

Abstract
Adolescents are among the most frequent users of social media websites, raising concern about the dangers of cyber bullying or cybervictimization (CV). A 12-month longitudinal study examined the unique, prospective relation of CV to the development of negative self-cognitions and depressive symptoms in a community sample of 827 children and young adolescents (ages 8-13; 55.1% female) from the southeastern United States. Over and above conventional types of peer victimization, CV significantly predicted changes in self-referential negative cognitions, victimization-related cognitive reactions, and depressive symptoms, even after controlling for baseline levels of the dependent variables. Results also showed that CV was significantly less stable than other forms of victimization and tended to increase slightly with time. The study highlights the unique effects of CV and has implications for research and practice.
Keywords: Cyber bullying, Internet, Peer victimization, Depression, Self-esteem
As adolescents’ use of social media has grown, so has concern about the dangers of CV (CV) by one’s peers. Although the definition of CV varies across researchers, most agree that it involves an intentional act to inflict harm on another using electronic media (Leung & McBride-Chang, 2013; Smith et al., 2008; Sontag, Clemans, Graber, & Lyndon, 2011; Williford et al., 2013). Specific behaviors include, but are not limited to, posting compromising material on social media websites, harassment via instant messaging or text messaging, and so on. Several studies have shown that the experience of CV is associated with a wide variety of serious psychological outcomes, including the development of maladaptive self-cognitions that can predispose youths to depression and related problems. Most of this concern, however, has been generated by cross-sectional, correlational studies, very few of which have examined the incremental effects of CV over and above other forms of peer victimization. The overarching goal of the current study was to examine the unique, prospective relation of CV to the development of negative self-cognitions and depressive symptoms in young adolescents, while controlling for other forms of peer victimization. Secondary goals were to examine fundamental, longitudinal characteristics of CV in young adolescents, as well as correlations with age and gender.
Based on cross-sectional research, public concern about CV is warranted. CV correlates with anxiety, low self-esteem, loneliness, depression (particularly in females), suicide attempts, externalizing symptoms, reactive and instrumental aggression, problematic peer relations, poor social skills, school absenteeism, academic under-achievement, low life satisfaction, and physical problems (Bauman, Toomey, & Walker, 2013; Campbell, Spears, Slee, Butler, & Kift, 2012; Dooley, Shaw, & Cross, 2012; Gámez-Guadix, Orue, Smith, & Calvete, 2013; Kessel Schneider, O’Donnell, Stueve, & Coulter, 2012; Kowalski & Limber, 2013; Leung & McBride-Chang, 2013; Nordahl, Beran, & Dittrick, 2013; Olenik-Shemesh, Heiman, & Eden, 2012; Perren, Dooley, Shaw, & Cross, 2010; Price, Chin, Higa-McMillan, Kim, & Frueh, 2013; Schultze-Krumbholz, Jäkel, Schultze, & Scheithauer, 2012; Turner, Exum, Brame, & Holt, 2013; Wang, Nansel, & Iannotti, 2011). Previous theory and research suggest that three conditions mediate the effects of negative life events on the emergence of negative self-cognitions and depressive symptoms in young people. The first pertains to focused attention on negative self-relevant information. From works by Ingram (1990) and Mogg and Bradley (2005), we see that sustained, rigid, self-focused attention is a risk factor for a wide range of psychological disorders, including depression. Cole et al. (2014) noted, “Life events that compel attention to negative self-relevant information should be especially important in the construction of depressive self-schemas” (p. 150). Second, the generative events must evoke strong negative affect. Drawing on reviews by Scher, Ingram, and Segal (2005) and Segal and Ingram (1994), Cole et al. concluded that the connection between negative self-schemas and negative mood is a learned association, “taught” to the child via events that simultaneously evoke negative affect and convey negative self-relevant information (Bell & Wolfe, 2004, p. 366; Cole et al., 2014). The third condition is recurrence. Learning maladaptive associations requires repetition (Cole, 1991; Harter, 1999; Masten, Best, & Garmezy, 1990). When levels of peer victimization are high, all three of the ingredients for the construction of depressive schemas are present.
Understanding the relation of CV to depression-related outcomes is especially important during early adolescence. Teenagers are among the most frequent users of social media websites, with 81% of American 12- to 17-year-olds reporting that they use social networking sites (Pew Research Center, 2014). Many of these young people are just beginning to develop an online presence; as such, their online social skills are often not well-developed. Furthermore, early adolescence is a critical period for the construction of self-esteem and self-perceived competence (Harter, 1999). Consequently, early adolescence is a period when youths may be especially vulnerable to the effects of peer victimization in general and cybervictimization in particular.
Among adolescents, adverse outcomes have been associated with a wide range of peer victimization behaviors (Cole et al., 2014; Gibb et al., 2006; Sinclair et al., 2012). Of these, relational victimization appears to be the most toxic. Relational victimization is defined as behavior that damages peer relationships, friendships, and social acceptance often by excluding the victim from peer activities, withdrawing friendship, or spreading rumors (Hawker & Boulton, 2000). Its particular toxicity may be due to the facts that relational victimization is difficult to defend against, the perpetrator is often unknown, and it thwarts an almost basic need for social belongingness (Cole et al., 2014). CV has these same characteristics, as well as others: CV is virtually impossible to undo; it can be disseminated quickly to a large number of people; and it can reach victims almost regardless of location.
A few cross-sectional studies have addressed the question of whether CV is a qualitatively different type of victimization that explains unique variance in problematic outcomes, over and above other forms of peer victimization. Results have been mixed. Bonanno and Hymel’s (2013) study of 399 Canadian adolescents in grades eight to 10 demonstrated that CV explained variance in depressive symptoms over and above physical, verbal, and social victimization (as well as gender). Similarly, Perren et al.’s (2010) investigation of CV in 1320 Australian and 374 Swiss adolescents in grades seven to nine showed that CV predicted depressive symptoms over and above relational, verbal, physical, and property-related victimization (as well as age, gender, country, and bullying perpetration). Bauman et al.’s (2013) study of 1491 American high school students showed that CV was related to depressive symptoms after controlling for school-based harassment and bullying (as well as bullying perpetration) but only for females. Turner et al.’s (2013) research on a sample of sixth to 12th graders also revealed a significant relation between CV and depressive symptoms for females only, after controlling for verbal and physical victimization (as well as a variety of other covariates). Dempsey, Sulkowski, Nichols, and Storch’s (2009) study of 1684 southern US adolescents reported that CV was not significantly related to symptoms of depression after controlling statistically for relational and overt peer victimization (as well as gender). The diversity of these results is confusing but may be due to the fact that each study used different control variables and thus actually addressed somewhat different questions.
Five studies provide have examined the relation of CV to either depressive symptoms or closely related variables in younger adolescents (age 9-13; Dooley et al., 2012; Jackson & Cohen, 2012; Machmutow, Perren, Sticca, & Alsaker 2012; Price et al., 2013; Völlink, Bolman, Dehue, & Jacobs, 2013). Most provide preliminary evidence of the expected relation; however, most of these studies are cross-sectional not longitudinal, some utilized new study-specific measures without strong psychometric support, some elected to dichotomize continuous variables, and most did not control for more conventional forms of victimization when examining the role of CV.
Two studies were longitudinal but did not examine the incremental predictive utility of CV over and above other types of peer victimization. Gámez-Guadix et al.’s (2013) study of 845 Spanish adolescents found that CV at time 1 significantly predicted increased depressive symptoms 6 months later. They statistically controlled for time 1 levels of depressive symptoms (as well as a measure of problematic Internet use). Schultze-Krumbholz et al.’s (2012) study of 233 German adolescents showed that over two to six months, CV predicted depressive symptoms for girls but not boys.
Only three longitudinal studies examined the incremental predictive effects of CV over and above other forms of peer victimization. One was Machmutow et al.’s (2012) two-wave study (spanning five to six months) of 767 Swiss adolescents (mean age = 13.18 years). They measured CV using a six-item scale developed specifically for the study. CV predicted change in depressive symptoms over and above a well-validated measure of victimization, but only when victimization was measured at time 2 (not time 1). Salmivalli , Sainio, and Hodges’ (2013) large sample, two-wave study of Finnish students (some in grades 3-5) reported that CV had no longitudinal effect on depression over and above traditional peer victimization; however, CV was measured with a single questionnaire item and depression was measured with only a subset of seven items from the Beck Depression Inventory. The third study was an unpublished dissertation by Landoll (2012) that measured CV using a novel 20-item version of the Cyber Victimization Scale for Adolescents (Landoll & La Greca, 2010) in a sample of 1045 Southeastern US adolescents (mean age = 15.80 years) at two time points six weeks apart. CV at time 1 predicted depressive symptoms (controlling for prior depressive symptoms), over and above time 1 traditional victimization. Taken together, these studies provide preliminary support for the possible incremental predictive effects of CV over more conventional forms of peer victimization.
