

Abstract
Background/Aims:
The smoking rates and patterns in the North Korean population are not well known. More than 20,000 North Korean defectors have settled in South Korea; thus, we can estimate the current North Korean smoking situation using this group.
Methods:
All North Korean defectors spend their first 3 months in a South Korean facility learning to adapt to their new home. We retrospectively analyzed the results from a questionnaire conducted among North Korean male defectors in this facility from August 2012 to February 2014.
Results:
Of 272 men, 84.2% were current smokers, 12.5% were ex-smokers, and 3.3% were non-smokers. The mean age of this group was 35.9 ± 11.3 years, and smoking initiation occurred at a mean age of 18.2 ± 4.7 years. Among the subjects, 78.1% had a family member who smoked. Of the 221 current smokers, 67.4% responded that they intended to quit smoking. Fagerström test and Kano test for social nicotine dependence (KTSND) results for current smokers were 3.35 ± 2.26 and 13.76 ± 4.87, respectively. Question 9 on the KTSND (doctors exaggerate the ill effects of smoking) earned a significantly higher score relative to the other questions and a significantly higher score in current smokers compared with non-smokers.
Conclusions:
The smoking rate in North Korean male defectors was higher than that indicated previously. However, interest in smoking cessation was high and nicotine dependence was less severe than expected. Further investigation is needed to identify an efficient method for North Korean smokers to stop smoking.
Keywords: Smoking, North Korean defectors, Tobacco use disorder, Smoking cessation
INTRODUCTION
Smoking is a leading cause of morbidity and mortality worldwide [1-3]. Tobacco use has declined steadily in developed countries over the past 20 to 30 years with increasing awareness of smoking-associated risks and heightened anti-smoking campaigns [4,5]. The smoking rate of people in the USA > 15-year-old was 42.4% in 1965, which declined to 14.2% in 2012 [6]. Similarly, smoking cessation has become an important social issue in South Korea due to lung cancer [7]. The smoking rate in South Korea among those > 15-year-old has decreased substantially from 34.6% in 1989 to 21.6% in 2012, which is approximately the same rate as that in Japan [6]. However, inadequate public awareness and tobacco control programs have resulted in a sharp increase in tobacco smoking among men over the past few decades in other Asian countries, particularly low- and middle-income countries [8]. Similarly, the smoking rate in North Korea is predicted to be high, but the smoking rates and patterns in the North Korean population are mostly unknown due to a lack of statistical research. World Health Organization (WHO) report in 2008 indicated that the smoking rate in North Korean adult men was 59.5%, whereas that in South Korean adult men was 53.8% [9]. However, this rate reported in the former population was lower than our expectation. In addition, limited information is available about smoking behavior, amount of smoking, nicotine dependence, and socioeconomic status among North Koreans. More than 20,000 North Korean defectors have settled in South Korea; thus, we can estimate the current smoking situation in North Korea using this population. We evaluated the smoking pattern and nicotine dependence in North Korean male defectors. We also used Kano test for social nicotine dependence (KTSND) to identify psychological and psychosocial states associated with smoking, because of the unique aspects of the North Korean society.
METHODS
Subjects
All North Korean defectors spend their first 3 months in South Korea at Hanawon, a government-sponsored educational facility to learn to adapt to their new home. We retrospectively analyzed the results of a smoking-related questionnaire conducted in all North Korean male defectors > 19 years of age who were in this facility from August 2012 to February 2014. The questionnaire was conducted with informed consent when they entered the facility. The questionnaire was not designed originally for this study but was used to understand the health status, demand for medical care, and basic data on smoking cessation education in North Korean defectors. Approval was obtained from the Institutional Review Board of Yeouido St. Mary’s Hospital (SC15RISI0002).
Diagnostic tools
The self-administered questionnaire was distributed at the facility health education class and returned after 1 hours. The questionnaire queried gender, age, smoking history (current smoking status, amount of smoking, and age of smoking initiation), smoking cessation history (experience and will to quit smoking), the Fagerström test for nicotine dependence (FTND), and the KTSND. Non-smokers were defined as those who had smoked less than 100 cigarettes in their lifetime [10]. Ex-smokers were defined as those who had quit smoking more than 6 months before the survey [11]. Collecting further personal information was limited due to personal protection and security issues.
