

Abstract
Based on the profound biological insights of the last years into the molecular pathogenesis of mantle cell lymphoma and the clinical introduction of new targeted drugs, with high efficacy and a good safety profile, the therapeutic scenario for this tumor has been shown to be thoroughly favourable. No longer characterized by a uniformly dismal prognosis, mantle cell lymphoma has been revealed as a spectrum of different diseases, ranging from very indolent cases to highly aggressive and refractory ones. Thus, there is an urgent need to adapt therapy to accommodate the diverse presentations of the disease. High-dose chemotherapy, followed by autologous stem cell transplantation is the current standard of care for younger patients, generally providing high responses and long survival rates, but hampered by acute and long-term toxicity. In addition, some patients may be overtreated, while others could benefit from targeted approaches, based on the new, molecular-directed compounds. Such a personalized treatment based on the specific characteristics of individual patients may be guided by validated prognostic tools, such as the Mantle Cell Lymphoma International Prognostic Index and the Ki-67 Proliferative Index, as well as by early predictors of treatment response, like minimal residual disease analysis. Moreover, mutation screening of distinctive genomic alterations may provide new, predictive biomarkers, with an additional impact on clinical practice. Only after tailoring treatment according to the clinical and biological heterogeneity of the disease the role of transplantation and modern therapeutic options will be redefined in mantle cell lymphoma.
Introduction
Mantle cell lymphoma (MCL) is a relatively rare lymphoma subtype, constituting nearly 6–8% of all non-Hodgkin Lymphomas (NHL) in Europe and North America. MCL is typically diagnosed in elderly males, with a median age at diagnosis of 65 years and a male preponderance of 3 to 1.1 Since its worldwide recognition in 1994, it has been known to have a dismal prognosis (“the worst lymphoma to have”), with a median overall survival (OS) rate of 3 years only. Unfortunately, no curative therapy has been established so far.2,3
After many years without significant advance in the management of patients with MCL, recently the prognosis for younger patients has improved significantly due to the introduction of dose-intensified regimens containing cytarabine, some incorporating autologous stem cell transplantation (ASCT), and the introduction of anti-CD20 monoclonal antibody rituximab. However, these intensive regimens raise some concern regarding acute and late toxicities and are not suitable for elderly patients, who represent the majority of MCL patients.4 The superiority of sequential regimens with ASCT consolidation after high-dose cytarabine schemes versus some intensive schedules like Hyper-CVAD/MA are debated, especially between European and American clinical groups.5 More importantly, even among younger patients, a minority presents with clinically indolent features (“indolent MCL”) or with classical MCL but characterized by low tumor mass and low-risk according to the MIPI (MCL International Prognostic Index) and/or the Ki-67 Proliferative Index. These patients also represent a dilemma for the clinician as to whether to offer them a high-dose therapy or not, as intensive treatments, with or without ASCT, are hampered by short-and long-term toxicities, including secondary malignancies.6,7
Moreover, recently the scientific and therapeutic scenario for MCL patients has rapidly changed: new biological insights into the molecular pathogenesis of MCL have highlighted some crucial oncogenic signaling pathways, underlying the aggressiveness and chemorefractoriness of the disease. Such discoveries have paved the way for the concept of personalized medicine in MCL. On one hand, the availability of these new diagnostic tests offers a better and more rational biology-based prognostic stratification of patients at baseline, suggesting different treatment strategies for patients with various risk profiles. On the other hand, a deeper unveiling of the underlying mechanisms has led to the clinical development of many new small molecules acting towards specific molecular targets, with high anti-lymphoma activity in some cases.8,9 The current availability of effective, targeted drugs and the increasing clinical application of robust and predictive diagnostic tools have already started to change the therapeutic algorithms of MCL and will challenge the established role of ASCT.
Therefore, our review will draw on the current landscape of evidence supporting ASCT in MCL, subsequently describing the most important new drugs available in clinical practice for this lymphoma and will finally debate the role of ASCT in the near future, proposing a new therapeutic algorithm for MCL in the era of personalized medicine.
The role of high-dose therapy and autologous transplantation
Soon after the recognition of MCL as a distinct entity in the REAL (Revised European-American Lymphoma) Classification back in 1994, it became obvious that this lymphoma subtype has a more aggressive clinical course with rapid relapses and subsequent chemorefractoriness, as compared to indolent lymphoma. Initially, MCL typically showed slightly lower response rates to polychemotherapy and a short event-free survival (EFS) and OS of 8 and 28 months, respectively, in a German series of 45 patients.2,3 The combination of rituximab with fludarabine or CHOP (cyclophosphamide, doxorubicin, vincristine and prednisone), though improving the response rate and the time to treatment failure (TTF), did not impact on OS, resulting in a median progression-free survival (PFS) of only slightly more than one year, with virtually unchanged long-term perspectives.10,11
On the contrary, more promising results were obtained in phase II studies implementing high-dose cytarabine, with or without ASCT. A sequential CHOP-DHAP (dexamethasone, high-dose cytarabine and cisplatin) regimen led to a CR rate of >80% in a series of 28 patients. Responding patients underwent intensified consolidation with total body irradiation (TBI), high-dose Ara-C, melphalan and ASCT, resulting in an impressive 3-year EFS rate of 83% and 3-year OS rate of 90%.12
Similarly, high response rates of more than 90% were demonstrated by the MD Anderson Cancer Center with a dose-intensified approach. Twenty-five patients received an alternating regimen of hyper-CVAD (hyperfractionated cyclophosphamide, vincristine, doxorubicin and dexamethasone) with high-dose cytarabine and methotrexate (MA). However, in this elderly patient population the median TTF was only 15 months, and hematologic toxicity was significant.13
The role of consolidation by dose intensification and ASCT was supported by encouraging results obtained by different phase II studies, aiming at the elimination of residual lymphoma cells after conventional chemotherapy.14–16 In addition, the benefit of TBI as part of the conditioning regimen in MCL was suggested by a retrospective analysis (PFS after 4 years: 71% vs. 0%, P<0.0001; OS 89% vs. 60%, P=0.07).17
Thus, in 1996, the European MCL Network embarked on a randomized comparison of CHOP followed by myeloablative radiochemotherapy (high-dose cyclophosphamide + 12 Gy TBI) followed by ASCT versus IFNα maintenance in patients under 65 years of age in order to assess more precisely the impact of ASCT. Patients in the ASCT arm experienced a significantly longer PFS, even though the 3-year OS was not significantly superior (Table 1).18 However, in a subsequent analysis the median OS was also superior in the ASCT arm after extended median follow-up (63 months) (90 months versus 54 months, P=0.034).19 Therefore, chemotherapy dose intensification and ASCT support became the standard of care for younger MCL patients. However, the non-curative potential of this intensive approach was witnessed by the continuous relapsing pattern and lack of molecular remissions (MR) (determined by Bcl-1 or immunoglobulin rearrangement nested-PCR approach).20,21
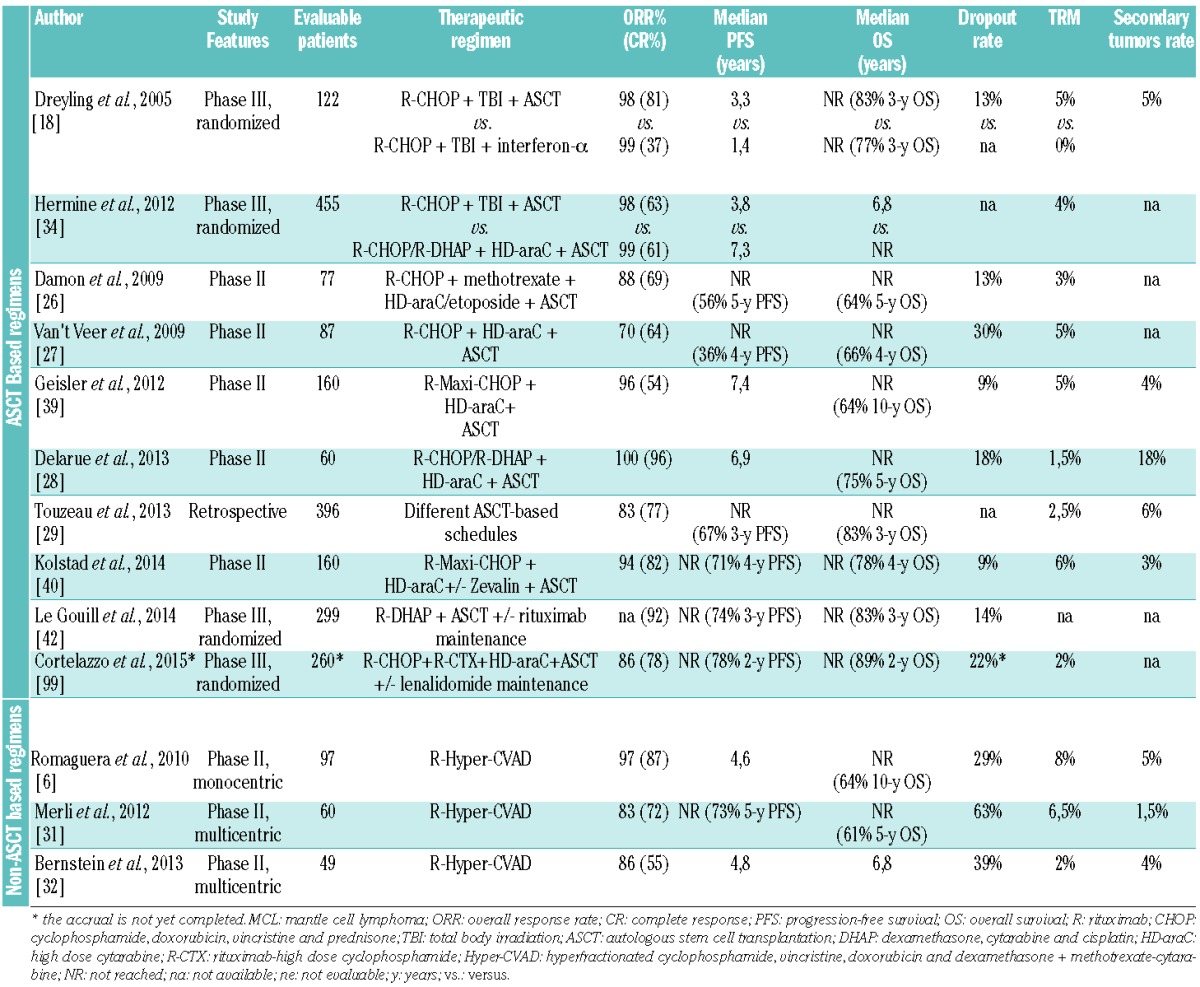
Table 1.