Consequently, our primary hypothesis was that experiences of CV would be prospectively related to negative self-cognitions and depressive symptoms over and above other forms of peer victimization. By controlling statistically for other forms of peer victimization, we focus attention on the unique effects of CV on negative self-cognitive outcomes related to depression. In this endeavor, we focused on three broad types of outcome variables: (1) Some kinds of negative self-cognitions represent only small cognitive steps from the victimization experience itself (e.g., “If someone picked on me, I would think, ‘He’ll never like me’”); (2) Other kinds of negative self-cognitions represent much larger cognitive leaps of over-generalization (e.g., “Nobody will ever like me”); (3) Still other outcome variables represent depression symptoms per se, not just cognitive precursors to depression. We tested all three.
One reason given for the particularly pernicious nature of CV is that things posted on the Internet are not retractable. This may be true, but after a relatively short amount of time, even viral postings often become relatively difficult to find, as they become buried amongst virtual tons of Internet data. As most postings (and most incidences of CV) have relatively short half-lives, a more important concern is the degree to which being the recipient of CV is a stable, recurring phenomenon. Among eight studies of CV stability, estimates range greatly. Machmutow et al. (2012) reported that CV levels were moderately stable over a six-month interval; however, the majority of Smith et al.’s (2008) sample reported that CV lasted one month or less. Cappadocia, Craig, and Pepler’s (2013) study noted that 11.6% of their sample experienced CV at only one of two yearly time points, whereas a scant 1.9% of their sample experienced CV at both time points. Wang et al. (2011) found that 5.6% of participants experienced CV once or twice over a 2-month interval. Wang, Ianotti, Luke, and Nansel (2010) found that 10.1% of participants experienced CV at least once over a similar time span, whereas Price et al. (2013) found that 7% experienced CV at least 2-3 times. Focusing on a one-month interval, Dempsey (2009) found that 14% of participants experienced CV at least once. Gan et al. (2014) reported the incidence of CV as 18% for “this year.” Absolute stability estimates can vary enormously as a function of time lag and type of measure. A more meaningful concept may be the relative stability of CV vis-à-vis other types of peer victimization over the same period of time. Consequently, our second goal was to not just to estimate but compare 12-month stability estimates for multiple types of peer victimization.
Also unclear is the relation of CV to demographic characteristics, such as sex and age. Many studies have found that CV is significantly more common among girls than boys (e.g., Campbell et al., 2012; Cappadocia et al., 2013; Dempsey et al., 2009; Landoll, 2012; Machmutow et al., 2012; Olenik-Shemesh et al., 2012; Perren et al., 2010; Smith et al., 2008, Study 1; Williford et al., 2013); however, other studies have found no significant difference (e.g., Bauman et al., 2013; Bonanno & Hymel, 2013; Machmutow et al., 2012; Schultze-Krumbholz et al., 2012; Smith et al., 2008; Sontag et al., 2011; Turner et al., 2013). The relation of age to CV is less studied, and the results are inconsistent. One study found that CV is significantly more common in older adolescents (Bauman et al., 2013); a second study reported that CV was significantly more common in younger adolescents (Landoll, 2012); and a third study reported no significant age differences in CV (Smith et al., 2008). Because of these disparities, a third goal of the current study was to examine the relation of age and gender to CV as well as other types of peer victimization. In selecting an age range for the current study, we were mindful of the fact that most types of peer victimization diminish with age (Nansel et al., 2001). The strongest test of hypotheses about CV would be before other types of peer victimization have begun to abate (i.e., at later ages, other types of victimization would be weaker competitors with CV). Consequently, we focused the current study on middle childhood and early adolescence.
In sum, three goals motivated the current study. One was to test the hypothesis that CV is prospectively related to negative self-cognitions and depressive symptoms over and above other forms of peer victimization. The second was to estimate and compare 12-month stabilities of multiple types of peer victimization. The third goal was to examine the relation of age and gender to CV and other types of more conventional peer victimization.
Methods
Participants
Participants included 827 students from four public middle schools and two public elementary schools in middle Tennessee. The full sample was 55.1% female and ethnically diverse: 35.8% African American, 6.0% Asian or Asian American, 58.8% Caucasian, 9.2% Hispanic American, and 13.3% Other (percentages do not sum to 100 as participants could select more than one race/ethnicity). Participants were in grades 3 to 6 at the beginning of the study; their mean age was 10.90 years (SD = 1.18).
At the first wave, 571 students participated in the study. At wave 2, we lost 186 participants due to attrition and recruited 256 new participants. Reasons for attrition were very similar to reasons for addition: moving into or out of the school district and being absent from school at one wave or the other. Participants with complete data were significantly more likely to be female (63.2% vs. 52.8%; χ2(1) = 6.33, p = .01) and Caucasian (68.6% vs. 55.9%; χ2(1) = 9.60, p < .01). In all analyses, we used full information maximum likelihood estimation (FIML) methods so as to include participants with partial data. Under the assumption that the data are missing at random, FIML yields estimates that are less biased and more consistent than the estimates generated by other methods (e.g., single imputation or listwise deletion).
Measures
Peer Victimization
Peer victimization was assessed via the Peer Victimization Self-Report (PVSR; Cole et al., 2014; Sinclair et al., 2012). Four questions focus on each of five types of victimization: cyber, relational, physical, verbal, and property-related. (Five additional questions focused on peer social support but were not examined in the current study). For each question, the stem was “How often have kids done these things to you this year and last year?” Participants marked separate responses about victimization in the current year and in the preceding year. An example item for the cyber victimization subscale is “…put lies about you on the Internet.” For both this year and last year, items were rated on 4-point scales (0 = never, 1 = rarely, 2 =sometimes, 3 = a lot). Confirmatory factor analyses have shown excellent item-level convergent and discriminant validity (Cole et al., 2014). For each type of victimization, we summed the responses about the current and previous year. At wave 1, Cronbach’s alphas ranged from .84 to .85 for the five victimization subscales.
Depressive Symptoms
The second edition of the Reynolds Adolescent Depression Scale – Version 2 (RADS-2; Reynolds, 2002) is a 30-item self-report inventory designed to assess depressive symptoms in youth. Participants respond to a series of items (e.g., “I feel lonely”; “I feel I am no good”) by indicating how often they have particular symptoms (1 = almost never, to 4 = most of the time). The questionnaire does not refer to a particular time period; rather respondents are instructed to note how they “usually feel.” Scores from the RADS-2 yield four subscale scores and a total score. In the current study, we used only the total score. In previous studies of school-age samples, the RADS-2 had three-week test–retest reliability of .87, strong criterion-related validity, and Cronbach’s alphas of .91 to .93, (Reynolds & Mazza, 1998). The measure has strong validity and reliability in clinical and nonclinical samples of children and adolescents (Reynolds, 2002) and has been used successfully with children as young as 9 years old (Laurent, Joiner, & Catanzaro, 2011; Painter, 2012). In our sample, the measure showed excellent internal consistency (Cronbach’s alpha = .91 at wave 1 and .93 at wave 2).
General negative cognitions
The Children’s Automatic Thoughts Scale (CATS; Schniering & Rapee, 2002) is a 40-item self-report measure designed to assess the frequency of negative automatic thoughts in children and adolescents ages 8-17. Participants note how often they have experienced specific negative cognitions within the past week (0 = not at all to 4 = all the time). Confirmatory factor analysis in the initial community sample revealed four factors underlying these cognitions: physical threat (e.g., “I’m going to get hurt”), social threat (e.g., “I look like an idiot”), personal failure (e.g., “It’s my fault that things have gone wrong”) and hostile intent (e.g., “Most people are against me”). In the original sample, subscales based on these factors showed good to excellent internal consistency (Cronbach’s alphas .85-.92) and acceptable test-retest reliability (.66-.80) at 1 and 3 months. The CATS total scale and subscales have shown good to excellent internal consistency in other clinical and community samples (e.g., Micco & Ehrenreich, 2009; Schniering & Lyneham, 2007). For waves 1 and 2 of the present study, Cronbach’s alphas were .87 and .86 for physical threat, .93 and .92 for social threat, .93 and .91 for personal failure, and .84 and .82 for hostile intent, respectively.
Victimization-related cognitive reactions
The Behind Your Back protocol (BYB; Cole et al., 2014) is a measure of negative cognitive reactions to (hypothetical) peer victimization scenarios. The instrument and its development are described in Cole et al. (2014). Briefly, the measure consists of 21 audio recordings of short conversations between a boy and a girl talking about a third person. Study participants are asked to imagine that they are the third person being discussed as they listen to the recordings and follow along on a printed version of the scenarios. (Male and female study participants receive separate versions of the BYB with the appropriate gendered pronouns for the third person. Otherwise, the versions are identical.) Scenarios range from mild to harsh intensity. A mild example is:
Speaker 1: Everyone was laughing at him.