FTND
The FTND was developed to assess the degree of physical dependence on nicotine [12]. It contains six items that assess different aspects of smoking behavior. The total score ranges from 0 to 10, with a higher score indicating greater nicotine dependence. Studies have shown reasonable reliability and internal consistency of the FTND [13,14]. The FTND is a better predictor of smoking relapse among smokers attempting to quit than is the number of cigarettes per day statistic [15]. Park et al. [16] examined smokers in Korea using the FTND and reported that it is a valid and reliable measure for Koreans. We used the Korean translation of the FTND from their study. FTND was only measured in the current and exsmokers. Ex-smokers answered the questions based on their previous smoking habits.
KTSND
The KTSND is a 10-item questionnaire with a total maximum score of 30 and is used to quantify social nicotine dependence. The KTSND is a useful index to evaluate the psychological aspects of smoking [17] and to select a smoking cessation method and predict the outcome of smoking cessation treatment [18]. Some Japanese studies have reported high KTSND scores among non-smoking children and adolescents who live with family members who smoke or associate with smoking friends [19,20]. Jeong et al. [21] suggested that the Korean KTSND questionnaire could be a useful method to evaluate the psychosocial aspects of smoking in Koreans.
Statistical analysis
The FTND results between current smokers and ex-smokers were compared using the Student t test. The KTSND results among current smokers, ex-smokers, and non-smokers were compared by analysis of variance (ANOVA), and Bonferroni’s correction was applied to the post hoc analysis. The FTND and KTSND results between having a family member who smokes and the intention to quit smoking or previous attempts to quit were also compared using the Student t test. The KTNSD mean values were compared by ANOVA and Bonferroni’s correction. Correlation between the scales (FTND and KTSND) and continuous variables (smoking amount per day, smoking year, smoking start age, and current age) were assessed using Spearman’s correlation analysis. Statistical analyses were performed using the SPSS version 18.0 (SPSS Inc., Chicago, IL, USA). A p < 0.05 was considered significant.
RESULTS
We analyzed 272 North Korean male defectors and their mean age was 35.9 ± 11.3 years (Table 1). The mean age of smoking initiation was 18.2 ± 4.7 years and eight subjects started smoking at < 10 years of age. Of the 272 participants, 229 (84.2%) were current smokers, 34 (12.5%) were ex-smokers, and nine (3.3%) were non-smokers. In both current and ex-smokers, the mean smoking amount per day was 0.7 ± 0.4 packs, and the mean smoking duration was 17.0 ± 10.7 years. The mean total smoking amount was 12.3 ± 11.6 pack-year. A total of 203 subjects (78.1%) had family members who smoked. Approximately 67.4% of current smokers intended to quit smoking, and 70.6% of current and ex-smokers had attempted to quit smoking previously. The success rate of smoking cessation in subjects who had made a previous attempt was 18.9%.
Table 1.
Demographic characteristics of the North Korean male defectors (n = 272)
| Characteristic | Value |
|---|---|
| Age, yr | 35.9 ± 11.3 |
| Age of smoking initiation, yr | 18.2 ± 4.7 |
| Smoking history | |
| Current smokers | 229 (84.2) |
| Ex-smokers | 34 (12.5) |
| Non-smokers | 9 (3.3) |
| Smoking amount | |
| Packs per day | 0.7 ± 0.4 |
| Years of smoking | 17.0 ± 10.7 |
| Pack-years | 12.3 ± 11.6 |
| Family members who smoked | 203/260 (78.1) |
| Smoking cessation | |
| Intention to quit smoking in current smokers | 149/221 (67.4) |
| Previous attempt in current and ex-smokers | 180/255 (70.6) |
| Success rate | 34/180 (18.9) |
| FTND scorea | 3.26 ± 2.24 |
| KTSND scoreb | 13.32 ± 4.95 |
Values are presented as mean ± SD or number (%).
FTND, Fagerström test for nicotine dependence; KTSND, Kano test for social nicotine dependence.
FTND was measured in current and ex-smokers (n = 193).
KTSND was measured in current, ex- and non-smokers (n = 255).