Published clinical studies investigating first-line dose-intensified therapy in MCL.
Nonetheless, the subsequent integration of rituximab and high-dose cytarabine into ASCT programs led to unprecedented levels of cytoreduction, making MR an attainable target in MCL patients. In 2003 Massimo Gianni et al. reported MR in 19 out of 20 patients receiving a rituximab-supplemented high-dose sequence (R-HDS), along with very favorable 4-year EFS and OS rates (79% and 89%, respectively).22 Comparable results were reported for a multicenter phase II trial by the Nordic Lymphoma Group. One hundred and sixty MCL patients received an induction with R-maxi-CHOP alternating with R-high dose cytarabine, followed by a high-dose consolidation (BEAM) with ASCT. MR was achieved in 92% of the 79 evaluable patients, while overall and complete response was achieved in 96% and 54%, respectively. The 6-year EFS, PFS and OS were 56%, 66%, and 70%, respectively, with no relapses observed after 5 years.23 Moreover, achievement of MR, irrespective of high-dose therapy with ASCT or less intensive immunochemotherapy regimens, was an independent predictor of clinical outcome.24,25
Additional phase II studies, as well as a large retrospective population-based analysis showed similar favorable clinical results of high-dose cytarabine-containing schedules followed by ASCT, with overall response rates (ORR) ranging from 70% to 100% (CR: 64–96%), 5-year OS ranging from 64% to 75% and acceptable toxicity profiles (treatment-related mortality ≤ 5%), but a significant dropout rate (13%–30%).26–29
Similarly, the MD Anderson Hyper-CVAD/MA regimen with rituximab resulted in excellent results in a monocentric series of 97 patients. Nonetheless, this dose-intensive regimen was not devoid of TRM and high dropout rates (8% and 29%, respectively)30 and its application in multicentric trials revealed a limited feasibility.31,32 Finally, a recent “real-life”, population-based observational study by the Nordic Lymphoma Group, demonstrated that rituximab (n=766; HR=0.66; P<0.001) and ASCT (n=273; HR=0.55; P<0.004) were independently associated with improved OS among patients receiving systemic treatment.33
Based on these promising data, in 2004 the European MCL Network launched the “MCL Younger” phase III trial, comparing a conventional R-CHOP induction to the “experimental” French one (alternating induction of 3 courses of R-CHOP and R-DHAP), both followed by myeloablative consolidation, TBI and ASCT. Preliminary results confirmed that the R-CHOP/R-DHAP arm achieved a significantly improved median TTF and OS (Table 1), with a comparable number of treatment-related deaths in both groups.34 The impact of cytarabine on the TTF rate was closely linked to MR in the bone marrow, which was much more frequent in the R-CHOP/R-DHAP arm (68% vs. 24%, P<0.001).35
Therefore, ASCT is currently considered the standard first-line consolidation therapy for younger MCL patients (including “low-risk” cases), as stated by international guidelines,36,37 as well as a recent consensus of the European MCL Network and the Lymphoma Working Party of the European Society for Blood and Marrow Transplantation (EBMT).38
However, although the overall results of all these high-dose cytarabine-containing regimens are excellent, with a median OS of more than 10 years in the updated Nordic Lymphoma Group experience, late relapses continue to occur, highlighting that even ASCT-based programs alone are not able to eradicate MCL.39 A recent trial by the Nordic Lymphoma Group failed to demonstrate an improved outcome after90 Yttrium-ibritumomab tiuxetan-BEAM conditioning before ASCT.40 On the other hand, more promising maintenance strategies are being implemented after ASCT, based on the results of rituximab maintenance in elderly MCL patients.41 The ongoing phase III Lyma trial (NCT00921414) investigated the role of rituximab maintenance after four courses of R-DHAP and ASCT. Besides confirming very favorable CR, PFS and OS rates (Table 1), the data from the interim analysis show a promising 2-year EFS of 93% in the rituximab maintenance arm versus 82% in the control arm (hazard ratio, HR = 2.1), suggesting that rituximab maintenance after ASCT may become a new standard of care in MCL.42 Currently, the randomized phase III trial FIL-MCL0208 (EudraCT Number 2009-012807-25) is exploring lenalidomide maintenance in young MCL patients after ASCT, and results are eagerly awaited.99
Despite high response rates and long-term survival advantages after the described high-dose schedules, the non-negligible toxicity profile of such an approach has to be disclosed. Dropout rates generally range between 10%–30% in all the studies (Table 1), with the major adverse events being infectious (neutropenic fever, pneumonia) and gastrointestinal (10%–15% of patients), besides the need for red cell and platelet transfusions (10%–30% of cycles). TRM generally ranges between 2%–8%, mainly due to infectious and cardiac complications. Moreover, costs of hospitalization for high-dose therapy and ASCT have to be considered. Finally, all the reported intensive regimens displayed a significant rate of second tumor development, ranging from 4% up to 18% (Table 1). These results are in line with the long-term secondary neoplasia rates of a large retrospective study on more than 1000 lymphoma patients treated with high-dose therapy, rituximab and ASCT (10-year rates of myelodysplasia/acute leukemia, 4.5% and solid tumors, 6.8%).7
Table 1 describes the most important published clinical studies investigating first-line high-dose therapy in MCL.
The emerging role of new drugs
During the last years, growing insights into the molecular biology of MCL have led to the systematic exploration of targeted approaches.8 Many new compounds are currently being tested within clinical trials, and some of them have already received approval both in the USA and Europe (Table 2), based on impressive activity in relapsed/refractory patients. Current trials are investigating the combinations with immunochemotherapy in earlier treatment lines, with the aim of enhanced efficacy, without adding further toxicity.