Speaker 2: Well, he did look like an idiot.
Speaker 1: It’s not his fault. Everyone messes up sometimes.
Speaker 2: I guess you’re right, it could’ve happened to anyone.
A harsh example is:
Speaker 1: Oh no, look. She’s bringing her lunch over here.
Speaker 2: She’s going to want to sit by us.
Speaker 1: No way. What should we do?
Speaker 2: Let’s spread out so there’s no room.
After each scenario, participants rate how they would feel and what they would think if they heard two people saying this about them. Only the cognition ratings were used in the current study. Cognitions varied by scenario: for example, “If you heard this [the scenario above], how much would it make you think, ‘I am an idiot’ or ‘I don’t like myself.’” Cognitive ratings were scored on 5-point Likert scales (1 = not at all to 5 = a lot). Exploratory factor analysis showed a single latent factor underlying all of the cognition questions (Cole et al., 2014). Thus, we summed the responses for the cognitive questions as a measure of negative victimization-related self-cognitions. Internal consistency for the total self-cognition scale at both times was excellent (Cronbach’s alpha = .97).
Procedure
After obtaining IRB approval for the study, we approached principals and guidance counselors at each school to ask for written permission to recruit students at their school. After receiving permission, senior research assistants went to each classroom within grades three through six (55 classrooms total) to explain the study and distribute parental consent forms. At wave 2, all available students were given a consent form and invited to participate regardless of whether they had participated the year before. To incentivize return of the consent forms, we gave teachers $100 to use in their classrooms if 90% of their students returned a signed form either granting or denying permission. In all, 911 out of 1251 students returned consent forms, and 827 parents granted permission for their child to participate in the study.
Both waves of data collection at all of the schools took place over a six-week period in the spring semester. On each data collection day, research assistants (graduate students, advanced undergraduate students, and one research staff member) escorted 20 to 30 consented students to a central room at the school (typically the library or cafeteria). A research team member described the study, answered questions about the study, and administered assent forms. Each participant received pencil-and-paper copies of the questionnaires (order was counterbalanced by group). A research assistant read the questions aloud while participants followed along and marked their answers. Other research assistants circulated around the room to answer questions and monitor participants for signs of distraction or distress (none showed signs of distress). For the BYB task, the research team passed out headphones and MP3 players. Participants listened to the scenarios while following along and marking their responses on the questionnaire after each scenario.
Once all participants had completed the measures, they were given a snack and decorative pencil. A research team member then escorted the students back to their classroom. The entire procedure lasted about 45 minutes. After each data collection, trained research assistants reviewed all responses and alerted school guidance counselors if respondents endorsed clinically significant depressive symptoms. Counselors were notified regarding 39 students after wave 1 and 31 students after wave 2. (Consent forms provided for limited confidentiality, and explained the circumstances under which we would contact school counselors.)
Results
Descriptive Statistics
Correlations, means, and standard deviations of all wave 1 and wave 2 study variables appear in Table 1. Descriptive statistics are similar to other school-based studies of middle school students (Cole et al., 2015; Gillham et al., 2012; Schniering & Rapee, 2002). In all but one instance, time 1 measures of victimization were significantly correlated with all time-1 and time-2 measures of negative cognition and depressive symptoms; only the correlation between time-1 property-related peer victimization and time-2 BYB scores was not significant. Additionally, the majority of participants reported experiencing at least some degree of peer victimization at either wave 1 or wave 2 (physical = 68.1%; relational = 89.8%; verbal = 87.9%; property-related = 65.8%; cyber = 63.1%). Furthermore, 16.1% of participants obtained raw scores on the RADS-2 greater than 75, and 8.1% obtained scores greater than 82 (signifying mild and moderate depression, respectively).
Table 1.
Pearson Correlations, Means, and Standard Deviations
| Variable | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | 21 | 22 | 23 | 24 | 25 | 26 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Age | 1.00 | |||||||||||||||||||||||||
| 2. Sex | .01 | 1.00 | ||||||||||||||||||||||||
| 3. W1 Verbal PV | .07* | −.03 | 1.00 | |||||||||||||||||||||||
| 4. W1 Physical PV | −.08* | .19*** | .59*** | 1.00 | ||||||||||||||||||||||
| 5. W1 Relational PV | −.04 | −.10** | .65*** | .53*** | 1.00 | |||||||||||||||||||||
| 6. W1 Property PV | −.06 | .06 | .43*** | .56*** | .59*** | 1.00 | ||||||||||||||||||||
| 7. W1 Cyber PV | .02 | −.03 | .25*** | .24*** | .38*** | .46*** | 1.00 | |||||||||||||||||||
| 8. W1 BYB | −.10** | −.17*** | .29*** | .25*** | .26*** | .20*** | .11** | 1.00 | ||||||||||||||||||
| 9. W1 RADS-2 | .02 | −.14*** | .37*** | .36*** | .41*** | .35*** | .16*** | .46*** | 1.00 | |||||||||||||||||
| 10. W1 CATS Total | −.01 | −.03 | .44*** | .42*** | .46*** | .43*** | .23*** | .50*** | .73*** | 1.00 | ||||||||||||||||
| 11. W1 CATS Phys threat | −.03 | −.03 | .36*** | .36*** | .40*** | .40*** | .25*** | .43*** | .68*** | .90*** | 1.00 | |||||||||||||||
| 12. W1 CATS Soc threat | −.04 | −.09** | .46*** | .38*** | .44*** | .37*** | .15*** | .56*** | .72*** | .91*** | .78*** | 1.00 | ||||||||||||||
| 13. W1 CATS Pers failure | −.02 | −.02 | .37*** | .38*** | .40*** | .40*** | .18*** | .52*** | .72*** | .92*** | .81*** | .84*** | 1.00 | |||||||||||||
| 14. W1 CATS Hostility | .06 | .06 | .32*** | .34*** | .37*** | .33*** | .24*** | .23*** | .44*** | .76*** | .56*** | .54*** | .55*** | 1.00 | ||||||||||||
| 15. W2 Verbal PV | .08* | .04 | .51*** | .35*** | .33*** | .21*** | .05 | .15*** | .28*** | .30*** | .27*** | .29*** | .26*** | .24*** | 1.00 | |||||||||||
| 16. W2 Physical PV | −.05 | .28*** | .34*** | .52*** | .32*** | .31*** | .19*** | .05 | .28*** | .32*** | .28*** | .31*** | .28*** | .25*** | .55*** | 1.00 | ||||||||||
| 17. W2 Relational PV | .03 | −.09** | .44*** | .34*** | .53*** | .29*** | .20*** | .19*** | .33*** | .31*** | .22*** | .28*** | .26*** | .30*** | .67*** | .46*** | 1.00 | |||||||||
| 18. W2 Property PV | −.03 | .11** | .28*** | .41*** | .36*** | .33*** | .40*** | .07* | .21*** | .27*** | .24*** | .19*** | .24*** | .26*** | .47*** | .56*** | .56*** | 1.00 | ||||||||
| 19. W2 Cyber PV | .07* | −.11** | .15*** | .07* | .16*** | .16*** | .31*** | .06 | .16*** | .17*** | .20*** | .11** | .12*** | .19*** | .30*** | .26*** | .45*** | .44*** | 1.00 | |||||||
| 20. W2 BYB | −.05 | −.22*** | .16*** | .07* | .09** | .00 | .13*** | .54*** | .37*** | .31*** | .28*** | .37*** | .27*** | .15*** | .29*** | .20*** | .30*** | .25*** | .18*** | 1.00 | ||||||
| 21. W2 RADS-2 | .11** | −.19*** | .20*** | .23*** | .16*** | .19*** | .11** | .31*** | .58*** | .40*** | .34*** | .42*** | .36*** | .25*** | .38*** | .36*** | .44*** | .36*** | .35*** | .50*** | 1.00 | |||||
| 22. W2 CATS Total | .08* | −.12*** | .25*** | .25*** | .16*** | .16*** | .21*** | .35*** | .47*** | .46*** | .41*** | .45*** | .34*** | .38*** | .42*** | .41*** | .49*** | .38*** | .34*** | .51*** | .74*** | 1.00 | ||||
| 23. W2 CATS Phys threat | .06 | −.13*** | .16*** | .21*** | .12*** | .17*** | .24*** | .35*** | .41*** | .34*** | .42*** | .36*** | .31*** | .23*** | .31*** | .35*** | .37*** | .37*** | .31*** | .43*** | .67*** | .88*** | 1.00 | |||
| 24. W2 CATS Soc threat | .07* | −.13*** | .21*** | .25*** | .16*** | .13*** | .15*** | .38*** | .47*** | .44*** | .36*** | .52*** | .36*** | .30*** | .48*** | .44*** | .51*** | .37*** | .33*** | .57*** | .71*** | .90*** | .72*** | 1.00 | ||
| 25. W2 CATS Pers failure | .02 | −.14*** | .18*** | .17*** | .09** | .12*** | .15*** | .38*** | .46*** | .39*** | .38*** | .44*** | .31*** | .22*** | .31*** | .35*** | .35*** | .28*** | .27*** | .55*** | .73*** | .90*** | .79*** | .82*** | 1.00 | |
| 26. W2 CATS Hostility | .11** | −.02 | .19*** | .22*** | .16*** | .14*** | .20*** | .11** | .28*** | .35*** | .28*** | .24*** | .20*** | .52*** | .34*** | .27*** | .44*** | .31*** | .27*** | .22*** | .43*** | .76*** | .55*** | .53*** | .48*** | 1.00 |
| M | 10.90 | 0.44 | 6.71 | 3.63 | 6.86 | 2.93 | 1.84 | 2.33 | 53.57 | 28.39 | 5.58 | 6.92 | 5.61 | 10.28 | 6.77 | 3.06 | 7.44 | 2.62 | 2.10 | 2.17 | 54.41 | 27.27 | 4.82 | 6.61 | 5.01 | 10.83 |
| SD | 1.18 | 0.50 | 5.43 | 4.47 | 5.69 | 4.12 | 3.55 | 1.05 | 15.12 | 28.56 | 7.43 | 8.76 | 8.39 | 8.18 | 5.60 | 3.88 | 5.69 | 3.52 | 3.58 | 1.01 | 16.93 | 26.11 | 6.42 | 8.12 | 7.66 | 8.29 |
Note. W1 = Wave 1; W2 = Wave 2; PV = peer victimization; BYB = Victimization-related negative self-cognitions, measured by the Behind Your Back measure; RADS-2= symptoms of depression, measured by the Reynolds Adolescent Depression Scale; CATS = generalized negative self-cognitions, measured by the Children’s Automatic Thoughts Scale.