The mean FTND score for physical nicotine dependence, measured only in current and ex-smokers (n = 193), was 3.26 ± 2.24. The FTND results were compared between current and ex-smokers (Table 2). The mean FTND scores of current and ex-smokers were 3.35 ± 2.26 and 2.57 ± 1.99, respectively. Current smokers tended to have a slightly higher FTND score than that of exsmokers.
Table 2.
Fagerström test between current smokers and ex-smokers
| Item | Current smokers (n = 172) | Ex-smokers (n = 21) | p valuea |
|---|---|---|---|
| Q1. How soon after you wake up do you smoke your first cigarette? | 1.46 ± 1.08 | 1.05 ± 1.12 | 0.103 |
| Q2. Do you find it difficult to refrain from smoking in places where it is forbidden, e.g., in a church, at a library, in cinema, etc.? | 0.27 ± 0.45 | 0.14 ± 0.36 | 0.138 |
| Q3. Which cigarette would you hate most to give up? | 0.54 ± 0.50 | 0.48 ± 0.51 | 0.578 |
| Q4. How many cigarettes/day do you smoke? | 0.49 ± 0.70 | 0.52 ± 0.81 | 0.829 |
| Q5. Do you smoke more frequently during the first hours after waking than during the rest of the day? | 0.15 ± 0.36 | 0.14 ± 0.36 | 0.920 |
| Q6. Do you smoke when you are so ill that you are in bed most of the day? | 0.44 ± 0.50 | 0.24 ± 0.44 | 0.064 |
| FTND score | 3.35 ± 2.26 | 2.57 ± 1.99 | 0.133 |
Values are presented as mean ± SD.
FTND, Fagerström test for nicotine dependence.
Comparison between current smokers and ex-smokers was done by t test.
The mean KTSND score, measured in current, ex-, and non-smokers (n = 255), was 13.32 ± 4.95. The KTSND results were compared among current, ex-, and non-smokers (Table 3). Mean total KTSND scores were 13.76 ± 4.87, 11.85 ± 4.74, and 8.33 ± 4.21 in current, ex-, and non-smokers, respectively. The total KTSND score and the specific scores for question (Q) 4 (smokers’ lifestyles may be respected), Q7 (tobacco has effects to relieve stress), and Q9 (doctors exaggerate the ill effects of smoking) were significantly different among the three groups (p = 0.001, p = 0.023, p < 0.001, and p = 0.037, respectively). Although no significant differences in scores were observed among the other questions, current smokers tended to have higher scores than those of ex- and non-smokers. Current smokers had a significantly higher total KTSND score compared with that of non-smokers after post hoc analysis and Bonferroni’s correction. Current smokers reported significantly higher Q7 values than those of ex- and non-smokers, as well as significantly higher Q9 values than those of non-smokers. A post hoc analysis of the Q4 results showed no difference. All KTSND responses were compared with each other in all subjects (Fig. 1). Significantly higher values were seen for Q7, Q9, and Q10 compared with the other questions, both in total subjects and in current smokers. The Q9 and Q10 values were also significantly higher than those for the other questions among ex-smokers. However, not all questions showed significant differences in non-smokers. The FTND and KTSND results were compared with other characteristics (Table 4). The mean FTND and KTSND results tended to be higher in subjects who had a family member who smoked; however, they were significantly lower in those who intended to quit smoking and who previously attempted to quit smoking. The mean FTND values were 2.94 ± 2.04 and 3.85 ± 2.41, and the mean KTSND values were 13.00 ± 4.53 and 14.72 ± 5.32 in the group that intended to quit and the group that did not, respectively. The mean FTND values in the group who previously attempted to quit smoking and in the group who did not were 3.05 ± 2.15 and 3.85 ± 2.38, respectively, and the mean KTSND values were 12.72 ± 4.68 and 15.16 ± 4.97, respectively.
Table 3.