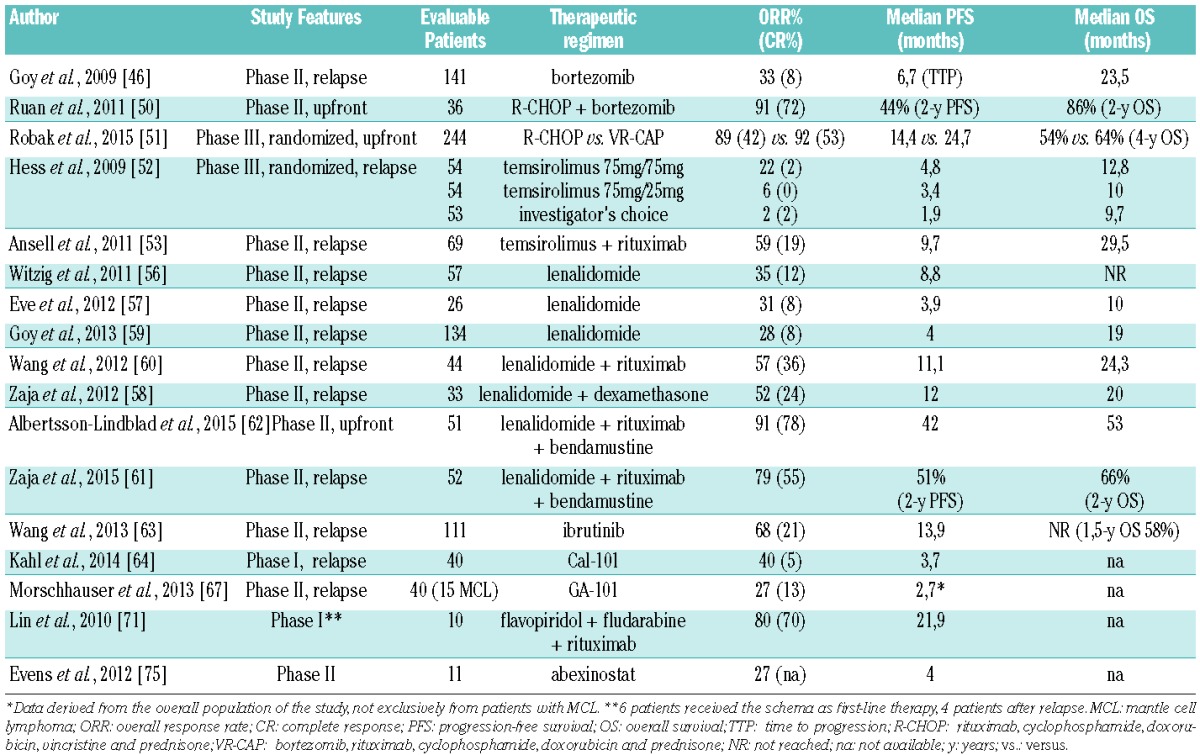
Table 2.
Recent published clinical studies investigating targeted approaches in MCL (with more than 10 evaluable MCL patients).
In the USA the first new agent registered in relapsed MCL was bortezomib, a selective and reversible proteasome 26S inhibitor. Some phase II, single-agent data showed significant responses and favorable PFS and OS rates, with predictable toxic effects.43–46 Since then, many combinations with rituximab and chemotherapy were tested, mainly in a limited series of relapsed/refractory patients.47–50 More recently, the phase III trial LYM-3002 showed that the substitution of vincristine by bortezomib in front-line R-CHOP (“VR-CAP” regimen) improved outcomes in elderly patients with MCL (Table 2); however, an increased hematologic toxicity was observed.51
Temsirolimus, an intravenous mammalian target of rapamycin (mTOR) inhibitor, received the European Medicines Agency (EMA) approval in 2009, due to its single-agent activity. This approval was based on a randomized phase III trial, showing superiority to monochemotherapy (Table 2).52 The addition of rituximab showed even higher response rates in a phase II study.53 To further improve its efficacy, temsirolimus is currently being investigated in combination with BR: of note, all evaluable patients of the phase I part responded to this combination.54
The immunomodulatory compound lenalidomide showed high activity in relapsed/refractory MCL patients in many phase II trials, either as a single-agent or combined with dexamethasone.55–59 Subsequently, a chemo-free lenalidomide-rituximab combination resulted in even higher response rates (Table 2) and impressive response duration of up to 19 months.60 Finally, preliminary results of a phase II trial in first relapse showed activity and the feasibility of a dose reduced rituximab, lenalidomide plus bendamustine combination, followed by lenalidomide maintenance.61 Nevertheless, a full dose combination in a front-line setting showed an excess of toxicity and secondary malignancies.62
Recently, highly promising data were reported for inhibitors of the B-cell receptor pathway. The covalent oral inhibitor of Bruton’s tyrosine kinase (BTK) ibrutinib showed durable single-agent efficacy in relapsed or refractory MCL.63 Based on an international phase II trial in heavily pre-treated MCL patients responses were achieved in the majority of patients paired with excellent tolerability (Table 2). Prior treatment with bortezomib had no effect on the response rate. The most common adverse events were mild or moderate diarrhoea, fatigue, and nausea. Grade 3 or higher hematologic events were infrequent and included neutropenia (16%), thrombocytopenia (11%), and anemia (10%). One phase III trial comparing ibrutinib versus temsirolimus monotherapies in relapsed patients (NCT0164021) has confirmed the superiority of the BTK inhibitor, and another trial assessing a BR schedule plus/minus ibrutinib in first-line therapy (NCT01776840) has completed accrual.
Another antagonist of the BCR signal cascade, idelalisib, a specific inhibitor of phosphatidylinositol 3-kinase delta isoform, also achieved high response rates in MCL, but had a disappointing median duration of response of only 2.7 months.64
Finally, many other promising targeted drugs are also currently being tested in MCL. New anti-CD20 monoclonal antibodies (mAB), such as obinutuzumab and ofatumumab,65–67 bispecific anti-CD19/anti-CD3 mAB blinatumumab,68,69 the toxin-immunoconjugated mAB anti-CD79b DCDS4501A,70 direct inhibitors of cyclin-dependent kinase 4 and 6 (flavopiridol and PD0332991),71–73 oral second generation BCL-2 inhibitors (venetoclax)74 and novel oral pan-histone deacetylase inhibitors (abexinostat).75 Overall, the above mentioned compounds showed activity in MCL. Nevertheless, additional studies on larger MCL patient cohorts are warranted to assess their specific role in this lymphoma subtype.
A summary of the recently published clinical trials of targeted approaches in MCL is presented in Table 2.
Looking for a tailored treatment in MCL
The well known biological and clinical heterogeneity of MCL, as well as the recent availability of highly active, but also expensive new compounds, urges the introduction of the concept of “personalized medicine” into the clinical practice of MCL. However, to effectively tailor the therapeutic approach according to the individual patient’s risk profile reliable prognostic tools applicable in clinical routine are mandatory. The ideal prognosticator should integrate clinical and biological features, taking into account the recent knowledge of molecular pathogenesis.
Currently, the most widely applied tool is the prognostic MIPI score, encompassing simple clinical parameters such as age, performance status, LDH and the leukocyte count.76 Based on easy calculations available via internet, and validation in a “simplified” version76,77 (Table 3), the MIPI is able to stratify newly diagnosed patients into three risk classes with different 5-year OS rates: 83%, 63%, and 34% in MIPI low, intermediate, and high-risk groups, respectively.78 However, there are some important limitations: first of all, as the “age” is one of the most important variables, MIPI fails to correctly classify some younger “high-risk” patients; moreover, it is not able to precisely stratify the outcomes of “low” and “intermediate” risk groups among elderly patients.78 Therefore, the integration of a validated biomarker, such as the Ki-67 proliferative index, has been proposed (“biological-MIPI”, MIPI-b).76 A Ki-67 index ≥ 30% was associated with poor outcome in different patients series, after conventional or intensified chemotherapy plus rituximab.23,79,80 The Ki-67 integration into the MIPI-b was validated in a large series of patients from randomized trials carried out by the European MCL Network, identifying patients at higher relapse risk in both the younger and older age categories, but again not reliably stratifying between “low” and “intermediate” risk groups.78 This limitation has been overcome by a recently improved version of “combined” MIPI, MIPI-c, identifying four risk classes based on a 30% Ki-67 cut-off value (5-year OS rates, 85%, 72%, 43% and 17%, respectively, P<0.0001)81 (Figure 1). However, an important limitation is the reproducibility of the Ki-67 evaluation in pathology labs, where the published guidelines may not be routinely followed.82 Moreover, a representative lymph node biopsy is required: thus, cases diagnosed only on BM histology are often not sufficiently evaluable.
Table 3.
Simplified MIPI calculation.
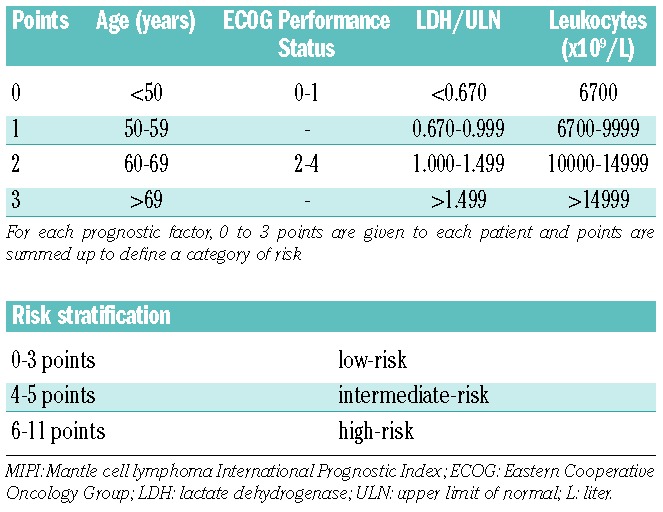
Figure 1.
