR53.40) of being MD-MPH program graduates than MD program graduates. Students considering “other” career paths and their advisors/counselors should be aware that the AAMC Careers in Medicine program offers information about alternative career paths—including government work, public policy, informatics, consulting, communication, and journalism—and guidance about career-path selection that best fits medical-school graduates' interests, values, and career goals.19 This program also provides information for students considering public health and service careers in international medicine, preventive medicine, organized medicine (nonprofits and associations), and aerospace medicine.20
Limitations
Our study had several limitations. Our observations about MD-MPH program graduates may not be generalizable to graduates of non-U.S. Liaison Committee for Medical Education-accredited medical schools, to physicians who obtained MPH degrees either before or after medical school (e.g., during residency training21), or to graduates of other types of combined health-professions dual-degree programs (e.g., doctor of dental medicine-MPH).22 Because the predictive validity for full-time, non-academic clinical practice and other GQ career intentions has not been established, further research in this area is warranted to determine if medical-school graduates who indicated these career intentions on the GQ had indeed pursued these career paths. Finally, the small differences that we observed between MD-MPH program and MD program graduates in the importance of altruism, status, and research/finding cures in the decision to study medicine may have been statistically significant due, at least in part, to the large sample size.
CONCLUSION
The number of MD-MPH program graduates in the United States is increasing, but the effects of this growth on public health and on the size of the physician workforce with expertise in public health remain to be seen. Before 2007, approximately 15% of the 6,500 yearly graduates from accredited schools of public health also had an MD degree.23 Because fewer than 200 people graduated from MD-MPH programs annually before 2007,4 most physicians who obtained MPH degrees historically had not completed MD-MPH programs. The increasing availability of MD-MPH programs at U.S. medical schools may result in an overall increase in the number of MDs who also obtain MPH degrees; alternatively, it might only produce a shift toward earlier completion of the MPH during, rather than after, medical school, but with no overall change in the number of physicians who ultimately obtain MPH degrees. Nevertheless, our findings regarding MD-MPH program graduates can further inform an understanding of the potential role of MD-MPH programs in the recruitment and training of a diverse physician workforce that is well positioned to address national public-health workforce needs.
Footnotes
The authors thank Paul Jolly, PhD (retired), and Emory Morrison, PhD, at the Association of American Medical Colleges (AAMC), Washington, D.C., for supporting research efforts through provision of data and assistance with coding; the National Board of Medical Examiners (NBME), Philadelphia, Pennsylvania, for permission to use U.S. Medical Licensing Examination Step data; and James Struthers, BA, and Yan Yan, MD, PhD, at Washington University School of Medicine, for data management services and statistical consultations, respectively.
Dorothy Andriole, Donna Jeffe, and Robert Tai were supported in part by a grant from the National Institute of General Medical Sciences (NIGMS; R01 GM094535). Drs. Andriole and Jeffe also were supported in part by 2R01 GM085350. The NIGMS was not involved in the design or conduct of the study; collection, management, analysis, and interpretation of the data; or preparation, review, or approval of the article. The opinions expressed in this article are those of the authors and do not reflect the views of the AAMC, the NIGMS, the NBME, or their respective staff members. This study was approved by the Institutional Review Board at Washington University School of Medicine as non-human-subjects research.
REFERENCES
- 1.Barzansky B, Etzel SI. Medical schools in the United States, 2010–2011. JAMA. 2011;306:1007–14. doi: 10.1001/jama.2011.1220. [DOI] [PubMed] [Google Scholar]
- 2.Jonas HS, Etzel SI, Barzansky B. Educational programs in US medical schools. JAMA. 1993;270:1061–8. [PubMed] [Google Scholar]
- 3.Barzansky B, Etzel SI. Educational programs in US medical schools, 2004–2005. JAMA. 2005;294:1068–74. doi: 10.1001/jama.294.9.1068. [DOI] [PubMed] [Google Scholar]
- 4.Caulfield M, Redden G, Sondheimer H. Graduation rates and attrition factors for U.S. medical school students. Association of American Medical Colleges. Analysis in Brief. 2014;14:1–2. Also available from: https://www.aamc.org/download/379220/data/may2014aib-graduationratesandattritionfactorsforusmedschools.pdf [cited 2016 Feb 26] [Google Scholar]
- 5.Harris R, Kinsinger LS, Tolleson-Rinehart S, Viera AJ, Dent G. The MD-MPH program at the University of North Carolina at Chapel Hill. Acad Med. 2008;83:371–7. doi: 10.1097/ACM.0b013e318166a848. [DOI] [PubMed] [Google Scholar]
- 6.Stellman JM, Cohen S, Rosenfield A. Evaluation of a one-year masters of public health program for medical students between their third and fourth years. Acad Med. 2008;83:365–70. doi: 10.1097/01.ACM.0b013e318166af00. [DOI] [PubMed] [Google Scholar]
- 7.Krousel-Wood M, He J, Booth M, Chen CS, Rice J, Kahn MJ, et al. Formal public health education and career outcomes of medical school graduates. PLoS One. 2012;7:e39020. doi: 10.1371/journal.pone.0039020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Association of American Medical Colleges. Post-MCAT questionnaire [cited 2016 Feb 26] Available from: https://www.aamc.org/data/pmq.