Kano test for social nicotine dependence between current, ex-, and non-smokers
| Item | Current smokers (n = 213) | Ex-smokers (n = 33) | Non-smokers (n = 9) | p valuea |
|---|---|---|---|---|
| Q1. Smoking itself is a disease | 1.19 ± 1.07 | 1.18 ± 1.10 | 0.67 ± 0.71 | 0.353 |
| Q2. Smoking is a part of culture | 1.11 ± 0.97 | 0.85 ± 0.94 | 0.89 ± 0.78 | 0.289 |
| Q3. Tobacco is one of life’s pleasures | 1.48 ± 0.94 | 1.36 ± 1.14 | 1.11 ± 1.05 | 0.446 |
| Q4. Smokers’ lifestyles may be respected | 1.01 ± 0.94 | 0.64 ± 0.78 | 0.44 ± 0.73 | 0.023b |
| Q5. Smoking sometimes enriches people’s life | 0.89 ± 0.86 | 0.61 ± 0.83 | 0.44 ± 0.73 | 0.082 |
| Q6. Tobacco has positive physical or mental effects | 1.04 ± 1.20 | 0.85 ± 0.97 | 0.33 ± 0.71 | 0.149 |
| Q7. Tobacco has effects to relieve stress | 1.92 ± 0.79 | 1.48 ± 0.97 | 0.89 ± 1.05 | < 0.001c |
| Q8. Tobacco enhances the function of smokers’ brains | 0.65 ± 0.84 | 0.48 ± 0.67 | 0.56 ± 1.01 | 0.554 |
| Q9. Doctors exaggerate the ill effects of smoking | 2.10 ± 0.99 | 2.12 ± 0.99 | 1.22 ± 1.30 | 0.037d |
| Q10. People can smoke at places where ashtrays are available | 2.36 ± 0.74 | 2.27 ± 0.88 | 1.78 ± 0.97 | 0.075 |
| KTSND score | 13.76 ± 4.87 | 11.85 ± 4.74 | 8.33 ± 4.21 | 0.001e |
Values are presented as mean ± SD.
KTSND, Kano test for social nicotine dependence.
Comparison between three groups was done by analysis of variance test and Bonferroni’s correction was applied to the post hoc analysis.
No significant difference was seen in post hoc analysis.
Current smokers showed significantly higher value compared with ex- and non-smokers.
Current smokers showed significantly higher value compared with non-smokers.
Figure 1.
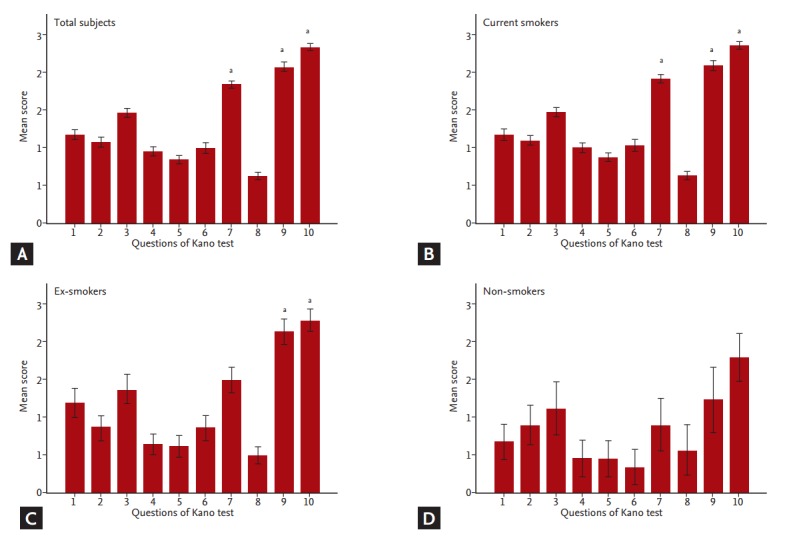
Mean comparison between the questions of Kano test. Significantly higher values were seen for Q7, Q9, and Q10 compared with the other questions, both in total subjects and in current smokers in (A) total subjects, (B) current smokers, (C) ex-smokers, and (D) non-smokers. The Q9 and Q10 values were also significantly higher than those for the other questions among ex-smokers. However, not all questions showed significant differences in non-smokers. ap < 0.05 compared with other questions (Q1 to 6 and Q8) by analysis of variance test and Bonferroni’s correction.
Table 4.