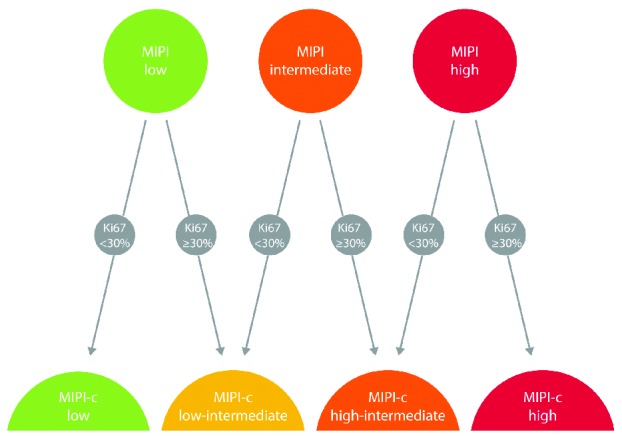
Alternative combination of Ki-67 index and MIPI: MIPIc. MIPI-c: combined mantle cell lymphoma international prognostic index.
More recently, the integration of new biomarkers in the MIPI has been proposed. A study by the Nordic Lymphoma Group reported that microRNA (miR)-18b overexpression identifies MCL patients with poor outcome.83 Despite the intriguing biological rationale of this work, the wide application of this tool appears to be hampered by the missing availability of miR analysis in clinical routine.
The only other validated prognosticator in MCL is the post-treatment evaluation of MRD by allele-specific oligonucleotide (ASO)-PCR. MRD analysis is able to detect very low levels (up to 1.00E-05) of residual lymphoma cells in patients achieving complete clinical response (CR) after treatment. This tool, currently applicable in 90% of MCL patients (with an available diagnostic specimen and BM or peripheral blood follow-up samples) is an effective early predictor of outcome, with an independent prognostic value in a large series of patients, which is even superior to CR achievement in multivariate analysis.25 Its value has been confirmed in various patients series through different treatments (both standard and high-dose chemotherapy, as well as maintenance therapy) in both young and elderly patients.24,25,35,39,84 Moreover, MRD prospective assessment is able to identify early those high-risk patients with molecular relapse only and thus prone to clinical relapse within the subsequent two years.84 This setting allows preemptive trials investigating non toxic treatments at MRD reappearances.85,86 The major limitations of this approach is the technical complexity of the MRD analysis with patient-specific primers, currently reliable only in specialized labs, applying standardized guidelines and performing regular quality control rounds (“EuroMRD group”).87
However, although such predictive tools effectively stratify patients into different risk classes, solid data on their application into personalized treatments are still lacking. To our knowledge, thus far only two trials designed by the Nordic Lymphoma Group have investigated tailored therapy in MCL. The “MCL2” trial proposed a “preemptive” rituximab strategy for 26 patients experiencing MRD recurrence after ASCT:85 even though molecular reconversion rates and preliminary data on survival are promising, the limited patient number does not yet justify therapeutic approaches in clinical routine.39 Moreover, the attempt to improve the prognosis of “high-risk” MCL (according to MIPI and MIPI-b) by offering increased doses of cytarabine did not yield satisfying results (“MCL5”).88 Therefore, although broadly validated, neither MIPI nor Ki-67 nor MRD are currently routinely applied to guide treatment decisions in MCL.36 Thus, a practical application of these predictors in the next clinical trials is eagerly awaited, to finally investigate tailored therapies in MCL.
In addition, in the last years, many new molecular pathways involved in tumor survival, aggressiveness and treatment refractoriness have been identified.8,89 Thus, numerous molecular markers (including SOX11 expression, p53 alterations and Notch-1 mutations)90–94 have been linked with outcome. However, a reliable translation of biological data into the context of clinical patient care is currently lacking, not yet allowing for a personalized strategy in the majority of MCL cases.
MCL: is transplant dead or alive?
Given that a high-dose schedule containing cytarabine and rituximab, followed by an ASCT, is nowadays widely recognized as the standard of care for younger patients affected by MCL, some important considerations should be made that might change the therapeutic scenario in the upcoming years.
First of all, the valuable results in terms of improved survival rates after high-dose therapy and ASCT consolidation are counterweighted by non-negligible toxicities, as previously described.7 Given that some patients do not need immediate treatment (the clinically defined “indolent MCL”, potentially identified by the lack of SOX11 expression),95–97 and others benefit from very long remissions after ASCT, it is reasonable to challenge the value of intensified treatment in these patients in order to avoid unnecessary toxicities. In this context, the recent improvements in induction schemes,34,98 as well as the very promising data on rituximab maintenance,41 even after ASCT,42 strongly suggest a more sustained PFS, especially in younger patients.
Moreover, the high activity of the targeted drugs as a single-agent in relapsed patients has prompted their investigation in combination with immunochemotherapy in first-line trials.51,62 Their impact on long-term survival will potentially result in new options for first-line treatment, and might challenge the current role of ASCT consolidation. This is precisely the concept of the upcoming phase III trial “Triangle” by the European MCL Network (EudraCT Number 2014-001363-12), assessing whether the implementation of a BTK-inhibitor in first-line treatment could eliminate the need for an ASCT consolidation in younger patients. In detail this trial offers a randomization between conventional induction R-CHOP/R-DHAP + ASCT, versus the identical scheme with the addition of ibrutinib, versus R-CHOP/R-DHAP + ibrutinib without ASCT (Figure 2). However, this trial does not implement personalized treatment according to the discussed prognosticators.
Figure 2.
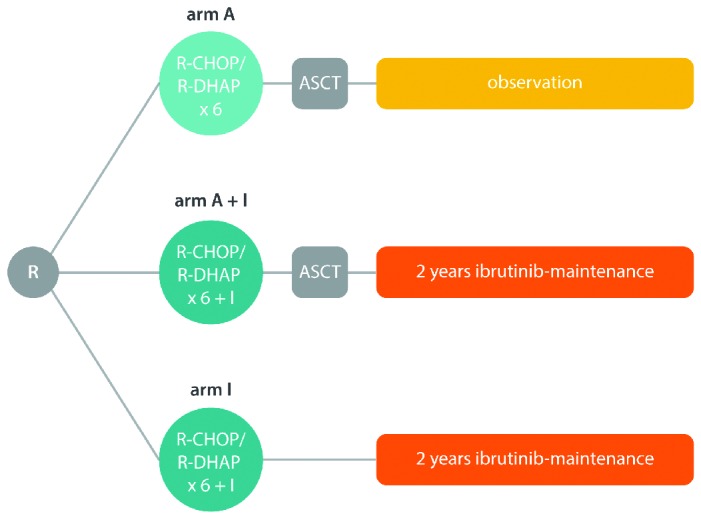
Schematic representation of the “Triangle” trial by the European MCL Network. MCL: mantle cell lymphoma; R: randomization; ASCT: autologous stem cell transplantation; R-CHOP: rituximab, cyclophosphamide, doxorubicin, vincristine and prednison; R-DHAP: rituximab, dexamethasone, cytarabine and cisplatin.
Interestingly, some important data on the value of ASCT are emerging from MRD studies, supporting the concept of “dispensable therapy”. High-dose consolidation followed by ASCT demonstrated a high impact on tumor reduction in the pooled treatment arms (R-CHOP vs. R-CHOP/R-DHAP) of the European MCL Network “Younger” trial, increasing the MR rate from 50% to 75% (P=0.0001). However, this improvement was prominent only in the R-CHOP arm (29% to 65%; P=0.0023), while detectable but not statistically significant after the more effective R-CHOP/R-DHAP arm (76% to 88%; P=0.18). Remarkably, MR after induction was associated with a significantly improved remission duration (89% vs. 74% at 24 months, P=0.002), and sustained MR during the first year after ASCT was also predictive for outcome.35 This observation underlines the important role of cytarabine in inducing sustained MR in MCL. Thus, it may be speculated that patients already achieving MR after high-dose cytarabine plus rituximab induction might do well without ASCT consolidation. Conversely, patients with persistent MRD positivity after a highly effective cytarabine induction might not benefit from ASCT, and thus may be potential candidates for experimental strategies. In accordance, such molecular results have been recently presented for the Italian “MCL0208” trial: preliminary MRD data demonstrate only a marginal improvement of the MR rate (from 67% to 73%) after ASCT.99 Of course, these MRD results have to be confirmed by subsequent PFS results: however, in our opinion, they should prompt the investigation of MRD-guided personalized treatment strategies.