p < .05.
p < .01,
p < .001.
Goal 1: Incremental Predictive Validity
Our first goal was to test whether CV longitudinally predicted negative self-cognitions and depressive symptoms over and above other forms of peer victimization while controlling for prior levels of the dependent variable. Accordingly, we conducted a series of hierarchical regressions, each with a different dependent variable from wave 2. In each regression, the step 1 predictor was the wave 1 measure of the outcome variable. In step 2, we entered all five wave 1 measures of victimization. We were interested in both the change in R-squared associated with all five victimization variables as well as the specific beta weight for wave 1 CV.
Table 2 contains the results of analyses in which the BYB, CATS (total score), or RADS-2 served as the outcome variable. In each analysis, the change in R-squared associated with the addition of the five victimization variables was significant (BYB: ΔF5, 820 = 7.75, p < .001; CATS: ΔF5, 820 = 4.63, p < .001, RADS-2: ΔF5, 820 = 2.23, p < .05), indicating that the five types of peer victimization collectively predicted each of the outcome variables, while controlling for a wave 1 measure of the outcome variable. Furthermore, the beta weight for the CV measure reached two-tailed significance (ps < .01) for the BYB and the CATS and one-tailed significance (p < .05) for the RADS-2, supporting the incremental predictive validity of CV over and above verbal, physical, relational, and property-related peer victimization.
Table 2.
Peer Victimization (PV) Subtypes Predicting Subsequent Negative Cognitions and Symptoms of Depression
| Step | Predictor | B | SE(B) | β | ΔR2 |
|---|---|---|---|---|---|
| Outcome = Wave 2 Victimization-related negative self-cognitions (BYB) | |||||
| 1 | Wave 1 BYB | 0.52 | .05 | 0.54*** | 0.29*** |
| 2 | Wave 1 BYB | 0.53 | .06 | 0.55*** | .03*** |
| Wave 1 Verbal PV | .01 | .02 | .03 | ||
| Wave 1 Physical PV | −.01 | .02 | −.06 | ||
| Wave 1 Relational PV | .00 | .02 | .00 | ||
| Wave 1 Property PV | −.04 | .02 | −0.17 | ||
| Wave 1 Cyber PV | .06 | .02 | 0.20** | ||
|
| |||||
| Outcome = Wave 2 Generalized negative self-cognitions (CATS) | |||||
| 1 | Wave 1 CATS | 0.48 | .05 | 0.52*** | 0.27*** |
| 2 | Wave 1 CATS | 0.41 | .07 | 0.46*** | .02*** |
| Wave 1 Verbal PV | .02 | 0.45 | .00 | ||
| Wave 1 Physical PV | 0.85 | 0.52 | 0.15 | ||
| Wave 1 Relational PV | −0.28 | 0.44 | −.06 | ||
| Wave 1 Property PV | −0.74 | 0.58 | −0.12 | ||
| Wave 1 Cyber PV | 1.62 | 0.52 | 0.22** | ||
|
| |||||
| Outcome = Wave 2 Symptoms of depression (RADS-2) | |||||
| 1 | Wave 1 RADS-2 | 0.62 | .06 | 0.57*** | 0.33*** |
| 2 | Wave 1 RADS-2 | 0.63 | .07 | 0.58*** | .01* |
| Wave 1 Verbal PV | −0.15 | 0.29 | −.05 | ||
| Wave 1 Physical PV | 0.23 | 0.34 | .06 | ||
| Wave 1 Relational PV | −0.20 | 0.29 | −.07 | ||
| Wave 1 Property PV | −0.12 | 0.37 | −.03 | ||
| Wave 1 Cyber PV | 0.60 | 0.34 | 0.13+ | ||
Note. BYB = Behind Your Back measure; CATS = Children’s Automatic Thoughts Scale; RADS-2= Reynolds Adolescent Depression Scale.
p < .10
p < .05
p < .01
p < .001.
As the CATS consists of various subscales, we followed up the significant prediction of its total score with a set of four additional hierarchical regressions, one for each subscale (physical threat, social threat, personal failure, and hostility). As shown in Table 3, the change in R-squared associated with the simultaneous addition of the five victimization variables was significant in the prediction of each CATS subscale (physical threat: ΔF5, 820 = 9.45, p < .001; social threat: ΔF5, 820 = 2.81, p < .05; personal failure: ΔF5, 820 = 3.10, p < .01; hostility: ΔF5, 820 = 4.76, p < .001). In the prediction of the physical threat subscale, the beta weights for both CV (p < .01) and physical victimization (p < .05) were significant, controlling for all else in the model. In the prediction of social threat, wave 1 CV was the only significant predictor (p < .01). In the prediction of perceived personal failure, wave 1 CV was the only significant predictor (p < .05). In the prediction of hostility, CV was again the only significant predictor but only at the one-tailed level (in the expected direction).
Table 3.
Peer Victimization (PV) Subtypes Predicting Subsequent Negative Self-Cognition Subtypes
| Step | Predictor | B | SE(B) | β | ΔR2 |
|---|---|---|---|---|---|
| Outcome = Wave 2 CATS Physical threat | |||||
| 1 | Wave 1 CATS Physical threat | 0.42 | .05 | 0.48*** | 0.23*** |
| 2 | Wave 1 CATS Physical threat | 0.35 | .06 | 0.41*** | .04*** |
| Wave 1 Verbal PV | −0.11 | 0.11 | −.09 | ||
| Wave 1 Physical PV | 0.28 | 0.13 | 0.20* | ||
| Wave 1 Relational PV | −.07 | 0.11 | −.06 | ||
| Wave 1 Property PV | −.09 | 0.15 | −.06 | ||
| Wave 1 Cyber PV | 0.42 | 0.13 | 0.23** | ||
|
| |||||
| Outcome = Wave 2 CATS Social threat | |||||
| 1 | Wave 1 CATS Social threat | 0.55 | .05 | 0.59*** | 0.35*** |
| 2 | Wave 1 CATS Social threat | 0.51 | .06 | 0.55*** | .01* |
| Wave 1 Verbal PV | 0.13 | 0.13 | .09 | ||
| Wave 1 Physical PV | 0.19 | 0.15 | 0.11 | ||
| Wave 1 Relational PV | −0.16 | 0.13 | −0.11 | ||
| Wave 1 Property PV | −0.29 | 0.17 | −0.15 | ||
| Wave 1 Cyber PV | 0.49 | 0.16 | 0.21** | ||
|
| |||||
| Outcome = Wave 2 CATS Personal failure | |||||
| 1 | Wave 1 CATS Personal failure | 0.34 | .06 | 0.37*** | 0.14*** |
| 2 | Wave 1 CATS Personal failure | 0.30 | .07 | 0.33*** | .02** |
| Wave 1 Verbal PV | .08 | 0.14 | .06 | ||
| Wave 1 Physical PV | 0.12 | 0.17 | .07 | ||
| Wave 1 Relational PV | −.08 | 0.14 | −.06 | ||
| Wave 1 Property PV | −0.22 | 0.19 | −0.12 | ||
| Wave 1 Cyber PV | 0.43 | 0.17 | 0.20* | ||
|
| |||||
| Outcome = Wave 2 CATS Hostility | |||||
| 1 | Wave 1 CATS Hostility | 0.51 | .06 | 0.51*** | 0.26*** |
| 2 | Wave 1 CATS Hostility | 0.47 | .07 | 0.47*** | .02*** |
| Wave 1 Verbal PV | −.09 | 0.14 | −.06 | ||
| Wave 1 Physical PV | 0.22 | 0.17 | 0.12 | ||
| Wave 1 Relational PV | .04 | 0.14 | .03 | ||
| Wave 1 Property PV | −0.15 | 0.18 | −.08 | ||
| Wave 1 Cyber PV | 0.30 | 0.17 | 0.13a | ||
Note. CATS = Children’s Automatic Thoughts Scale.
