

Abstract
Mitochondria play an important role in energy production for the cell. The proper function of a myocardial cell largely depends on the functional capacity of the mitochondria. Therefore it is necessary to establish a novel and reliable method for a non-invasive assessment of mitochondrial function and metabolism in humans. Although originally designed for evaluating myocardial perfusion, 99mTc-MIBI can be also used to evaluate cardiac mitochondrial function. In a clinical study on ischemic heart disease, reverse redistribution of 99mTc-MIBI was evident after direct percutaneous transluminal coronary angioplasty. The presence of increased washout of 99mTc-MIBI was associated with the infarct-related artery and preserved left ventricular function. In non-ischemic cardiomyopathy, an increased washout rate of 99mTc-MIBI, which correlated inversely with left ventricular ejection fraction, was observed in patients with congestive heart failure. Increased 99mTc-MIBI washout was also observed in mitochondrial myopathy, encephalopathy, lactic acidosis and stroke-like episodes (MELAS) and in doxorubicin-induced cardiomyopathy. Noninvasive assessment of cardiac mitochondrial function could be greatly beneficial in monitoring possible cardiotoxic drug use and in the evaluation of cardiac damage in clinical medicine.
Keywords: mitochondria, 99mTc-MIBI, ischemic heart disease, heart failure, cardiomyopathy
Introduction
Mitochondria play an important role in energy metabolism and are integrally involved in embryonic development, cell signaling activities, cell-cycle control and cell death (1-2). Hence the proper function of a myocardial cell largely depends on the functional capability of the mitochondria. In vitro techniques using isolated mitochondria or cell culture are frequently used to assess the mitochondrial function. However, the techniques have not been fully established for the evaluation of mitochondrial function and metabolism in vivo. It is necessary to establish a novel and reliable method for non-invasive assessment in humans. This article aims to review promising methods for in vivo assessment of mitochondrial function using nuclear cardiology techniques.
99mTc-MIBI kinetics in the myocardium
The technetium-99m-labeled agents are used to assess myocardial blood flow. HEXAKIS (2-methoxyisobutylisonitrile) technetium-99m (99mTc-MIBI) is a class of alkylisonitrile technetium compounds designed for noninvasive myocardial perfusion imaging. 99mTc-MIBI concentrates in mitochondria according to membrane potential (3). By using quantitative electron-probe x-ray microanalysis, a strong mitochondrial concentration of 99mTc-MIBI was documented (3). The uptake of 99mTc-MIBI is known to be non-dose dependent. Although originally designed for evaluating myocardial perfusion, 99mTc-MIBI can also be used to evaluate cardiac mitochondrial function. Figure 1 illustrates the kinetics of 99mTc-MIBI in the cell. It does not bind to the cell membrane because no activity was counted with the cell debris resulting from the action of trichloroacetic acid. Piwinica-Worms, Kronauge and Chiu et al provided the fundamental explanation of the mechanism responsible for the cellular accumulation of 99mTc-MIBI (4). Various isonophores and inhibitors that affect the electrical potentials of the plasma and mitochondrial membranes could modify 99mTc-MIBI. The dependence of membrane potential is one of the most important factors in 99mTc-MIBI uptake mechanism. Because the cell membranes are more negatively charged at the mitochondrial level than at the sarcolemmal level, the tracer concentrates preferentially in the mitochondria. The presence of membrane electrical potential drives the accumulation of 99mTc-MIBI. A decrease in mitochondrial function in myocardial cell produces a reduction in the mitochondrial inner matrix potential. The uptake of 99mTc-MIBI seems to be completely driven by a process of passive diffusion. The tracer concentrates preferentially in the mitochondria. At equilibrium, 99mTc-MIBI is sequestered within mitochondria by a large negative potential. An increase in 99mTc-MIBI excretion from cell is thought to be due to P-glycoprotein in tumor cell. Besides the use for a myocardial perfusion tracer, 99mTc-MIBI is known to be a potential functional imaging tracer of multidrug-resistant P-glycoprotein in tumor cells. Increased washout rate of 99mTc-MIBI was correlated with poorer therapy response in some tumors (5).
Figure 1.