Finally, despite their high efficacy, ASCT based regimens do not lead to complete eradication of the disease. Actually, even among long-term responders, late relapses still continue to occur up to 10 years after the transplantation.39 In addition, MRD reappearance has shown to herald full-blown relapse (with a median time to clinical relapse of 18 months).84 Thus, even after ASCT, effective maintenance therapies have to be considered42 and MRD-driven pre-emptive treatments may be investigated in the context of maintenance trials. Finally, a problem which remains unresolved are the “very high-risk” patients, in whom the standard high-dose + ASCT approach does not result in long-term disease control.88 There is an urgent need to identify those patients at baseline, in order to investigate new front-line approaches, tailored on the high risk of early disease progression. Currently, some genomic alterations have been described, predicting high risk of treatment failure: in particular p53 and CDK2N mutations, as well as complex karyotype mutations.94,100 Those patients who are refractory to intensified therapies and ASCT are appropriate candidates to explore new, targeted approaches or to undergo immunological approaches, such as allogeneic transplantation or the recently described chimeric antigen receptor T cells.101 However, all of these therapeutic approaches have to be further investigated in the context of well-designed clinical trials, carefully weighing the pros and cons. In this regard, concerns are actually rising about the unsustainable costs of the unselected use of targeted drugs, as well as their long-term toxicity; very little is known about their role in inducing subsequent aggressive transformations of the disease.102
On the basis of all these considerations we propose a rational strategy of “personalized first-line treatment” for younger MCL patients, to be investigated in a clinical trial (Figure 3). In our model risk stratification is based on MIPI-c and mutational analysis at baseline, and MRD evaluation during therapy: low-risk and MRD negative low-intermediate risk patients may not proceed to ASCT consolidation, while high-intermediate and high-risk patients should receive a combined chemotherapy induction with biological agents; finally, consolidation and maintenance strategies may be carried out in all patients based on the post-treatment MRD result.
Figure 3.
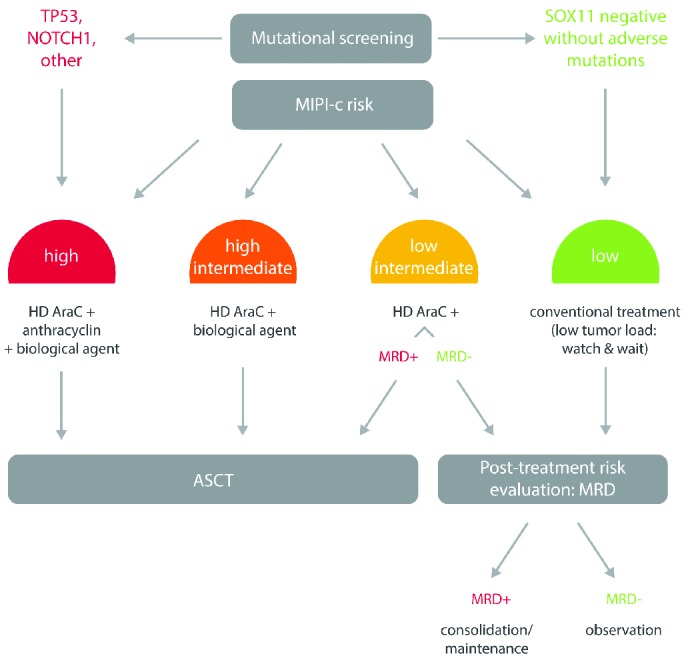
Suggested personalized treatment strategy according to risk stratification in mantle cell lymphoma (MCL). MIPI-c: combined MCL International Prognostic Index; MRD: minimal residual disease; ASCT: autologous stem cell transplantation; HD AraC: high-dose cytarabine-based regimen.
Conclusions
The clinical scenario of MCL has completely changed during the last years due to the availability of highly effective targeted drugs, as well as reliable predictive tools determining the prognostic heterogeneity of such patients. Currently, a high-dose immunochemotherapeutic regimen based on cytarabine and rituximab, supported by ASCT, is the standard of care for younger patients, in spite of its non negligible toxicity. However, recent biological insights on MCL molecular pathogenesis are paving the way for both the development of new drugs and refined prognostication. Therefore, it is likely that in the near future the therapeutic approach in this disease will become more and more personalized, based on the individualized risk of relapse, and potentially ASCT will be reserved only for those cases who will really benefit from this effective, but toxic procedure.
Acknowledgments
The Authors would like to thank Antonella Fiorillo for the excellent secretarial support
Footnotes
Check the online version for the most updated information on this article, online supplements, and information on authorship & disclosures: www.haematologica.org/content/101/2/104
Funding: SF was supported by Progetto di Rilevante Interesse Nazionale (PRIN 2009) from Ministero Italiano dell’Università e della Ricerca (MIUR), Roma, Italy (code: 7.07.02.60 AE01); Progetto di Ricerca Sanitaria Finalizzata 2009, head unit: Divisione di Ematologia S. Cortellazzo, A. O. S. Maurizio, Bolzano/Bozen, Italy (code: RF-2009-1469205); Progetto di Ricerca Sanitaria Finalizzata 2010, (head unit: Divisione di Ematologia, A. O. S. Maurizio, Bolzano/Bozen, Italy, code: RF-2010-2307262), Fondi di Ricerca Locale, Università degli Studi di Torino, Torino, Italy; Fondazione Neoplasie del Sangue (FO. NE. SA), Torino, Italy.
References
- 1.World Health Organization, Swerdlow SH, International Agency for Research on Cancer. WHO classification of tumours of haematopoietic and lymphoid tissues. 4. ed. Lyon: Internat. Agency for Research on Cancer; 2008; 439 S. p [Google Scholar]
- 2.Hiddemann W, Unterhalt M, Herrmann R, et al. Mantle-cell lymphomas have more widespread disease and a slower response to chemotherapy compared with follicle-center lymphomas: results of a prospective comparative analysis of the German Low-Grade Lymphoma Study Group. J Clin Oncol. 1998;16(5):1922–1930. [DOI] [PubMed] [Google Scholar]
- 3.Herrmann A, Hoster E, Zwingers T, et al. Improvement of overall survival in advanced stage mantle cell lymphoma. J Clin Oncol. 2009;27(4):511–518. [DOI] [PubMed] [Google Scholar]
- 4.Dreyling M, Ferrero S, Hermine O. How I manage mantle cell lymphoma. Leukemia. 2014;28(11):2117–2130 [DOI] [PubMed] [Google Scholar]
- 5.Dreyling M. Hyper-CVAD in mantle-cell lymphoma: really “hyper” or just hype? Leuk Lymphoma 2008;49(6):1017–1018. [DOI] [PubMed] [Google Scholar]
- 6.Romaguera JE, Fayad LE, Feng L, et al. Ten-year follow-up after intense chemoimmunotherapy with Rituximab-HyperCVAD alternating with Rituximab-high dose methotrexate/cytarabine (R-MA) and without stem cell transplantation in patients with untreated aggressive mantle cell lymphoma. Br J Haematol. 2010;150(2):200–208. [DOI] [PubMed] [Google Scholar]
- 7.Tarella C, Passera R, Magni M, et al. Risk factors for the development of secondary malignancy after high-dose chemotherapy and autograft, with or without rituximab: a 20-year retrospective follow-up study in patients with lymphoma. J Clin Oncol. 2011;29(7):814–824. [DOI] [PubMed] [Google Scholar]
- 8.Pérez-Galán P, Dreyling M, Wiestner A. Mantle cell lymphoma: biology, pathogenesis, and the molecular basis of treatment in the genomic era. Blood. 2011;117(1):26–38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Jares P, Colomer D, Campo E. Molecular pathogenesis of mantle cell lymphoma. J Clin Invest. 2012;122(10):3416–3423. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Forstpointner R, Dreyling M, Repp R, et al. The addition of rituximab to a combination of fludarabine, cyclophosphamide, mitoxantrone (FCM) significantly increases the response rate and prolongs survival as compared with FCM alone in patients with relapsed and refractory follicular and mantle cell lymphomas: results of a prospective randomized study of the German Low-Grade Lymphoma Study Group. Blood. 2004;104(10):3064–3071. [DOI] [PubMed] [Google Scholar]
- 11.Lenz G, Dreyling M, Hoster E, et al. Immunochemotherapy with rituximab and cyclophosphamide, doxorubicin, vincristine, and prednisone significantly improves response and time to treatment failure, but not long-term outcome in patients with previously untreated mantle cell lymphoma: results of a prospective randomized trial of the German Low Grade Lymphoma Study Group (GLSG). J Clin Oncol. 2005;23(9): 1984–1992. [DOI] [PubMed] [Google Scholar]
- 12.Lefrère F, Delmer A, Suzan F, et al. Sequential chemotherapy by CHOP and DHAP regimens followed by high-dose therapy with stem cell transplantation induces a high rate of complete response and improves event-free survival in mantle cell lymphoma: a prospective study. Leukemia. 2002;16(4):587–593. [DOI] [PubMed] [Google Scholar]