Fagerström test and Kano test for social nicotine dependence with other characteristics
| Characteristic | FTND |
KTSND |
||
|---|---|---|---|---|
| Mean ± SD | p valuea | Mean ± SD | p valuea | |
| Family member who smoke | 0.676 | 0.652 | ||
| Yes | 3.34 ± 2.09 | 13.39 ± 4.71 | ||
| No | 3.16 ± 2.70 | 13.06 ± 5.19 | ||
| Intention to quit smoking | 0.014 | 0.014 | ||
| Yes | 2.94 ± 2.04 | 13.00 ± 4.53 | ||
| No | 3.85 ± 2.41 | 14.72 ± 5.32 | ||
| Previous attempt of smoking cessation | 0.027 | < 0.001 | ||
| Yes | 3.05 ± 2.15 | 12.72 ± 4.68 | ||
| No | 3.85 ± 2.38 | 15.16 ± 4.97 | ||
FTND, Fagerström test for nicotine dependence; KTSND, Kano test for social nicotine dependence.
Comparison was done by t test.
The Spearman’s rank correlation coefficients between the scales (FTND and KTSND) and continuous variables (smoking amount per day, smoking year, age of smoking initiation, and current age) are shown in Table 5. The amount of smoking was correlated strongly with the FTND score but weakly with the KTSND score. The smoking year was correlated with the KTSND score and amount of smoking per day. The age of smoking initiation was correlated negatively with the FTND and KTSND scores and with the amount of smoking per day. Current age was correlated positively with smoking year and age of smoking initiation. The FTND and KTSND scores were not correlated.
Table 5.
Correlation coefficient of the scales and other parameters
| Parameter | KTSND | Smoking amount/day | Smoking years | Current age | Starting age of smoking |
|---|---|---|---|---|---|
| FTND | 0.110 | 0.601a | 0.122 | 0.040 | –0.214a |
| KTSND | - | 0.139b | 0.174a | 0.111 | –0.135b |
| Smoking amount/day | - | - | 0.167a | 0.115 | –0.159b |
| Smoking years | - | - | - | 0.866a | 0.030 |
| Current age | - | - | - | - | 0.348a |
KTSND, Kano test for social nicotine dependence; FTND, Fagerström test for nicotine dependence.
p < 0.01,
p < 0.05,
by Spearman correlation analysis.
DISCUSSION
We analyzed the smoking habits and physical and social nicotine dependence of North Korean male defectors while living in an education facility to prepare for settlement in South Korea. The mean age of the entire study population was 35.9 ± 11.3 years, mainly reflecting the 20- to 40-year age groups. The mean age of smoking initiation was 18.2 ± 4.7 years. A national survey of South Korean teenagers reported that the mean age of smoking initiation has decreased consistently from 14.1 years in 2005 to 13.5 years in 2013 [22]. Although the study populations differed, the age of smoking initiation in North Korea may not be significantly lower than that in South Korea and other countries [23,24]. In our study, 78.1% of smokers had family members who smoked, which may affect smoking prevalence among adolescents and those who suffer from second-hand smoke. Second-hand smoke exposure at home is prevalent (73%) among smoking adolescents worldwide [25].
Among our study subjects, 84.2% were current smokers, 12.5% were ex-smokers, and 3.3% were non-smokers. This rate of current smokers was much higher than the 59.5% smoking rate in North Korean adult men in the 2008 WHO report [9]. Compared with the adult male smoking rates in other countries according to the 2011 WHO report [26], 84.2% was the highest reported value. The adult male smoking rates are 67% in Indonesia and 47% in China [26]. Moreover, the ex-smokers among the North Korean defectors could resume smoking habits. The North Korean subjects had difficulties finding cigarettes during their escape, and they were in an education facility that discouraged smoking. The high smoking rate among colleague defectors also makes it difficult to abstain from smoking. The smoking rate was 96.7% in our study when current smokers and ex-smokers were combined.
Although the smoking rate was higher than our expectations, 67.4% of the current smokers intended to quit, and 70.6% of current and ex-smokers had attempted to quit smoking previously. Approximately 70% of current smokers in the USA and 55% of current smokers in South Korea intend to quit [27,28]. Our results indicate that North Korean defectors know the disadvantages of smoking and want to stop smoking. The smoking cessation success rate was 18.9% without any medical assistance. However, a long-term follow-up assessment is needed after leaving the educational facility.