- 9.Jeffe DB, Andriole DA, Wathington HD, Tai RH. The emerging physician-scientist workforce: demographic, experiential, and attitudinal predictors of MD-PhD program enrollment. Acad Med. 2014;89:1398–407. doi: 10.1097/ACM.0000000000000400. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Association of American Medical Colleges. Graduation questionnaire (GQ) [cited 2016 Feb 26] Available from: https://www.aamc.org/data/gq.
- 11.United States Medical Licensing Examination. What is USMLE? [cited 2016 Feb 26] Available from: http://www.usmle.org.
- 12.IBM Corp. IBM SPSS® Statistics: Version 22.0 for Windows. Armonk (NY): IBM Corp.; 2013. [Google Scholar]
- 13.Castillo-Page L, editor. Diversity in medical education: facts and figures 2008. Washington: Association of American Medical Colleges; 2008. [Google Scholar]
- 14.Association of American Medical Colleges. Directory of MD-MPH educational opportunities [cited 2014 Jul 24] Available from: https://www.aamc.org/students/mdmph.
- 15.Bodenheimer T, Pham HH. Primary care: current problems and proposed solutions. Health Aff (Millwood) 2010;29:799–805. doi: 10.1377/hlthaff.2010.0026. [DOI] [PubMed] [Google Scholar]
- 16.Petterson SM, Liaw WR, Phillips RL, Jr, Rabin DL, Meyers DS, Bazemore AW. Projecting US primary care physician workforce needs: 2010–2025. Ann Fam Med. 2012;10:503–9. doi: 10.1370/afm.1431. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Department of Health and Human Services (US), Health Resources and Services Administration, National Center for Health Workforce Analysis. Rockville (MD): HHS; 2013. Projecting the supply and demand for primary care practitioners through 2020. Also available from: http://bhpr.hrsa.gov/healthworkforce/supplydemand/usworkforce/primarycare/projectingprimarycare.pdf [cited 2016 Feb 26] [Google Scholar]
- 18.Andriole DA, Jeffe DB, Hageman HL, Ephgrave K, Lypson ML, Mavis B, et al. Variables associated with full-time faculty appointment among contemporary U.S. medical school graduates: implications for academic medicine workforce diversity. Acad Med. 2010;85:1250–7. doi: 10.1097/ACM.0b013e3181e10159. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Association of American Medical Colleges. Careers in medicine: alternative careers [cited 2016 Feb 26] Available from: https://www.aamc.org/cim/career/alternativecareers.
- 20.Association of American Medical Colleges. Careers in medicine: public health and service [cited 2016 Feb 26] Available from: https://www.aamc.org/cim/career/alternativecareers/publichealthandservice.
- 21.Baker S, Daginawala N. Leadership training for radiologists: a survey of opportunities and participants in MBA and MPH programs by medical students, residents, and current chairpersons. J Am Coll Radiol. 2011;8:563–7. doi: 10.1016/j.jacr.2011.02.013. [DOI] [PubMed] [Google Scholar]
- 22.Arizona School of Dentistry & Oral Health. D.M.D./M.P.H. dual degree program [cited 2016 Feb 26] Available from: http://www.atsu.edu/asdoh/programs/dual_degree/index.htm.
- 23.Hernandez LM, Munthali AW, editors. Training physicians for public health careers. Washington: National Academies Press; 2007. [Google Scholar]