- 13.Romaguera JE, Khouri IF, Kantarjian HM, et al. Untreated aggressive mantle cell lymphoma: results with intensive chemotherapy without stem cell transplant in elderly patients. Leuk Lymphoma. 2000;39(1–2): 77–85. [DOI] [PubMed] [Google Scholar]
- 14.Khouri IF, Romaguera J, Kantarjian H, et al. Hyper-CVAD and high-dose methotrexate/cytarabine followed by stem-cell transplantation: an active regimen for aggressive mantle-cell lymphoma. J Clin Oncol. 1998;16(12):3803–3809. [DOI] [PubMed] [Google Scholar]
- 15.Freedman AS, Neuberg D, Gribben JG, et al. High-dose chemoradiotherapy and anti-B-cell monoclonal antibody-purged autologous bone marrow transplantation in mantle-cell lymphoma: no evidence for long-term remission. J Clin Oncol. 1998;16(1):13–18. [DOI] [PubMed] [Google Scholar]
- 16.Vandenberghe E, Ruiz de Elvira C, Loberiza FR, et al. Outcome of autologous transplantation for mantle cell lymphoma: a study by the European Blood and Bone Marrow Transplant and Autologous Blood and Marrow Transplant Registries. Br J Haematol. 2003;120(5):793–800. [DOI] [PubMed] [Google Scholar]
- 17.Milpied N, Gaillard F, Moreau P, et al. High-dose therapy with stem cell transplantation for mantle cell lymphoma: results and prognostic factors, a single center experience. Bone Marrow Transplant. 1998;22(7):645–650. [DOI] [PubMed] [Google Scholar]
- 18.Dreyling M, Lenz G, Hoster E, et al. Early consolidation by myeloablative radiochemotherapy followed by autologous stem cell transplantation in first remission significantly prolongs progression-free survival in mantle-cell lymphoma: results of a prospective randomized trial of the European MCL Network. Blood. 2005;105(7):2677–2684. [DOI] [PubMed] [Google Scholar]
- 19.Hoster E, Metzner B, Forstpointner R, et al. Autologous Stem Cell Transplantation and Addition of Rituximab Independently Prolong Response Duration in Advanced Stage Mantle Cell Lymphoma. Blood (ASH Annual Meeting Abstracts), 2009; 114:880. [Google Scholar]
- 20.Andersen NS, Donovan JW, Borus JS, et al. Failure of immunologic purging in mantle cell lymphoma assessed by polymerase chain reaction detection of minimal residual disease. Blood. 1997;90(10):4212–4221. [PubMed] [Google Scholar]
- 21.Corradini P, Ladetto M, Zallio F, et al. Long-term follow-up of indolent lymphoma patients treated with high-dose sequential chemotherapy and autografting: evidence that durable molecular and clinical remission frequently can be attained only in follicular subtypes. J Clin Oncol. 2004;22(8):1460–1468. [DOI] [PubMed] [Google Scholar]
- 22.Gianni AM, Magni M, Martelli M, et al. Long-term remission in mantle cell lymphoma following high-dose sequential chemotherapy and in vivo rituximab-purged stem cell autografting (R-HDS regimen). Blood. 2003;102(2):749–755. [DOI] [PubMed] [Google Scholar]
- 23.Geisler CH, Kolstad A, Laurell A, et al. Long-term progression-free survival of mantle cell lymphoma after intensive front-line immunochemotherapy with in vivo-purged stem cell rescue: a nonrandomized phase 2 multicenter study by the Nordic Lymphoma Group. Blood 2008;112(7): 2687–2693. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Pott C, Schrader C, Gesk S, et al. Quantitative assessment of molecular remission after high-dose therapy with autologous stem cell transplantation predicts long-term remission in mantle cell lymphoma. Blood. 2006;107(6):2271–2278. [DOI] [PubMed] [Google Scholar]
- 25.Pott C, Hoster E, Delfau-Larue MH, et al. Molecular remission is an independent predictor of clinical outcome in patients with mantle cell lymphoma after combined immunochemotherapy: a European MCL intergroup study. Blood. 2010;115(16):3215–3223. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Damon LE, Johnson JL, Niedzwiecki D, et al. Immunochemotherapy and autologous stem-cell transplantation for untreated patients with mantle-cell lymphoma: CALGB 59909. J Clin Oncol. 2009;27(36): 6101–6108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.van ‘t Veer MB, de Jong D, MacKenzie M, et al. High-dose Ara-C and beam with auto-graft rescue in R-CHOP responsive mantle cell lymphoma patients. Br J Haematol. 2009;144(4):524–530. [DOI] [PubMed] [Google Scholar]
- 28.Delarue R, Haioun C, Ribrag V, et al. CHOP and DHAP plus rituximab followed by autologous stem cell transplantation in mantle cell lymphoma: a phase 2 study from the Groupe d’Etude des Lymphomes de l’Adulte. Blood. 2013;121(1):48–53. [DOI] [PubMed] [Google Scholar]
- 29.Touzeau C, Leux C, Bouabdallah R, et al. Autologous stem cell transplantation in mantle cell lymphoma: a report from the SFGM-TC. Ann Hematol. 2014;93(2):233–242. [DOI] [PubMed] [Google Scholar]
- 30.Romaguera JE, Fayad L, Rodriguez MA, et al. High rate of durable remissions after treatment of newly diagnosed aggressive mantle-cell lymphoma with rituximab plus hyper-CVAD alternating with rituximab plus high-dose methotrexate and cytarabine. J Clin Oncol. 2005;23(28):7013–7023. [DOI] [PubMed] [Google Scholar]
- 31.Merli F, Luminari S, Ilariucci F, et al. Rituximab plus HyperCVAD alternating with high dose cytarabine and methotrexate for the initial treatment of patients with mantle cell lymphoma, a multicentre trial from Gruppo Italiano Studio Linfomi. Br J Haematol. 2012;156(3):346–353. [DOI] [PubMed] [Google Scholar]
- 32.Bernstein SH, Epner E, Unger JM, et al. A phase II multicenter trial of hyperCVAD MTX/Ara-C and rituximab in patients with previously untreated mantle cell lymphoma; SWOG 0213. Ann Oncol. 2013;24(6):1587–1593. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Abrahamsson A, Albertsson-Lindblad A, Brown PN, et al. Real world data on primary treatment for mantle cell lymphoma: a Nordic Lymphoma Group observational study. Blood. 2014;124(8):1288–1295. [DOI] [PubMed] [Google Scholar]
- 34.Hermine O, Hoster E, Walewski J, et al. Alternating Courses of 3x CHOP and 3x DHAP Plus Rituximab Followed by a High Dose ARA-C Containing Myeloablative Regimen and Autologous Stem Cell Transplantation (ASCT) Increases Overall Survival When Compared to 6 Courses of CHOP Plus Rituximab Followed by Myeloablative Radiochemotherapy and ASCT in Mantle Cell Lymphoma: Final Analysis of the MCL Younger Trial of the European Mantle Cell Lymphoma Network (MCL net). Blood (ASH Annual Meeting Abstracts), 2012;120:151. [Google Scholar]
- 35.Pott C, Hoster E, Beldjord K, et al. R-CHOP/R-DHAP Compared to R-CHOP Induction Followed by High Dose Therapy with Autologous Stem Cell Transplantation Induces Higher Rates of Molecular Remission In MCL: Results of the MCL Younger Intergroup Trial of the European MCL Network. Blood (ASH Annual Meeting Abstracts), 2010;116:965. [Google Scholar]
- 36.Dreyling M, Geisler C, Hermine O, et al. Newly diagnosed and relapsed mantle cell lymphoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2014;25 Suppl 3:iii83–92. [DOI] [PubMed] [Google Scholar]
- 37.National Comprehensive Cancer Network (NCCN) 2015. Guidelines for treatment of cancer: Non-Hodgkin’s Lymphomas (http://www.nccn.org/professionals/physician_gls/f_guidelines.asp#nhl)
- 38.Robinson S, Dreger P, Caballero D, et al. The EBMT/EMCL consensus project on the role of autologous and allogeneic stem cell transplantation in mantle cell lymphoma. Leukemia. 2015;29(2):464–473. [DOI] [PubMed] [Google Scholar]
- 39.Geisler CH, Kolstad A, Laurell A, et al. Nordic MCL2 trial update: six-year followup after intensive immunochemotherapy for untreated mantle cell lymphoma followed by BEAM or BEAC + autologous stem-cell support: still very long survival but late relapses do occur. Br J Haematol. 2012;158(3):355–362. [DOI] [PubMed] [Google Scholar]
- 40.Kolstad A, Laurell A, Jerkeman M, et al. Nordic MCL3 study: 90Y-ibritumomab-tiux-etan added to BEAM/C in non-CR patients before transplant in mantle cell lymphoma. Blood. 2014;123(19):2953–2959. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Kluin-Nelemans HC, Hoster E, Hermine O, et al. Treatment of older patients with mantle-cell lymphoma. N Engl J Med. 2012;367(6):520–531. [DOI] [PubMed] [Google Scholar]