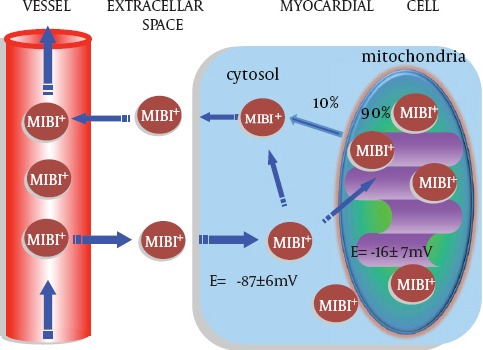
Kinetics of 99mTc-MIBI in the cell. 99mTc-MIBI accumulates and concentrates into cell according to membrane potential
The consequences of simulated ischemia have been assessed by the experimental study (6). Metabolic change that induces an alteration in the myocardial uptake of 99mTc-MIBI could also alter the trans-membrane potentials, which are accompanied by the myocardial ischemia. Previous experimental study demonstrated that approximately 90% of 99mTc-MIBI in vivo is associated with mitochondria in an energy-dependent manner as a free cationic complex (7). Thus 99mTc-MIBI retention in a mitochondrium relates to mitochondrial function. In addition, Carnonyl cyanide-m-chloro phenylhydrazone (CCCP), a mitochondrial uncoupler, rapidly depletes cellular content of 99mTc-MIBI in the presence of tetraphenylborate (4,8). The results support a potential-dependent mechanism for cell uptake of 99mTc-MIBI (6). In the ischemic model, myocardial 99mTc-MIBI uptake was significantly decreased in mild ischemia, and further decreased in severe ischemia (9). Besides, a lack of 99mTc-MIBI uptake has been reported in some experimental studies (10-11).
The washout rate of 99mTc-MIBI becomes greater in heart failure patients than healthy controls. 99mTc-MIBI washout rate could be used for mitochondrial functional imaging, especially in patients with cardiac dysfunction (12). A recent report showed that an increased washout of 99mTc-MIBI was correlated with a decrease in myocardial mitochondrial mRNA expression or an abnormal morphology of mitochondria in patients with dilated cardiomyopathy (DCM) (13). Several mitochondrial protein mRNA are involved in the myocardial adenosine triphosphate (ATP) production in DCM patients. Mitochondrial ATP production is mainly generated by the tricarboxilic acid cycle in the mitochondrial matrix and the electron transport chain in the mitochondrial membrane (13). Electron microscopic findings revealed that the severity of degeneration in the cristae of mitochondria in the myocardium is correlated with myocardial washout of 99mTc-MIBI (13). Therefore an accelerated 99mTc-MIBI clearance from the myocardium is thought to be related to impaired mitochondrial function, including myocardial damage.
Ischemic Heart Disease
In a clinical study on ischemic heart disease, Takeishi et al. made a quantitative analysis of 99mTc-MIBI single photon emission computed tomography (SPECT) in acute myocardial infarction patients with successful percutaneous transluminal coronary angioplasty. Reverse redistribution of 99mTc-MIBI was evident after direct percutaneous transluminal coronary angioplasty (14). The presence of increased washout of 99mTc-MIBI was associated with the infarct-related artery and preserved left ventricular function. Fujiwara found the same phenomenon in patients with acute myocardial infarction (15). Both reverse redistribution of 99mTc-MIBI and 99mTc-MIBI /BMIPP mismatch was related to the recovery of left ventricular function, indicating myocardial viability. Reverse redistribution of 99mTc-MIBI may be helpful in prognostic assessment and clinical-decision making in patients with acute myocardial infarction. However, in patients with coronary spastic angina, faster myocardial clearance of 99mTc-MIBI was also observed in the SPECT study, indicating that the ability of myocytes to retain the tracer was impaired due to repetitive brief ischemia by coronary spasm (16). Therefore, the early and delayed 99mTc-MIBI SPECT imaging provides useful information for the diagnosis and responses to the treatment in patients with coronary spastic angina.