p < .05.
p < .01.
p < .001.
significant one-tailed test in expected direction (p < .05)
Goal 2: Stability
A second goal was to estimate and compare the 12-month stabilities of peer victimization subtypes. Pearson correlations of each wave 1 measure with its wave 2 counterpart are presented in Table 4. Using the Pearson-Filon z-test of dependent correlations, we compared all pairs of stability correlations. Stability coefficients for CV and property-related peer victimization were significantly smaller than were the stabilities of the other three (ps < .001). Differences among all other correlations were not significant.
Table 4.
One-year Stability Coefficients for Peer Victimization Subtypes and Pearson-Filon z-tests of their Differences
| Peer victimization subtype |
Pearson correlation |
Z-tests of Difference between Two Dependent Correlations |
|||
|---|---|---|---|---|---|
| Verbal | Physical | Relational | Property | ||
| Verbal | 0.51*** | -- | -- | -- | -- |
| Physical | 0.54*** | −1.00 | -- | -- | -- |
| Relational | 0.54*** | −1.09 | .00 | -- | -- |
| Property | 0.34*** | 4.68*** | 5.91*** | 6.02*** | -- |
| Cyber | 0.29* | 5.59*** | 6.38*** | 6.80*** | 1.24 |
p < .05.
p < .001.
We also compared mean-level stabilities for the five types of peer victimization. Using a multivariate approach to repeated measures ANOVA, we found a significant Type main effect, F(4,381) = 51.95, Wilks lambda = .40, p < .001, and a significant Type × Time interaction, F(4,381) = 2.87, Wilks lambda = .92, p < .05. As shown in Figure 1, the interaction reflects the fact that physical and property-related peer victimization diminish over time, while relational and cyber peer victimization increase. (Changes in verbal peer victimization were not significant.)
Figure 1.
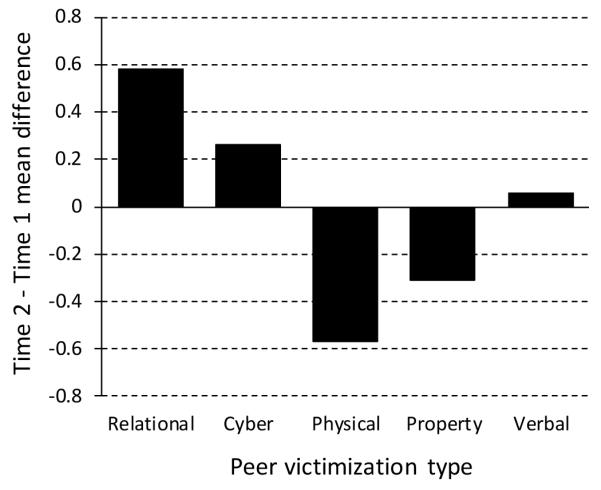
Time 2 – Time 1 mean differences for peer victimization subtypes.
Goal 3: Age and Gender
Our third goal was to examine not just the effects of Age and Gender on peer victimization but to test Age and Gender as potential moderators of the relation between CV and our outcome variables. Consequently, our first analysis tested the main effects of Age and Gender and their interaction on each peer victimization subtype. None of the interactions were significant. For physical peer victimization, main effects for Age (β = −.08, t = −1.96, p < .05) and Gender (β = 0.20, t = 4.80, p < .001) were significant, with exposure to physical peer victimization being greater at younger ages and for boys. For verbal peer victimization, the main effect for Age was significant (β = 0.11, t = 2.60, p < .01), with scores becoming larger with age. For relational peer victimization, the Gender main effect was significant (β = −0.11, t = −2.60, p < .01), with girls experiencing more than boys.
To test Age and Gender as moderators of the relation of CV to depression-related outcome, we conducted a series of multiple regressions, one for each wave 2 dependent variable (BYB, CATS, or RADS-2), controlling for wave 1 versions of the same outcome measure. We first examined the three-way interaction (Age × Gender × Cybervictimization). In none of the analyses was this three-way interaction significant. Then, removing the three-way interaction, we tested all two-way interactions. The Age × Gender interaction was significant only for the RADS-2: t = 2.06, p < .05. The finding was consistent with previous research, showing that age-related increases in depression scores were greater for girls than for boys. All other two-way interactions were nonsignificant.
Discussion
In this 12-month longitudinal study of 8- to 13-year-olds, three major sets of findings emerged. First, being subjected to CV was related to the development of negative self-cognitions and depressive symptoms over time, even after controlling for prior levels of the outcome measure and four other types of victimization. Second, despite its especially pernicious role, CV was among the least stable forms of victimization. Third, neither gender nor age was related to CV or moderated its relation to cognitive/emotional outcomes; however, gender and age differences did emerge for other forms of victimization. Below, we discuss how each of these findings extends the growing literature about the seriousness of CV and its potentially unique effect on young adolescents’ social-emotional development.
Several aspects of the first result deserve elaboration. First, CV demonstrated incremental predictive validity over and above more conventional forms of verbal, relational, physical, and property-related peer victimization. This result bolsters the conclusions of the only two other studies that examined the incremental, longitudinal effects of CV over other forms of peer victimization. One was Machmutow et al.’s (2012) six-month longitudinal study showing that time 2 but not time 1 CV predicted time 2 depressive symptoms while controlling for other forms of peer victimization. Interpretation of their results was complicated by the use of prior victimization and coping strategies as covariates. The other study was Landoll’s (2012) unpublished dissertation that also used a novel measure to show that CV predicted depressive symptoms six weeks later after controlling for relational, reputational, and overt victimization as well as prior levels of depressive symptoms (although some details about this analysis were not reported). The current study reinforces and extends the results of these studies in five ways: (1) it used an established measure of CV that was parallel in form to measures of other forms of victimization; (2) it controlled for relational, verbal, physical, and property-related types of noncyber victimization; (3) it intentionally did not control for coping strategies or other variables that could mediate the relation between victimization and outcome variables; (4) it extended the time frame to 12 months; and (5) it focused on the prediction of not just depressive symptoms but the emergence of cognitive diatheses for depression as well. Combining our results with the two previous longitudinal studies suggest that the incremental and predictive effects of CV on depression-related symptoms and cognitions are evident at six weeks, six months, and one year.
Speculation as to why CV shows incremental predictive validity over other forms of victimization suggests important directions for future research. Technically, its unique contribution is partially a result of its low correlation with other forms of peer victimization. Several factors may be responsible for this low correlation. One is that different kinds of personal behaviors and characteristics are evident in the online versus in-person worlds. Considerable research has shown that almost any characteristic that makes a person “different” is correlated with increased risk for victimization (Monks, Ortega-Ruiz, & Rodríguez-Hidalgo, 2008; Shea & Wiener, 2003; Visconti et al., 2013). What makes a person “different” in person may not be evident to potential online perpetrators. For example, physical differences or behavioral mannerisms that correlate with in-person peer victimization may not be relevant online. Future research should examine differential reasons for online versus in-person peer victimization. A second possibility is that the perpetrators of cyber bullying may constitute a qualitatively different social niche from one’s in-person bullies. If this is true, then research should be able to show that online interactions will differ more radically from in-person interactions when young people use social media to connect with people who are not part of their in-person social network. A third possibility is that one’s peers may simply act differently online than they do in-person. Research into this possibility might focus on theories about differences between public and private social interactions (e.g., Asch, 1956; Cialdini & Goldstein, 2004). Perceptions of social norms and one’s sense of audience may be very different for online versus in-person behavior. Fourth, cyber bullying may have more severe or longer lasting consequences compared to in-person victimization. Victims’ knowledge that CV can be highly viral, far-reaching, and virtually indefensible may contribute to the potency of CV in the prediction of depressive thoughts and symptoms. Each of these potential mediators deserves further research.