The mean FTND score for current smokers was 3.35 ± 2.26. Ex-smokers answered the questionnaire according to their previous smoking experience. Fagerstrom et al. [29] defined high nicotine dependence as a score > 6 and low to moderate dependence as a score < 5 [30]. Withdrawal symptoms are more severe, smoking cessation is more difficult, and nicotine supplementation therapy is needed more frequently in the high nicotine dependence group [31]. The mean FTND scores were 4.85 ± 2.54 in 943 South Korean adult current smokers [32] and 3.7 ± 2.1 in 235 Japanese adult current smokers [18]. Current smokers tended to show higher scores than those of exsmokers, indicating that nicotine dependence in North Korean defectors may be less severe and that smoking cessation may be easier with appropriate consultation compared with South Koreans.
In this study, the mean KTSND scores were 13.76 ± 4.87, 11.85 ± 4.74, and 8.33 ± 4.21 in current smokers, ex-smokers, and non-smokers, respectively. Although no significant differences in the FTND score were observed between current and ex-smokers, the KTSND total scores and the scores to Q7 and Q9 were significantly different among current smokers, ex-smokers, and non-smokers. Jeong et al. [21] showed that the total KTSND scores of current smokers were significantly higher than those of ex-smokers, and of non-smokers from 741 South Korean subjects (17.1 ± 5.4 for current smokers vs. 14.3 ± 5.5 for ex-smokers and 12.3 ± 5.5 for non-smokers, p < 0.001).
The Q9 and Q10 scores were significantly higher compared with the other questions in current and ex-smokers, suggesting that subjects tended to answer these two questions with more confidence. Interestingly, Q9 (doctors exaggerate the ill effects of smoking) scored significantly higher compared with the other questions and significantly higher in current smokers compared with non-smokers. This result may indicate that a mutual understanding may be needed between smokers and a medical team for effective smoking cessation therapy.
The FTND and KTSND scores were significantly lower in subjects who intended to quit smoking and who had previously attempted to quit smoking, indicating that the will to stop smoking is an important factor in smoking cessation. Subjects with no will to quit smoking tended to be physically and socially more nicotine dependent. Younger men tended to start smoking earlier than did older men. Subjects who started smoking at a younger age smoked more per day and had higher physical and social nicotine dependence. These results indicate that smoking cessation programs for North Koreans should focus on the younger generations.
Our study had several limitations. Detailed data regarding safety and protection of personal information were not collected. In addition, North Korean defectors living in South Korea are not a perfect representation of the North Korean population. Age, occupation, and residence may differ between North Korean defectors and the general North Korean population. Women were also not included. Although North and South Korea use the same language, many words are different due to the long period of division between the countries. We explained the meaning of some words in the questionnaire, which may have affected the results.
In conclusion, the smoking rate in North Korean male defectors was higher than that previously thought. However, interest in smoking cessation was high and nicotine dependence was less severe than expected. Further investigation is needed to identify an efficient smoking cessation method for North Korean smokers, particularly those of younger generations.
KEY MESSAGE
1. The current smoking situation in North Korea was estimated with North Korean male defectors in South Korea.
2. The smoking rate in North Korean male defectors was 84.2% and higher than that previously thought.
3. However, interest in smoking cessation was high and nicotine dependence was less severe than expected.
Acknowledgments
The authors acknowledge the Hanawon, a government sponsored educational facility, for administering data collection.
Footnotes
No potential conflict of interest relevant to this article was reported.