Non-ischemic Cardiomyopathy
Both dilated and hypertrophic cardiomyopathies are often accompanied by changes in oxidative phosphorylation or respiratory enzyme activities in cardiac tissues (2). In non-ischemic cardiomyopathy, clinical usefulness of using 99mTc-MIBI for cardiac mitochondrial function in patients with cardiomyopathy was recently investigated (12). A 740-MBq dose of 99mTc-MIBI was injected slowly through the antecubital vein and flushed with a 10mL saline solution at rest. The planar and SPECT images were obtained approximately 30 minutes and 3.5 hours after the injection. Cardiac 99mTc-MIBI uptake was measured by heart/mediastinum (H/M) average count ratio, and washout rate was calculated (12). Planar imaging of H/M of 99mTc-MIBI is a simple method that allows comparison of inter-individual and institutional results (Figure 2). An increased washout rate of 99mTc-MIBI was observed in patients with congestive heart failure when compared to the washout rates of those without heart failure (12). Matsuo et al. reported that the washout rate of 99mTc-MIBI was positively correlated with the level of brain natriuretic peptide, end-systolic and end-systolic volume of the left ventricle (12). The washout rate of 99mTc-MIBI was inversely correlated with left ventricular ejection fraction, peak filling rate and first-third ejection fraction. Thus the high 99mTc-MIBI washout rate could be associated with earlier progression of congestive heart failure, suggesting that the evaluation of 99mTc-MIBI washout rate may be useful for predicting the outcomes of congestive heart failure. Since heart failure could be caused by impaired energy production in mitochondria of the cardiomyocyte, the washout rate of 99mTc-MIBI could be a good indicator of myocardial damage or dysfunction even in non-ischemic cardiomyopathy. Besides, the decrease in H/M of iodine-123-metaiodobenzyguanidine (MIBG), a tracer to detect cardiac sympathetic nerve function, was associated with higher washout rate of 99mTc-MIBI in patients with heart failure (11). MIBG scintigraphy and circulating B-type or brain natriuretic peptide (BNP) could be used in combination with perfusion tracer of 99mTc-MIBI to provide complementary information on severity of patients with heart failure (12,17).
Figure 2.
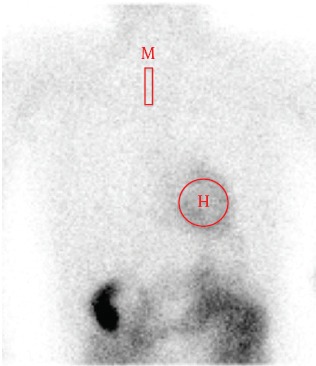
Quantitative analysis by heart-to-mediastinum count ratio on planar image. M = mediastinum; H = heart.
Cardiac Function Evaluation
Quantitative gated single-photon emission computed tomography (QGS) can provide accurate and reproducible values for ejection fraction, regional wall motion, wall thickening and dyssynchrony (18-20). Although a normal heart may contract in a coordinated way, the ischemic burden or myocardial damage results in the inability of cardiomyocyte to produce energy in the mitochondria. Consequently, cardiac dyssynchrony also occurs in such patients. Phase analysis of left ventricular dyssynchrony using a perfusion tracer can be used clinically and gives information on left ventricular dyssynchrony to detect coronary artery disease (21). Furthermore, for evaluating patients with left ventricular bundle branch block or ischemic heart disease, it seems to be more appropriate to evaluate left ventricular wall motion and wall thickening. The assessment of systolic and diastolic function has been commonly used to describe a category of congestive heart failure. These cardiac function evaluations by QGS give useful information on the severity of heart failure.
Lactic acidosis and stroke-like episodes
Mitochondrial disorders are a heterogeneous group of diseases resulting from abnormalities in mitochondrial deoxyribonucleic acid and function. Cardiac involvement manifesting as hypertrophic (symmetrical or asymmetrical) or dilated cardiomyopathy is frequently observed in mitochondrial myopathy, encephalopathy, lactic acidosis and stroke-like episodes (MELAS) (22). For instance, in a patient with MELAS, increased 99mTc-MIBI washout, which correlated inversely with left ventricular ejection fraction, was observed, whereas increased 123I-beta-methyl iodophenyl-pentadecanoic acid (123I-BMIPP) uptake was observed in the region of decreased 99mTc-MIBI uptake.