In the current study, CV not only predicted victimization-related negative thinking, it also predicted highly generalized negative self-cognitions and even depressive symptoms. In typically developing youths, resilience is essentially normative (Masten, 2007; Masten et al., 1990). The question arises, why is CV so detrimental? Part of the answer may be that (compared to other forms of peer victimization), victimizing texts, posts, or pictures on the Internet are instantly ubiquitous and virtually inescapable. Whereas most bullying is limited to particular times, people, and places, cyber bullying is perpetrated upon its victims any time and any place that a person can be online. Its pervasive nature may contribute to the over-generalized negative self-cognitions and the emergence of depressive symptoms. This possibility reflects aspects of Cole’s competency-based model of child depression (Cole, 1991). Children are highly motivated to construct for themselves a sense of self-perceived competence. Given the opportunity, they will selectively attend to positive feedback about themselves and attempt to denigrate or dismiss negative feedback (Harter, 1999). When negative feedback is pervasive, however, youths may become cognitively cornered into making negative conclusions about themselves. In light of the current findings, we speculate that CV may constitute exactly this kind of pervasive negative feedback.
The second set of findings pertained to the low temporal stability of individual differences in CV. Whereas verbal, relational, and physical peer victimization had 12-month stability correlations between .51 and .54, cybervictimizaton was significantly less stable (r = .29). Mean-level differences were also significant; cyber and relational peer victimization increased over time, while physical and property peer victimization decreased. Although the current study does not speak to the reasons for these differences, we speculate that two separate processes may be at work. On the one hand, physical and property-related peer victimization likely diminish as youths become increasingly socialized to social (if not legal) norms of behavior. On the other hand, adolescence is also a time of rapid skill development. The capacity for more subtle and technical forms of relational and cyber peer victimization increases. With age, more youths acquire smartphones, gain access to computers, and begin to use social media websites. These processes increase the total number of potential perpetrators and victims of cyber bullying. The tendency of socialization to reduce bullying may compete with the increasing number of potential cyber bullies and victims. The net result could be mean-level increases in CV coupled with low cross-time correlational stability. Future research could test this hypothesis by teasing apart these two developmental trends.
Third, although age and gender differences were evident for physical, social, and relational victimization, neither age nor gender differences emerged for CV. Furthermore, neither age nor gender moderated the longitudinal effects of CV on any of our outcome variables. On the one hand, this may reflect the generalizability of CV effects across age and gender. On the other hand, we should note that our oldest participants were only in grade 7 at the end of the study. As rates of social media use continue to increase with age, so might the incidence of CV and the seriousness of its effects. An important direction for future research will be to examine CV and its effects during later adolescence and even young adulthood.
Shortcomings of the current study suggest directions for future research. First, although the study was longitudinal and involved well-validated measures, all variables derived from self-report methods. Consequently, even though we statistically controlled for prior levels of the dependent variables, some shared method variance (e.g., social desirability, self-deception, other deception, etc.) could have affected our estimates of the relation between predictor and outcome measures. A powerful direction for future research would be to replicate the current findings using diverse methods of measurement. Second, the current study focused on youths between the ages of 8 and 13. Across this age range, we did not find that age significantly moderated the relations of CV to negative self-cognitions or depressive symptoms. Evidence of age as a moderator might well have emerged if our sample had spanned a wider age range. At younger ages, children’s online social networks may be nearly identical to their in-person social networks. In such cases, youths who are maltreated in person may also be maltreated online. As youths grow older, these two networks may overlap less and less. Consequently, how they are treated online may begin to differ from how they are treated face-to-face. If true, the incremental predictive validity of CV may increase with age. Third is effect size. On the one hand, the magnitudes of the CV effects were small to moderate in size. On the other hand, these effects are quite comparable to those reported for other kinds of victimization in other longitudinal studies in which prior level of the dependent variable have been statistically controlled (e.g., Boyes, Bowes, Cluver, Ward, & Badcock, 2014; Özdemir & Stattin, 2011; Perren & Alsaker, 2009; Prinstein, Cheah, & Guyer, 2005; Taylor, Sullivan, & Kliewer, 2013; Tran, Cole, & Weiss, 2012; Zwierzynska, Wolke, & Lereya, 2013). In longitudinal research, effects often vary as a function of time lag (Cole & Maxwell, 2009). Further research exploring the effects of CV over both shorter and longer lags is warranted. Fourth, participants in the current study constituted a nonclinical, school-based sample. An important direction for future research would be to extend this work to clinical samples with higher rates of diagnosable depressive disorders. Despite these shortcomings, this study provides important insights into the special toxicity of CV. As recognition of these harmful effects increases, school officials, parents, and researchers should pay particular attention to online bullying behaviors. Although these may be virtual acts of aggression, the consequences of these behaviors are far too real.
Acknowledgments
This research was supported by a gift from Patricia and Rodes Hart and by support from the Warren Family Foundation to David A. Cole. We thank Sara Alavi, Sydney Wait-Kudla, and Darcy Kayla for their support at various stages of this project.
Footnotes
None of the authors have conflicts of interest regarding any aspect of the research reported herein.
References
- Asch S. Studies of independence and conformity: I. A minority of one against a unanimous majority. Psychological Monographs: General and Applied. 1956;70:1–70. http://doi.org/10.1037/h0093718. [Google Scholar]
- Bauman S, Toomey RB, Walker JL. Associations among bullying, cyber-bullying, and suicide in high school students. Journal of Adolescence. 2013;36:341–350. doi: 10.1016/j.adolescence.2012.12.001. http://doi.org/10.1016/j.adolescence.2012.12.001. [DOI] [PubMed] [Google Scholar]
- Beck AT. Depression: Clinical, experimental, and theoretical aspects. Harper & Row; New York: 1967. [Google Scholar]
- Beck AT, Rush AJ, Shaw BF, Emery G. Cognitive therapy of depression. Guilford Press; New York: 1979. [Google Scholar]
- Bell MA, Wolfe CD. Emotion and cognition: An intricately bound developmental process. Child Development. 2004;75:366–370. doi: 10.1111/j.1467-8624.2004.00679.x. http://doi.org/10.1111/j.1467-8624.2004.00679.x. [DOI] [PubMed] [Google Scholar]
- Bonanno RA, Hymel S. Cyber bullying and internalizing difficulties: Above and beyond the impact of traditional forms of bullying. Journal of Youth and Adolescence. 2013;42:685–697. doi: 10.1007/s10964-013-9937-1. http://doi.org/10.1007/s10964-013-9937-1. [DOI] [PubMed] [Google Scholar]
- Boyes ME, Bowes L, Cluver LD, Ward CL, Badcock NA. Bullying victimisation, internalising symptoms, and conduct problems in South African children and adolescents: A longitudinal investigation. Journal of Abnormal Child Psychology. 2014;42(8):1313–1324. doi: 10.1007/s10802-014-9888-3. doi: http://dx.doi.org/10.1007/s10802-014-9888-3. [DOI] [PubMed] [Google Scholar]
- Campbell M, Spears B, Slee P, Butler D, Kift S. Victims’ perceptions of traditional and cyber bullying, and the psychosocial correlates of their victimisation. Emotional and Behavioural Difficulties. 2012;17:389–401. http://doi.org/10.1080/13632752.2012.704316. [Google Scholar]