- 42.Le Gouill S, Thieblemont C, Oberic L, et al. Rituximab Maintenance Versus Wait and Watch after Four Courses of R-DHAP Followed By Autologous Stem Cell transplantation in Previously Untreated Young Patients with Mantle Cell Lymphoma: First Interim Analysis of the Phase III Prospective Lyma Trial, a Lysa Study. Blood. 2014;124:146 Abstr. [Google Scholar]
- 43.Goy A, Younes A, McLaughlin P, et al. Phase II study of proteasome inhibitor bortezomib in relapsed or refractory B-cell non-Hodgkin’s lymphoma. J Clin Oncol. 2005;23(4):667–675. [DOI] [PubMed] [Google Scholar]
- 44.O’Connor OA, Wright J, Moskowitz C, et al. Phase II clinical experience with the novel proteasome inhibitor bortezomib in patients with indolent non-Hodgkin’s lymphoma and mantle cell lymphoma. J Clin Oncol. 2005;23(4):676–684. [DOI] [PubMed] [Google Scholar]
- 45.Fisher RI, Bernstein SH, Kahl BS, et al. Multicenter phase II study of bortezomib in patients with relapsed or refractory mantle cell lymphoma. J Clin Oncol. 2006;24(30):4867–4874. [DOI] [PubMed] [Google Scholar]
- 46.Goy A, Bernstein SH, Kahl BS, et al. Bortezomib in patients with relapsed or refractory mantle cell lymphoma: updated time-to-event analyses of the multicenter phase 2 PINNACLE study. Ann Oncol. 2009;20(3):520–525. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Weigert O, Weidmann E, Mueck R, et al. A novel regimen combining high dose cytarabine and bortezomib has activity in multiply relapsed and refractory mantle cell lymphoma - long-term results of a multicenter observation study. Leuk Lymphoma. 2009; 50(5):716–722. [DOI] [PubMed] [Google Scholar]
- 48.Gerecitano J, Portlock C, Hamlin P, et al. Phase I trial of weekly and twice-weekly bortezomib with rituximab, cyclophosphamide, and prednisone in relapsed or refractory non-Hodgkin lymphoma. Clin Cancer Res. 2011;17(8):2493–2501. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Friedberg JW, Vose JM, Kelly JL, et al. The combination of bendamustine, bortezomib, and rituximab for patients with relapsed/refractory indolent and mantle cell non-Hodgkin lymphoma. Blood. 2011;117(10):2807–2812. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Ruan J, Martin P, Furman RR, et al. Bortezomib plus CHOP-rituximab for previously untreated diffuse large B-cell lymphoma and mantle cell lymphoma. J Clin Oncol. 2011;29(6):690–697. [DOI] [PubMed] [Google Scholar]
- 51.Robak T, Huang H, Jin J, et al. Bortezomib-based therapy for newly diagnosed mantle-cell lymphoma. N Engl J Med. 2015;372(10):944–953. [DOI] [PubMed] [Google Scholar]
- 52.Hess G, Herbrecht R, Romaguera J, et al. Phase III study to evaluate temsirolimus compared with investigator’s choice therapy for the treatment of relapsed or refractory mantle cell lymphoma. J Clin Oncol. 2009;27(23):3822–3829. [DOI] [PubMed] [Google Scholar]
- 53.Ansell SM, Tang H, Kurtin PJ, et al. Temsirolimus and rituximab in patients with relapsed or refractory mantle cell lymphoma: a phase 2 study. Lancet Oncol. 2011;12(4):361–368. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Hess G, Keller U, Scholz CW, et al. Safety and efficacy of Temsirolimus in combination with Bendamustine and Rituximab in relapsed mantle cell and follicular lymphoma. Leukemia. 2015;29(8):1695–1701. [DOI] [PubMed] [Google Scholar]
- 55.Wiernik PH, Lossos IS, Tuscano JM, et al. Lenalidomide monotherapy in relapsed or refractory aggressive non-Hodgkin’s lymphoma. J Clin Oncol. 2008;26(30):4952–4957. [DOI] [PubMed] [Google Scholar]
- 56.Witzig TE, Vose JM, Zinzani PL, et al. An international phase II trial of single-agent lenalidomide for relapsed or refractory aggressive B-cell non-Hodgkin’s lymphoma. Ann Oncol. 2011;22(7):1622–1627. [DOI] [PubMed] [Google Scholar]
- 57.Eve HE, Carey S, Richardson SJ, et al. Single-agent lenalidomide in relapsed/refractory mantle cell lymphoma: results from a UK phase II study suggest activity and possible gender differences. Br J Haematol. 2012;159(2):154–163. [DOI] [PubMed] [Google Scholar]
- 58.Zaja F, De Luca S, Vitolo U, et al. Salvage treatment with lenalidomide and dexamethasone in relapsed/refractory mantle cell lymphoma: clinical results and effects on microenvironment and neo-angiogenic biomarkers. Haematologica. 2012;97(3):416–422. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Goy A, Sinha R, Williams ME, et al. Single-agent lenalidomide in patients with mantle-cell lymphoma who relapsed or progressed after or were refractory to bortezomib: phase II MCL-001 (EMERGE) study. J Clin Oncol. 2013;31(29):3688–3695. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Wang M, Fayad L, Wagner-Bartak N, et al. Lenalidomide in combination with rituximab for patients with relapsed or refractory mantle-cell lymphoma: a phase 1/2 clinical trial. Lancet Oncol. 2012;13(7):716–723. [DOI] [PubMed] [Google Scholar]
- 61.Zaja F, Ferrero S, Stelitano C, et al. Rituximab, lenalidomide, bendamustine second line therapy in mantle cell lymphoma: a phase II study of the Fondazione Italiana Linfomi (FIL). Hematol Oncol. 2015;33:100–180. (ICML Meeting Abstract 014). [Google Scholar]
- 62.Albertsson-Lindblad A, Kolstad A, Laurell A, et al. Lenalidomide-rituximab-bendamustine in first line for patients > 65 with mantle cell lymphoma: final results of the Nordic Lymphoma Group MCL4 (LENA-BERIT) phase I/II trial. Hematol Oncol. 2015; 33:100–180. (ICML Meeting Abstract 060). [Google Scholar]
- 63.Wang ML, Rule S, Martin P, et al. Targeting BTK with ibrutinib in relapsed or refractory mantle-cell lymphoma. N Engl J Med. 2013;369(6):507–516. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Kahl BS, Spurgeon SE, Furman RR, et al. A phase 1 study of the PI3Kδ inhibitor idelalisib in patients with relapsed/refractory mantle cell lymphoma (MCL). Blood 2014;123(22):3398–3405. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Magni M, Di Nicola M, Carlo-Stella C, et al. Safety, Tolerability and Activity of Ofatumumab, Bendamustine and Dexamethasone Combination As First-Line Treatment of Mantle-Cell Lymphoma in the Elderly: A Multicenter Study. Blood (ASH Annual Meeting Abstracts), 2011;118:1647. [Google Scholar]
- 66.Vose JM, Loberiza FR, Bociek G, Bierman P, James O. Armitage. Phase I/II Trial of Ofatumumab/Lenalidamide for Patients with Relasped/Refractory B-Cell Non-Hodgkin Lymphoma: High Response Rate in Indolent Lymphoma. Blood (ASH Annual Meeting Abstracts). 2012;120:3692. [Google Scholar]
- 67.Morschhauser FA, Cartron G, Thieblemont C, et al. Obinutuzumab (GA101) monotherapy in relapsed/refractory diffuse large b-cell lymphoma or mantle-cell lymphoma: results from the phase II GAUGUIN study. J Clin Oncol. 2013;31(23):2912–2919. [DOI] [PubMed] [Google Scholar]
- 68.Bargou R, Leo E, Zugmaier G, et al. Tumor regression in cancer patients by very low doses of a T cell-engaging antibody. Science. 2008;321(5891):974–977. [DOI] [PubMed] [Google Scholar]
- 69.Viardot A, Goebeler M, Scheele JS, et al. Treatment of Patients with Non-Hodgkin Lymphoma (NHL) with CD19/CD3 Bispecific Antibody Blinatumomab (MT103): Double-Step Dose Increase to Continuous Infusion of 60 μg/m2/d Is Tolerable and Highly Effective. Blood (ASH Annual Meeting Abstracts). 2010;116:2880. [Google Scholar]
- 70.Palanca-Wessels MC, Czuczman M, Salles G, et al. Safety and activity of the anti-CD79B antibody-drug conjugate polatuzumab vedotin in relapsed or refractory B-cell non-Hodgkin lymphoma and chronic lymphocytic leukaemia: a phase 1 study. Lancet Oncol. 2015;16(6):704–715. [DOI] [PubMed] [Google Scholar]