REFERENCES
- 1.Godtfredsen NS, Holst C, Prescott E, Vestbo J, Osler M. Smoking reduction, smoking cessation, and mortality: a 16-year follow-up of 19,732 men and women from The Copenhagen Centre for Prospective Population Studies. Am J Epidemiol. 2002;156:994–1001. doi: 10.1093/aje/kwf150. [DOI] [PubMed] [Google Scholar]
- 2.Cowling DW, Yang J. Smoking-attributable cancer mortality in California, 1979-2005. Tob Control. 2010;19 Suppl 1:i62–i67. doi: 10.1136/tc.2009.030791. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.IARC Working Group on the Evaluation of Carcinogenic Risks to Humans Tobacco smoke and involuntary smoking. IARC Monogr Eval Carcinog Risks Hum. 2004;83:1–1438. [PMC free article] [PubMed] [Google Scholar]
- 4.Forey B, Hamling J, Lee P, Wald N. International Smoking Statistics: A Collection of Historical Data from 30 Economically Developed Countries. London: Oxford University Press; 2002. [Google Scholar]
- 5.Thun MJ, Carter BD, Feskanich D, et al. 50-year trends in smoking-related mortality in the United States. N Engl J Med. 2013;368:351–364. doi: 10.1056/NEJMsa1211127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Organization for Economic Cooperation and Development (OECD) Paris: OECD; c2015. OECD Health Data 2014 [Internet] [cited 2015 Dec 16]. Available from: http://stats.oecd.org/index.aspx?DataSetCode=HEALTH_STAT. [Google Scholar]
- 7.Kim IS, Jee SH, Ohrr H, Yi SW. Effects of smoking on the mortality of lung cancer in Korean men. Yonsei Med J. 2001;42:155–160. doi: 10.3349/ymj.2001.42.2.155. [DOI] [PubMed] [Google Scholar]
- 8.Zheng W, McLerran DF, Rolland BA, et al. Burden of total and cause-specific mortality related to tobacco smoking among adults aged ≥ 45 years in Asia: a pooled analysis of 21 cohorts. PLoS Med. 2014;11: doi: 10.1371/journal.pmed.1001631. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.World Health Organization (WHO) Geneva: WHO; c2008. WHO report on the global tobacco epidemic 2008: the MPOWER package [Internet] [cited 2015 Dec 16]. Available from: http://www.who.int/tobacco/mpower/mpower_report_full_2008.pdf. [Google Scholar]
- 10.Bondy SJ, Victor JC, Diemert LM. Origin and use of the 100 cigarette criterion in tobacco surveys. Tob Control. 2009;18:317–323. doi: 10.1136/tc.2008.027276. [DOI] [PubMed] [Google Scholar]
- 11.Lee YI, Lee SG, Kang DM, et al. Work-relatedness of lung cancer by smoking and histologic type in Korea. Ann Occup Environ Med. 2014;26:43. doi: 10.1186/s40557-014-0043-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Heatherton TF, Kozlowski LT, Frecker RC, Fagerstrom KO. The Fagerstrom test for nicotine dependence: a revision of the Fagerstrom tolerance questionnaire. Br J Addict. 1991;86:1119–1127. doi: 10.1111/j.1360-0443.1991.tb01879.x. [DOI] [PubMed] [Google Scholar]
- 13.Pomerleau CS, Carton SM, Lutzke ML, Flessland KA, Pomerleau OF. Reliability of the Fagerstrom tolerance questionnaire and the Fagerstrom test for nicotine dependence. Addict Behav. 1994;19:33–39. doi: 10.1016/0306-4603(94)90049-3. [DOI] [PubMed] [Google Scholar]
- 14.Etter JF, Duc TV, Perneger TV. Validity of the Fagerström test for nicotine dependence and of the heaviness of smoking index among relatively light smokers. Addiction. 1999;94:269–281. doi: 10.1046/j.1360-0443.1999.94226910.x. [DOI] [PubMed] [Google Scholar]
- 15.Fidler JA, Shahab L, West R. Strength of urges to smoke as a measure of severity of cigarette dependence: comparison with the Fagerström test for nicotine dependence and its components. Addiction. 2011;106:631–638. doi: 10.1111/j.1360-0443.2010.03226.x. [DOI] [PubMed] [Google Scholar]
- 16.Park SM, Son KY, Lee YJ, et al. A preliminary investigation of early smoking initiation and nicotine dependence in Korean adults. Drug Alcohol Depend. 2004;74:197–203. doi: 10.1016/j.drugalcdep.2004.01.001. [DOI] [PubMed] [Google Scholar]