- Cappadocia MC, Craig WM, Pepler D. Cyber bullying: Prevalence, stability, and risk factors during adolescence. Canadian Journal of School Psychology. 2013;28:171–192. http://doi.org/10.1177/0829573513491212. [Google Scholar]
- Cialdini RB, Goldstein NJ. Social influence: Compliance and conformity. Annual Review of Psychology. 2004;55:591–621. doi: 10.1146/annurev.psych.55.090902.142015. http://doi.org/10.1146/annurev.psych.55.090902.142015. [DOI] [PubMed] [Google Scholar]
- Cole DA, Maxwell SE. Statistical methods for risk-outcome research: Being sensitive to longitudinal structure. Annual Review of Clinical Psychology. 2009;5:71–96. doi: 10.1146/annurev-clinpsy-060508-130357. http://dx.doi.org/10.1146/annurev-clinpsy-060508-130357. [DOI] [PubMed] [Google Scholar]
- Cole DA. Preliminary support for a competency-based model of depression in children. Journal of Abnormal Psychology. 1991;100:181–190. doi: 10.1037//0021-843x.100.2.181. http://doi.org/10.1037/0021-843X.100.2.181. [DOI] [PubMed] [Google Scholar]
- Cole DA, Dukewich T, Roeder K, Sinclair KR, McMillan J, Will E, Felton J. Linking peer victimization to the development of depressive self-schemas in children and adolescents. Journal of Abnormal Child Psychology. 2014;42:149–160. doi: 10.1007/s10802-013-9769-1. http://doi.org/10.1007/s10802-013-9769-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cole DA, Sinclair KR, Zelkowitz R, Bilsky SA, Roeder K, Spinelli T. Peer victimization and harsh parenting predict cognitive diatheses for depression in children and adolescents. Journal of Clinical Child & Adolescent Psychology. doi: 10.1080/15374416.2015.1004679. (In press) http://doi.org/10.1080/15374416.2015.1004679. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cole PM, Martin SE, Dennis TA. Emotion regulation as a scientific construct: methodological challenges and directions for child development research. Child Development. 2004;75:317–333. doi: 10.1111/j.1467-8624.2004.00673.x. http://doi.org/10.1111/j.1467-8624.2004.00673.x. [DOI] [PubMed] [Google Scholar]
- Dempsey AG, Sulkowski ML, Nichols R, Storch EA. Differences between peer victimization in cyber and physical settings and associated psychosocial adjustment in early adolescence. Psychology in the Schools. 2009;46:962–972. http://doi.org/10.1002/pits.20437. [Google Scholar]
- Dooley JJ, Shaw T, Cross D. The association between the mental health and behavioural problems of students and their reactions to cyber-victimization. European Journal of Developmental Psychology. 2012;9:275–289. doi: http://dx.doi.org.proxy.library.vanderbilt.edu/10.1080/17405629.2011.648425. [Google Scholar]
- Gan SS, Zhong C, Das S, Gan JS, Willis S, Tully E. The prevalence of bullying and cyber bullying in high school: A 2011 survey. International Journal of Adolescent Medicine and Health. 2014;26:27–31. doi: 10.1515/ijamh-2012-0106. http://doi.org/10.1515/ijamh-2012-0106. [DOI] [PubMed] [Google Scholar]
- Gámez-Guadix M, Orue I, Smith PK, Calvete E. Longitudinal and reciprocal relations of cyber bullying with depression, substance use, and problematic Internet use among adolescents. Journal of Adolescent Health. 2013;53:446–452. doi: 10.1016/j.jadohealth.2013.03.030. http://doi.org/10.1016/j.jadohealth.2013.03.030. [DOI] [PubMed] [Google Scholar]
- Gibb BE, Alloy LB, Walshaw PD, Comer JS, Shen GHC, Villari AG. Predictors of attributional style change in children. Journal of Abnormal Child Psychology. 2006;34:408–422. doi: 10.1007/s10802-006-9022-2. http://doi.org/10.1007/s10802-006-9022-2. [DOI] [PubMed] [Google Scholar]
- Gillham JE, Reivich KJ, Brunwasser SM, Freres DR, Chajon ND, Kash-MacDonald VM, Seligman MEP. Evaluation of a group cognitive-behavioral depression prevention program for young adolescents: A randomized effectiveness trial. Journal of Clinical Child & Adolescent Psychology. 2012;41:621–639. doi: 10.1080/15374416.2012.706517. http://doi.org/10.1080/15374416.2012.706517. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harter S. A model of causes, correlates, and consequences of global self-worth. In: Harter S, editor. The construction of the self: A developmental perspective. New York; Guilford: 1999. [Google Scholar]
- Hawker DSJ, Boulton MJ. Twenty years’ research on peer victimization and psychosocial maladjustment: A meta-analytic review of cross-sectional studies. Journal of Child Psychology and Psychiatry. 2000;41:441–455. http://doi.org/10.1111/1469-761.00629. [PubMed] [Google Scholar]
- Ingram RE. Self-focused attention in clinical disorders: Review and a conceptual model. Psychological Bulletin. 1990;107:156–176. doi: 10.1037/0033-2909.107.2.156. http://doi.org/10.1037/0033-2909.107.2.156. [DOI] [PubMed] [Google Scholar]
- Jackson CL, Cohen R. Childhood victimization: Modeling the relation between classroom victimization, cyber victimization, and psychosocial functioning. Psychology of Popular Media Culture. 2012;1:254–269. http://doi.org/10.1037/a0029482. [Google Scholar]
- Kessel Schneider S, O’Donnell L, Stueve A, Coulter RWS. Cyber bullying, school bullying, and psychological distress: A regional census of high school students. American Journal of Public Health. 2012;102:171–177. doi: 10.2105/AJPH.2011.300308. http://doi.org/10.2105/AJPH.2011.300308. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kowalski RM, Limber SP. Psychological, physical, and academic correlates of cyber bullying and traditional bullying. Journal of Adolescent Health. 2013;53(1, Suppl):S13–S20. doi: 10.1016/j.jadohealth.2012.09.018. http://doi.org/10.1016/j.jadohealth.2012.09.018. [DOI] [PubMed] [Google Scholar]
- Landoll RR. The new frontier of peer victimization: Prospective associations between adolescents’ on-line peer victimization and internalizing symptoms. 2012 Retrieved from http://scholarlyrepository.miami.edu/oa_dissertations/820/
- Landoll RR, La Greca AM, Landoll RR, Swedo DE. Who Am I in a Digital World? Associations between Youths’ On-line Behavior and Offline Development. Society for Research on Adolescence; Philadelphia, PA: Mar, 2010. New ways to hurt: The development and utility of a measure of cyber-victimization among adolescents and emerging adults. [Google Scholar]
- Laurent J, Joiner TE, Catanzaro SJ. Positive affect, negative affect, and physiological hyperarousal among referred and nonreferred youths. Psychological Assessment. 2011;23:945–957. doi: 10.1037/a0024080. http://doi.org/10.1037/a0024080. [DOI] [PubMed] [Google Scholar]
- Leung AN, McBride-Chang C. Game on? Online friendship, cyber bullying, and psychosocial adjustment in Hong Kong Chinese children. Journal of Social and Clinical Psychology. 2013;32:159–185. http://doi.org/10.1521/jscp.2013.32.2.159. [Google Scholar]
- Machmutow K, Perren S, Sticca F, Alsaker FD. Peer victimisation and depressive symptoms: Can specific coping strategies buffer the negative impact of cybervictimisation? Emotional & Behavioural Difficulties. 2012;17:403–420. doi: http://dx.doi.org.proxy.library.vanderbilt.edu/10.1080/13632752.2012.704310. [Google Scholar]
- Masten AS. Resilience in developing systems: Progress and promise as the fourth wave rises. Development and Psychopathology. 2007;19:921–930. doi: 10.1017/S0954579407000442. http://doi.org/10.1017/S0954579407000442. [DOI] [PubMed] [Google Scholar]
- Masten AS, Best KM, Garmezy N. Resilience and development: Contributions from the study of children who overcome adversity. Development and Psychopathology. 1990;2:425–444. http://doi.org/10.1017/S0954579400005812. [Google Scholar]
- Micco JA, Ehrenreich JT. Validity and specificity of the Children’s Automatic Thoughts Scale in clinically anxious and non-clinical children. Cognitive Therapy and Research. 2009;33:532–536. http://doi.org/10.1007/s10608-009-9230-5. [Google Scholar]
- Mogg K, Bradley BP. Attentional bias in generalized anxiety disorder versus depressive disorder. Cognitive Therapy and Research. 2005;29:29–45. http://doi.org/10.1007/s10608-005-1646-y. [Google Scholar]
- Monks CP, Ortega-Ruiz R, Rodríguez-Hidalgo AJ. Peer victimization in multicultural schools in Spain and England. European Journal of Developmental Psychology. 2008;5:507–535. doi: http://dx.doi.org/10.1080/17405620701307316. [Google Scholar]
- Nansel TR, Overpeck M, Pilla RS, Ruan WJ, Simons-Morton B, Scheidt P. Bullying behaviors among US youth: Prevalence and association with psychosocial adjustment. JAMA: Journal of the American Medical Association. 2001;285:2094–2100. doi: 10.1001/jama.285.16.2094. doi: http://dx.doi.org/10.1001/jama.285.16.2094. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nordahl J, Beran TN, Dittrick CJ. Psychological impact of cyber-bullying: Implications for school counsellors. Canadian Journal of Counselling and Psychotherapy/Revue Canadienne de Counseling et de Psychothérapie. 2013;47:383–402. [Google Scholar]