Doxorubicin-Induced Cardiomyopathy
Doxorubicin (Adriamycin) is one of the original anthracyclines isolated in the early 1960s from the pigment-producing bacterium Streptomyoces percetius, together with daunorubicin. However, doxorubicin has been known to exert many biochemical effects on myocytes, including damage to mitochondria, alteration of nucleic acids and protein synthesis, and lipid peroxidation after free radical generation. Its cardiotoxicity is a dose-dependent process resulting in myocyte damage that may cause congestive heart failure. Monitoring of patients and diagnostic procedures are important because its cardiotoxicity can be lethal. We reported that the 99mTc-MIBI washout rates were higher after the chemotherapy compared to before the chemotherapy in a malignant bone tumor patient with doxorubicin-induced cardiomyopathy (23). Quantitative gated SPECT data showed that the cardiac function decreased in a patient with doxorubicin-induced cardiomyopathy as shown in Figure 3. The washout rate of 99mTc-MIBI increased significantly after the chemotherapy in a patient with doxorubicin-induced cardiomyopathy (Figure 4). 99mTc-MIBI could monitor the change of mitochondrial damage induced by chemotherapy in asymptomatic patients with possible anthracycline antibiotic cardiotoxicity, although there is no difference in SPECT imaging before and after chemotherapy. Moreover, cardiac functions, such as systolic and diastolic function, were impaired more severely in patients with cardiotoxicity than those without (22). Further studies are needed to establish the usefulness of 99mTc-MIBI washout rates in chemotherapy in a larger population of patients (24). Not only doxorubicin but also various kinds of drugs have a potential for cardiotoxicity. The relationship between the increase of myocardial washout of 99mTc-MIBI and poor prognosis in the heart of a patient with cardiotoxicity demonstrate that early detection of these abnormalities and early recognition of myocardial insufficiency is important. Hypertension, ischemia, toxic drugs, or genetic abnormalities cause myocardial damages and may finally result in congestive heart failure. The myocardial washout of 99mTc-MIBI could be a marker for mitochondrial damage in various cardiac diseases.
Figure 3.
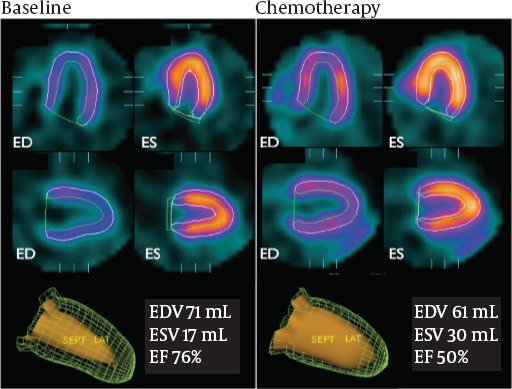
Quantitative gated-SPECT provides cardiac systolic and diastolic functional information. The cardiac function deteriorated in a patient after chemotherapy.
Figure 4.
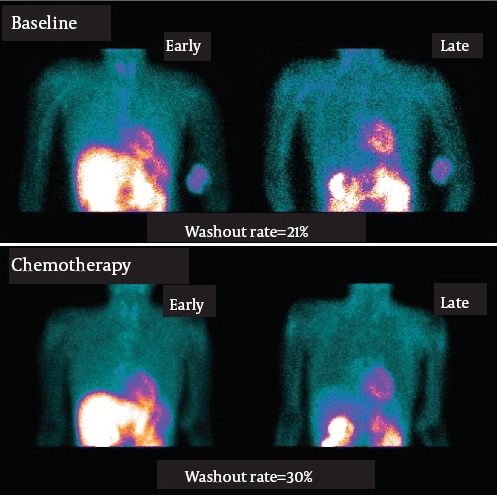
Initial and delayed planar images after administration of 99mTc-MIBI, on baseline and after chemotherapy in a female patient (37 y.o.) with osteosarcoma. The washout rate is increased after chemotherapy (21% on baseline to 30% after chemotherapy).
There may be several factors that affect the values of washout, including age, sex and sympathetic nerve function. The cut-off value between normal and abnormal mitochondrial function is not yet determined. Quantification of the 99mTc-MIBI wash out rate needs to be established by further investigations.
Conclusion
Noninvasive assessment of cardiac mitochondrial function could be of great benefit in monitoring effective drug use and in the evaluation of cardiac damage in clinical medicine. Although there are a limited number of clinical studies, important features of 99mTc-MIBI outlined in this review suggest utility in assessment of cardiac mitochondrial function. Further studies are needed to fully establish nuclear imaging techniques as a noninvasive assessment of mitochondrial function.