- 71.Lin TS, Blum KA, Fischer DB, et al. Flavopiridol, fludarabine, and rituximab in mantle cell lymphoma and indolent B-cell lymphoproliferative disorders. J Clin Oncol. 2010;28(3):418–423. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Holkova B, Perkins EB, Ramakrishnan V, et al. Phase I trial of bortezomib (PS-341; NSC 681239) and alvocidib (flavopiridol; NSC 649890) in patients with recurrent or refractory B-cell neoplasms. Clin Cancer Res. 2011;17(10):3388–3397. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Leonard JP, LaCasce AS, Smith MR, et al. Selective CDK4/6 inhibition with tumor responses by PD0332991 in patients with mantle cell lymphoma. Blood. 2012;119(20): 4597–4607. [DOI] [PubMed] [Google Scholar]
- 74.Davids MS, Seymour JF, Gerecitano JF, et al. The Single-Agent Bcl-2 Inhibitor ABT-199 (GDC-0199) In Patients With Relapsed/Refractory (R/R) Non-Hodgkin Lymphoma (NHL): Responses Observed In All Mantle Cell Lymphoma (MCL) Patients. Blood (ASH Annual Meeting Abstracts). 2013;122:1789. [Google Scholar]
- 75.Evens AM, Vose JM, Harb W, et al. A Phase II Multicenter Study of the Histone Deacetylase Inhibitor (HDACi) Abexinostat (PCI-24781) in Relapsed/Refractory Follicular Lymphoma (FL) and Mantle Cell Lymphoma (MCL). Blood (ASH Annual Meeting Abstracts). 2012;120:55. [Google Scholar]
- 76.Hoster E, Dreyling M, Klapper W, et al. A new prognostic index (MIPI) for patients with advanced-stage mantle cell lymphoma. Blood. 2008;111(2):558–565. [DOI] [PubMed] [Google Scholar]
- 77.Geisler CH, Kolstad A, Laurell A, et al. The Mantle Cell Lymphoma International Prognostic Index (MIPI) is superior to the International Prognostic Index (IPI) in predicting survival following intensive first-line immunochemotherapy and autologous stem cell transplantation (ASCT). Blood. 2010; 115(8):1530–1533. [DOI] [PubMed] [Google Scholar]
- 78.Hoster E, Klapper W, Hermine O, et al. Confirmation of the mantle-cell lymphoma international prognostic index in randomized trials of the European mantle-cell lymphoma network. J Clin Oncol. 2014;32(13):1338–1346. [DOI] [PubMed] [Google Scholar]
- 79.Determann O, Hoster E, Ott G, et al. Ki-67 predicts outcome in advanced-stage mantle cell lymphoma patients treated with anti-CD20 immunochemotherapy: results from randomized trials of the European MCL Network and the German Low Grade Lymphoma Study Group. Blood. 2008;111(4):2385–2387. [DOI] [PubMed] [Google Scholar]
- 80.Dreyling M, Ferrero S, Vogt N, Klapper W; European Mantle Cell Lymphoma Network. New paradigms in mantle cell lymphoma: is it time to risk-stratify treatment based on the proliferative signature? Clin Cancer Res 2014;20(20):5194–5206. [DOI] [PubMed] [Google Scholar]
- 81.Hoster E, Rosenwald A, Berger F, et al. Prognostic value of proliferation, cytology, and growth pattern in mantle cell lymphoma: results from randomized trials of the European MCL Network. Hematol Oncol. 2015;33:100–180. (ICML Meeting Abstract 058). [DOI] [PubMed] [Google Scholar]
- 82.Klapper W, Hoster E, Determann O, et al. Ki-67 as a prognostic marker in mantle cell lymphoma-consensus guidelines of the pathology panel of the European MCL Network. J Hematop. 2009;2(2):103–111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Husby S, Ralfkiaer U, Garde C, et al. miR-18b overexpression identifies mantle cell lymphoma patients with poor outcome and improves the MIPI-B prognosticator. Blood. 2015;125(17):2669–2677. [DOI] [PubMed] [Google Scholar]
- 84.Pott C, Macintyre E, Delfau-Larue MH, et al. MRD Eradication Should be the Therapeutic Goal in Mantle Cell Lymphoma and May Enable Tailored Treatment Approaches: Results of the Intergroup Trials of the European MCL Network. Blood. 2014;124: 147 Abstr. [Google Scholar]
- 85.Andersen NS, Pedersen LB, Laurell A, et al. Pre-emptive treatment with rituximab of molecular relapse after autologous stem cell transplantation in mantle cell lymphoma. J Clin Oncol. 2009;27(26):4365–4370. [DOI] [PubMed] [Google Scholar]
- 86.Ferrero S, Monitillo L, Mantoan B, et al. Rituximab-based pre-emptive treatment of molecular relapse in follicular and mantle cell lymphoma. Ann Hematol. 2013;92(11):1503–1511. [DOI] [PubMed] [Google Scholar]
- 87.van der Velden VH, Cazzaniga G, Schrauder A, et al. Analysis of minimal residual disease by Ig/TCR gene rearrangements: guidelines for interpretation of real-time quantitative PCR data. Leukemia. 2007;21(4):604–611. [DOI] [PubMed] [Google Scholar]
- 88.Laurell A, Kolstad A, Jerkeman M, Räty R, Geisler CH. High dose cytarabine with rituximab is not enough in first-line treatment of mantle cell lymphoma with high proliferation: early closure of the Nordic Lymphoma Group Mantle Cell Lymphoma 5 trial. Leuk Lymphoma. 2014;55(5):1206–1208. [DOI] [PubMed] [Google Scholar]
- 89.Beà S, Valdés-Mas R, Navarro A, et al. Landscape of somatic mutations and clonal evolution in mantle cell lymphoma. Proc Natl Acad Sci USA. 2013;110(45):18250–18255. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Navarro A, Clot G, Royo C, et al. Molecular subsets of mantle cell lymphoma defined by the IGHV mutational status and SOX11 expression have distinct biologic and clinical features. Cancer Res. 2012;72(20):5307–5316. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Nygren L, Baumgartner Wennerholm S, Klimkowska M, Christensson B, Kimby E, Sander B. Prognostic role of SOX11 in a population-based cohort of mantle cell lym phoma. Blood. 2012;119(18):4215–4223. [DOI] [PubMed] [Google Scholar]
- 92.Kridel R, Meissner B, Rogic S, et al. Whole transcriptome sequencing reveals recurrent NOTCH1 mutations in mantle cell lymphoma. Blood. 2012;119(9):1963–1971. [DOI] [PubMed] [Google Scholar]
- 93.Nordström L, Sernbo S, Eden P, et al. SOX11 and TP53 add prognostic information to MIPI in a homogenously treated cohort of mantle cell lymphoma–a Nordic Lymphoma Group study. Br J Haematol. 2014;166:98–108 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Delfau-Larue MH, Klapper W, Berger F, et al. CDKN2A and TP53 deletions predict adverse outcome in younger mantle cell lymphoma patients, independent of treatment and MIPI. Blood. 2015;126(5):604–611. [DOI] [PubMed] [Google Scholar]
- 95.Martin P, Chadburn A, Christos P, et al. Outcome of deferred initial therapy in mantle-cell lymphoma. J Clin Oncol. 2009;27(8):1209–1213. [DOI] [PubMed] [Google Scholar]
- 96.Fernàndez V, Salamero O, Espinet B, et al. Genomic and gene expression profiling defines indolent forms of mantle cell lymphoma. Cancer Res. 2010;70(4):1408–1418. [DOI] [PubMed] [Google Scholar]
- 97.Ribera-Cortada I, Martinez D, Amador V, et al. Plasma cell and terminal B-cell differentiation in mantle cell lymphoma mainly occur in the SOX11-negative subtype. Mod Pathol. 2015;28(11):1435–1447. [DOI] [PubMed] [Google Scholar]
- 98.Visco C, Finotto S, Zambello R, et al. Combination of rituximab, bendamustine, and cytarabine for patients with mantle-cell non-Hodgkin lymphoma ineligible for intensive regimens or autologous transplantation. J Clin Oncol. 2013;31(11):1442–1449. [DOI] [PubMed] [Google Scholar]
- 99.Cortelazzo S, Martelli M, Ladetto M, et al. High dose sequential chemotherapy with rituximab and ASCT as first line therapy in adult MCL patients: clinical and molecular response of the MCL0208 trial, a FIL study. Haematologica. 2015;100(s1):3–4.25552677 [Google Scholar]
- 100.Sarkozy C, Terré C, Jardin F, et al. Complex karyotype in mantle cell lymphoma is a strong prognostic factor for the time to treatment and overall survival, independent of the MCL international prognostic index. Genes Chromosomes Cancer. 2014;53(1): 106–116. [DOI] [PubMed] [Google Scholar]
- 101.Curran KJ, Brentjens RJ. Chimeric antigen receptor T cells for cancer immunotherapy. J Clin Oncol. 2015;33(15):1703–1706. [DOI] [PubMed] [Google Scholar]
- 102.Cheah CY, Chihara D, Romaguera JE, et al. Patients with mantle cell lymphoma failing ibrutinib are unlikely to respond to salvage chemotherapy and have poor outcomes. Ann Oncol. 2015;26(6):1175–1179. [DOI] [PubMed] [Google Scholar]