- Olenik-Shemesh D, Heiman T, Eden S. Cyber bullying victimisation in adolescence: Relationships with loneliness and depressive mood. Emotional and Behavioural Difficulties. 2012;17:361–374. http://doi.org/10.1080/13632752.2012.704227. [Google Scholar]
- Özdemir M, Stattin H. Bullies, victims, and bully-victims: A longitudinal examination of the effects of bullying-victimization experiences on youth well-being. Journal of Aggression, Conflict and Peace Research. 2011;3:97–102. http://dx.doi.org/10.1108/17596591111132918. [Google Scholar]
- Painter K. Outcomes for youth with severe emotional disturbance: A repeated measures longitudinal study of a wraparound approach of service delivery in systems of care. Child Youth Care Forum. 2012;41:407–425. http://doi.org/10.1007/s10566-011-9167-11. [Google Scholar]
- Perren S, Alsaker FD. Depressive symptoms from kindergarten to early school age: Longitudinal associations with social skills deficits and peer victimization. Child and Adolescent Psychiatry and Mental Health. 2009;3:1–10. doi: 10.1186/1753-2000-3-28. http://dx.doi.org/10.1186/1753-2000-3-28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Perren S, Dooley J, Shaw T, Cross D. Bullying in school and cyberspace: Associations with depressive symptoms in Swiss and Australian adolescents. Child and Adolescent Psychiatry and Mental Health. 2010;4 doi: 10.1186/1753-2000-4-28. http://doi.org/10.1186/1753-2000-4-28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pew Research Center Pew Research Internet Project. 2014 Retrieved from http://www.pewinternet.org/2013/05/21/part-1-teens-and-social-media-use/
- Price M, Chin MA, Higa-McMillan C, Kim S, Frueh CB. Prevalence and internalizing problems of ethnoracially diverse victims of traditional and cyber bullying. School Mental Health. 2013;5:183–191. doi: http://dx.doi.org.proxy.library.vanderbilt.edu/10.1007/s12310-013-9104-6. [Google Scholar]
- Prinstein MJ, Cheah CSL, Guyer AE. Peer victimization, cue interpretation, and internalizing symptoms: Preliminary concurrent and longitudinal findings for children and adolescents. Journal of Clinical Child and Adolescent Psychology. 2005;34:11–24. doi: 10.1207/s15374424jccp3401_2. http://dx.doi.org/10.1207/s15374424jccp3401_2. [DOI] [PubMed] [Google Scholar]
- Reynolds WM, Mazza JJ. A longitudinal investigation of depression, hopelessness, social support, and major and minor life events and their relation to suicidal ideation in adolescents. Suicide and Life-Threatening Behavior. 1998;28:358–374. [PubMed] [Google Scholar]
- Reynolds WM. Reynolds Adolescent Depression Scale: Professional manual. 2nd ed Psychological Assessment Resources, Inc; Odessa, FL: 2002. [Google Scholar]
- Salmivalli C, Sainio M, Hodges EVE. Electronic Victimization: Correlates, Antecedents, and Consequences Among Elementary and Middle School Students. Journal of Clinical Child & Adolescent Psychology. 2013;42:442–453. doi: 10.1080/15374416.2012.759228. http://doi.org/10.1080/15374416.2012.759228. [DOI] [PubMed] [Google Scholar]
- Scher CD, Ingram RE, Segal ZV. Cognitive reactivity and vulnerability: Empirical evaluation of construct activation and cognitive diatheses in unipolar depression. Clinical Psychology Review. 2005;25:487–510. doi: 10.1016/j.cpr.2005.01.005. http://doi.org/10.1016/j.cpr.2005.01.005. [DOI] [PubMed] [Google Scholar]
- Schniering CA, Rapee RM. Development and validation of a measure of children’s automatic thoughts: The Children’s Automatic Thoughts Scale. Behaviour Research and Therapy. 2002;40:1091–1109. doi: 10.1016/s0005-7967(02)00022-0. http://doi.org/10.1016/S0005-7967(02)00022-0. [DOI] [PubMed] [Google Scholar]
- Schniering CA, Lyneham H. The Children’s Automatic Thoughts Scale in a clinical sample: Psychometric properties and clinical utility. Behaviour Research and Therapy. 2007;45:1931–1940. doi: 10.1016/j.brat.2006.09.009. http://doi.org/10.1016/j.brat.2006.09.009. [DOI] [PubMed] [Google Scholar]
- Schultze-Krumbholz A, Jäkel A, Schultze M, Scheithauer H. Emotional and behavioural problems in the context of cyber bullying: A longitudinal study among German adolescents. Emotional and Behavioural Difficulties. 2012;17:329–345. http://doi.org/10.1080/13632752.2012.704317. [Google Scholar]
- Segal ZV, Ingram RE. Mood priming and construct activation in tests of cognitive vulnerability to unipolar depression. Clinical Psychology Review. 1994;14:663–695. doi: 10.1016/j.cpr.2005.01.005. http://doi.org/10.1016/0272-7358(94)90003-5. [DOI] [PubMed] [Google Scholar]
- Shea B, Wiener J. Social exile: The cycle of peer victimization for boys with ADHD. Canadian Journal of School Psychology. 2003;18:55–90. http://dx.doi.org/10.1177/082957350301800104. [Google Scholar]
- Sinclair KR, Cole DA, Dukewich T, Felton J, Weitlauf AS, Maxwell MA, Jacky A. Impact of physical and relational peer victimization on depressive cognitions in children and adolescents. Journal of Clinical Child & Adolescent Psychology. 2012;41:570–583. doi: 10.1080/15374416.2012.704841. http://doi.org/10.1080/15374416.2012.704841. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith PK, Mahdavi J, Carvalho M, Fisher S, Russell S, Tippett N. Cyber bullying: Its nature and impact in secondary school pupils. Journal of Child Psychology and Psychiatry. 2008;49:376–385. doi: 10.1111/j.1469-7610.2007.01846.x. http://doi.org/10.1111/j.1469-7610.2007.01846.x. [DOI] [PubMed] [Google Scholar]
- Sontag LM, Clemans KH, Graber JA, Lyndon ST. Traditional and cyber aggressors and victims: A comparison of psychosocial characteristics. Journal of Youth and Adolescence. 2011;40:392–404. doi: 10.1007/s10964-010-9575-9. http://doi.org/10.1007/s10964-010-9575-9. [DOI] [PubMed] [Google Scholar]
- Taylor KA, Sullivan TN, Kliewer W. A longitudinal path analysis of peer victimization, threat appraisals to the self, and aggression, anxiety, and depression among urban African American adolescents. Journal of Youth and Adolescence. 2013;42:178–189. doi: 10.1007/s10964-012-9821-4. http://dx.doi.org/10.1007/s10964-012-9821-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tran CV, Cole DA, Weiss B. Testing reciprocal longitudinal relations between peer victimization and depressive symptoms in young adolescents. Journal of Clinical Child and Adolescent Psychology. 2012;41:353–360. doi: 10.1080/15374416.2012.662674. http://dx.doi.org/10.1080/15374416.2012.662674. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Turner MG, Exum ML, Brame R, Holt TJ. Bullying victimization and adolescent mental health: General and typological effects across sex. Journal of Criminal Justice. 2013;41(1):53–59. http://doi.org/10.1016/j.jcrimjus.2012.12.005. [Google Scholar]
- Visconti KJ, Kochenderfer-Ladd B, Clifford CA. Children’s attributions for peer victimization: A social comparison approach. Journal of Applied Developmental Psychology. 2013;34:277–287. http://dx.doi.org/10.1016/j.appdev.2013.06.002. [Google Scholar]
- VÖllink T, Bolman CAW, Dehue F, Jacobs NCL. Coping with cyberbullying: Differences between victims, bully-victims and children not involved in bullying. Journal of Community & Applied Social Psychology. 2013;23:7–24. doi: http://dx.doi.org.proxy.library.vanderbilt.edu/10.1002/casp.2142. [Google Scholar]
- Wang J, Ianotti RJ, Luk JW, Nansel TR. Co-occurrence of victimization from five subtypes of bullying: Physical, verbal, social exclusion, spreading rumors, and cyber. Journal of Pediatric Psychology. 2010;35:1103–1112. doi: 10.1093/jpepsy/jsq048. http://doi.org/10.1093/jpepsy/jsq048. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wang J, Nansel TR, Iannotti RJ. Cyber and traditional bullying: Differential association with depression. Journal of Adolescent Health. 2011;48:415–417. doi: 10.1016/j.jadohealth.2010.07.012. http://doi.org/10.1016/j.jadohealth.201.07.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Williford A, Elledge LC, Boulton AJ, DePaolis KJ, Little TD, Salmivalli C. Effects of the KiVa Antibullying Program on cyber bullying and cybervictimization frequency among Finnish youth. Journal of Clinical Child and Adolescent Psychology. 2013;42:820–833. doi: 10.1080/15374416.2013.787623. http://doi.org/10.1080/15374416.2013.787623. [DOI] [PubMed] [Google Scholar]
- Zwierzynska K, Wolke D, Lereya TS. Peer victimization in childhood and internalizing problems in adolescence: A prospective longitudinal study. Journal of Abnormal Child Psychology. 2013;41:309–323. doi: 10.1007/s10802-012-9678-8. http://dx.doi.org/10.1007/s10802-012-9678-8. [DOI] [PubMed] [Google Scholar]