References
- 1.Ong SB, Hausenloy DJ. Mitochondrial morphology and cardiovascular disease. Cardiovasc Res. 2010;88(1):16–29. doi: 10.1093/cvr/cvq237. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Finck BN, Kelly DP. Peroxisome proliferator-activated receptor gamma coactivator-1 (PGC-1) regulatory cascade in cardiac physiology and disease. Circulation. 2007;115(19):2540–8. doi: 10.1161/CIRCULATIONAHA.107.670588. [DOI] [PubMed] [Google Scholar]
- 3.Backus M, Piwnica-Worms D, Hockett D, Kronauge J, Lieberman M, Ingram P, LeFurgey A. Microprobe analysis of Tc-MIBI in heart cells: calculation of mitochondrial membrane potential. Am J Physiol. 1993;265(1 Pt 1):C178–87. doi: 10.1152/ajpcell.1993.265.1.C178. [DOI] [PubMed] [Google Scholar]
- 4.Piwnica-Worms D, Kronauge JF, Chiu ML. Enhancement by tetraphenylborate of technetium-99m-MIBI uptake kinetics and accumulation in cultured chick myocardial cells. J Nucl Med. 1991;32(10):1992–9. [PubMed] [Google Scholar]
- 5.Kostakoglu L, Kiratli P, Ruacan S, Hayran M, Emri S, Ergün EL, Bekdik CF. Association of tumor washout rates and accumulation of technetium-99m-MIBI with expression of P-glycoprotein in lung cancer. J Nucl Med. 1998;39(2):228–34. [PubMed] [Google Scholar]
- 6.Maublant JC, Gachon P, Moins N. Hexakis (2-methoxy isobutylisonitrile) technetium-99m and thallium-201 chloride: uptake and release in cultured myocardial cells. J Nucl Med. 1988;29(1):48–54. [PubMed] [Google Scholar]
- 7.Carvalho PA, Chiu ML, Kronauge JF, Kawamura M, Jones AG, Holman BL, Piwnica-Worms D. Subcellular distribution and analysis of technetium-99m-MIBI in isolated perfused rat hearts. J Nucl Med. 1992;33(8):1516–22. [PubMed] [Google Scholar]
- 8.Arbab AS, Koizumi K, Toyama K, Arai T, Araki T. Technetium-99m-tetrofosmin, technetium-99m-MIBI and thallium-201 uptake in rat myocardial cells. J Nucl Med. 1998;39(2):266–71. [PubMed] [Google Scholar]
- 9.Piwnica-Worms D, Chiu ML, Kronauge JF. Divergent kinetics of 201Tl and 99mTc-SESTAMIBI in cultured chick ventricular myocytes during ATP depletion. Circulation. 1992;85(4):1531–41. doi: 10.1161/01.cir.85.4.1531. [DOI] [PubMed] [Google Scholar]
- 10.Li QS, Frank TL, Franceschi D, Wagner HN, Jr, Becher LC. Technetium-99m methoxyisobutyl isonitrile (rp30) for quantification of myocardial ischemia and reperfusion in dogs. J Nucl Med. 1988;29:1539–48. [PubMed] [Google Scholar]
- 11.Liu Z, Okada DR, Johnson G, Hocherman SD, Beju D, Okada RD. 99mTc-sestamibi kinetics predict myocardial viability in a perfused rat heart model. Eur J Nucl Med Mol Imaging. 2008;35:570–8. doi: 10.1007/s00259-007-0549-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Matsuo S, Nakae I, Tsutamoto T, Okamoto Horie M. A novel clinical indicator using Tc-99m sestamibi for evaluating cardiac mitochondrial function in patients with cardiomyopathies. J Nucl Cardiol. 2007;14:215–20. doi: 10.1016/j.nuclcard.2006.10.022. [DOI] [PubMed] [Google Scholar]
- 13.Hayashi D, Ohshima S, Isobe S, Cheng XW, Unno K, Funahashi H, Shinoda N, Okumura T, Hirashiki A, Kato K, Murohara T. Increased 99m Tc-sestamibi washout reflects impaired myocardial contractile and relaxation reserve during dobutamine stress due to mitochondrial dysfunction in dilated cardiomyopathy patients. J Am Coll Cardiol. 2013 doi: 10.1016/j.jacc.2013.01.074. e-pub. [DOI] [PubMed] [Google Scholar]