- 17.Yoshii C, Kano M, Isomura T, et al. Innovative questionnaire examining psychological nicotine dependence, “The Kano test for social nicotine dependence (KTSND)”. J UOEH. 2006;28:45–55. doi: 10.7888/juoeh.28.45. [DOI] [PubMed] [Google Scholar]
- 18.Otani T, Yoshii C, Kano M, et al. Validity and reliability of Kano test for social nicotine dependence. Ann Epidemiol. 2009;19:815–822. doi: 10.1016/j.annepidem.2009.03.016. [DOI] [PubMed] [Google Scholar]
- 19.Kurioka N, Inagaki K, Yoshii C, Kano M. Investigation of the perception of female students towards tobacco smoking with the Kano test for social nicotine dependence (KTSND) in 2006. Jpn J Tob Control. 2007;2:62–67. [Google Scholar]
- 20.Hoshino K, Yoshii C, Nakakuki K, et al. The evaluation of the anti-smoking education in 5th and 6th grades elementary school students and junior high school students by KTSND. Jpn J Tob Control. 2007;2:96–101. [Google Scholar]
- 21.Jeong JH, Choi SB, Jung WY, et al. Evaluation of Social Nicotine Dependence Using the Kano Test for Social Nicotine Dependence (KTSND-K) Questionnaire in Korea. Tuberc Respir Dis. 2007;62:365–373. [Google Scholar]
- 22.Statistics Korea . Daejeon (KR): Statistics Korea; 2015. Age at initiation of smoking in adolescent [Internet] [cited 2015 Dec 16]. Available from: http://kosis.kr/statHtml/statHtml.do?orgId=117&tblId=DT_117_12_Y009&vw_cd=MT_ZTITLE&list_id=117_11758_008&seqNo=&lang_mode=ko&language=kor&obj_var_id=&itm_id=&conn_path=E1. [Google Scholar]
- 23.Kaleta D, Makowiec-Dąbrowska T, Dziankowska-Zaborszczyk E, Fronczak A. Predictors of smoking initiation: results from the Global Adult Tobacco Survey (GATS) in Poland 2009-2010. Ann Agric Environ Med. 2013;20:756–766. [PubMed] [Google Scholar]
- 24.Rosen L, Rozhavski V, Levine H, et al. Smoking initiation among Israeli adolescents: a 24-year time-to-event analysis. Prev Med. 2014;65:141–147. doi: 10.1016/j.ypmed.2014.05.020. [DOI] [PubMed] [Google Scholar]
- 25.Wang MP, Ho SY, Lo WS, Lam TH. Smoking family, secondhand smoke exposure at home, and nicotine addiction among adolescent smokers. Addict Behav. 2012;37:743–746. doi: 10.1016/j.addbeh.2012.02.016. [DOI] [PubMed] [Google Scholar]
- 26.World Health Organization (WHO) Geneva: WHO; c2008. WHO report on the global tobacco epidemic 2011 [Internet] [cited 2015 Dec 16]. Available from: http://whqlibdoc.who.int/publications/2011/9789240687813_eng.pdf. [Google Scholar]
- 27.Kim YJ. Predictors for successful smoking cessation in Korean adults. Asian Nurs Res (Korean Soc Nurs Sci) 2014;8:1–7. doi: 10.1016/j.anr.2013.09.004. [DOI] [PubMed] [Google Scholar]
- 28.Lee ES, Seo HG. The factors associated with successful smoking cessation in Korea. J Korean Acad Fam Med. 2007;28:39–44. [Google Scholar]
- 29.Fagerstrom KO, Kunze M, Schoberberger R, et al. Nicotine dependence versus smoking prevalence: comparisons among countries and categories of smokers. Tob Control. 1996;5:52–56. doi: 10.1136/tc.5.1.52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Lim G, Park I, Park S, Song S, Kim H, Kim S. Effectiveness of smoking cessation using motivational interviewing in patients consulting a pulmonologist. Tuberc Respir Dis (Seoul) 2014;76:276–283. doi: 10.4046/trd.2014.76.6.276. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Becona E, Garcia MP. Relation between the tolerance questionnaire (nicotine dependence) and assessment of carbon monoxide in smokers who participated in treatment for smoking. Psychol Rep. 1995;77(3 Pt 2):1299–1304. doi: 10.2466/pr0.1995.77.3f.1299. [DOI] [PubMed] [Google Scholar]
- 32.Lee SK, Kweon HJ, Lim DJ, et al. The usefulness of heavy smoking index as a test for nicotine dependence. J Korean Acad Fam Med. 2008;29:405–411. [Google Scholar]