- 14.Takeishi Y, Sukekawa H, Fujiwara S, Ikeno E, Sasaki Y, Tomoike H. Reverse redistribution of technetium-99m-sestamibi following direct PTCA in acute myocardial infarction. J Nucl Med. 1996;37(8):1289–94. [PubMed] [Google Scholar]
- 15.Fujiwara S, Takeishi Y, Atsumi H, Yamaki M, Takahashi N, Yamaoka M, Tojo T, Tomoike H. Prediction of functional recovery in acute myocardial infarction: comparison between sestamibi reverse redistribution and sestamibi/BMIPP mismatch. J Nucl Cardiol. 1998;5(2):119–27. doi: 10.1016/s1071-3581(98)90194-5. [DOI] [PubMed] [Google Scholar]
- 16.Ono S, Takeishi Y, Yamaguchi H, Abe S, Tachibana H, Sato T, Kubota I. Enhanced regional washout of technetium-99m-sestamibi in patients with coronary spastic angina. Ann Nucl Med. 2003;17(5):393–8. doi: 10.1007/BF03006607. [DOI] [PubMed] [Google Scholar]
- 17.Sugiura T, Takase H, Toriyama T, Goto T, Ueda R, Dohi Y, Sugiura T, Takase H, Toriyama T, Goto T, Ueda R, Dohi Y. Usefulness of Tc-99m methoxyisobutylisonitrile scintigraphy for evaluating congestive heart failure. J Nucl Cardiol. 2006;13(1):64–8. doi: 10.1016/j.nuclcard.2005.10.003. [DOI] [PubMed] [Google Scholar]
- 18.Matsuo S, Matsumoto T, Nakae I, Koh T, Masuda D, Takada M, et al. Prognostic value of ECG-gated thallium-201 single-photon emission tomography in patients with coronary artery disease. Ann Nucl Med. 2004;18(7):617–622. doi: 10.1007/BF02984584. [DOI] [PubMed] [Google Scholar]
- 19.Matsuo S, Nakae I, Matsumoto T, Horie M. Impact of endothelial dysfunction on left ventricular remodeling after successful primary coronary angioplasty for acute myocardial infarction- Analysis by quantitative ECG-gated SPECT. Ann Nucl Med. 2006;20(1):57–62. doi: 10.1007/BF02985592. [DOI] [PubMed] [Google Scholar]
- 20.Matsuo S, Matsumoto T, Nakae I, Ito M, Nakamura Y, Takada M, Murata K, Horie M. Evaluation of cardiac resynchronization therapy in drug-resistant idiopathic dilated cardiomyopathy by means of Tc-99m tetrofosmin ECG-gated SPECT. Exp Clin Cardiol. 2004;9(4):248–250. [PMC free article] [PubMed] [Google Scholar]
- 21.Matsuo S. Phase analysis using gated myocardial perfusion single-photon emission computed tomography imaging for evaluating cardiac dyssynchrony. Circ J. 2012;76(8):1832–3. doi: 10.1253/circj.cj-12-0636. [DOI] [PubMed] [Google Scholar]
- 22.Matsuo S, Nakajima K, Kinuya S, Sato Y, Matsumoto T, Horie M. Cardiac scintigraphic findings of mitochondrial myopathy, encephalopathy, lactic acidosis and stroke-like episodes: a case report. Exp Clin Cardiol. 2008;13(2):93–95. [PMC free article] [PubMed] [Google Scholar]
- 23.Matsuo S, Taki J, Nakajima K. Evaluation of myocardial damage using Tc-99m sestamibi in patients with chemotherapy. J Cardiol Jpn Ed. 2011;6(Suppl-I):442. [Google Scholar]
- 24.Matsuo S, Nakajima K, Kinuya S. Clinical use of nuclear cardiology in the assessment of heart failure. World J Cardiol. 2010;2(10):344–356. doi: 10.4330/wjc.v2.i10.344. [DOI] [PMC free article] [PubMed] [Google Scholar]