

Abstract
The high incidence of tumor recurrence after resection of metastatic liver lesions remains an unsolved problem. Small tumor cell deposits, which are not detectable by routine clinical imaging, may be stimulated by hepatic regeneration factors after liver resection. It is not entirely clear, however, which factors are crucial for tumor recurrence.
The presented mouse model may be useful to explore the mechanisms that play a role in the development of recurrent malignant lesions after liver resection. The model combines the easy-to-perform and reproducible techniques of defined amounts of liver tissue removal and tumor induction (by injection) in mice. The animals were treated with either a single laparotomy, a 30% liver resection, or a 70% liver resection. All animals subsequently received a tumor cell injection into the remaining liver tissue. After two weeks of observation, the livers and tumors were evaluated for size and weight and examined by immunohistochemistry.
After a 70% liver resection, the tumor volume and weight were significantly increased compared to a laparotomy alone (p <0.05). In addition, immunohistochemistry (Ki67) showed an increased tumor proliferation rate in the resection group (p <0.05).
These findings demonstrate the influence of hepatic regeneration mechanisms on intrahepatic tumor growth. Combined with methods like histological workup or RNA analysis, the described mouse model could serve as foundation for a close examination of different factors involved in tumor growth and metastatic disease recurrence within the liver. A considerable number of variables like the length of postoperative observation, the cell line used for injection or the timing of injection and liver resection offer multiple angles when exploring a specific question in the context of post-hepatectomy metastases. The limitations of this procedure are the authorization to perform the procedure on animals, access to an appropriate animal testing facility and acquisition of certain equipment.
Keywords: Medicine, Issue 110, Liver resection, tumor recurrence, hepatic malignancy, mouse model, hepatic growth factor, endothelial growth factor, tissue growth factor, immunohistochemistry
Introduction
Colorectal cancer (CRC) accounts for nearly 9% of all malignant tumors. It is the third most common cancer, both in the U.S. and worldwide. Global mortality rates from CRC range from 300,000 to over 500,000 per year1. Twenty percent of patients suffer from liver metastases upon discovery of their colorectal tumor. Resectable metastases are normally treated by a partial liver resection2,3. Improved surgical techniques, new multimodal strategies and new definitions of resectable metastases render the therapy of a partial liver resection possible for an increasing number of patients4.
Recurrence of secondary liver malignancies, however, is a challenging clinical sequalae in modern gastrointestinal surgery. Patients with CRC who underwent resection of liver metastases have a 30 to 50% chance of developing a new tumor in their remnant liver5. Therefore, there is a need for further research on the mechanisms involved in recurrence of liver metastases.
A liver resection of about 70% is normally compensated within a few weeks by the remaining hepatic tissue. This regeneration involves multiple mechanisms, including cytokines like Interleukin 6 (IL-6), tumor necrosis factor alpha (TNF-α), hepatocyte growth factor (HGF), transforming growth factor beta (TGF-β), vascular endothelial growth factor (VEGF), matrix metalloproteases (MMP-2 and MMP-9) and CXC-Chemokines6-11. These substances support hepatic regeneration and may also be responsible for the high recurrence rates of primary and secondary liver malignancies by inducing the growth of small tumor cell deposits in the remaining liver which are not detected by routine clinical imaging. This causality has not been proven so far.
The following hypothesis was established. After partial liver resection, the proliferation factors that are responsible for liver hypertrophy may also induce the growth of previously undiscovered tumor cells in the liver. A mouse model was designed which combined the techniques of liver resection and tumor induction. Thirty athymic nude-foxn1nu/nu mice were divided into three groups of ten animals each. Each of them was treated with either a laparotomy alone (Group A), a 30% liver resection (Group B) or a 70% liver resection (Group C). Animals in all groups subsequently received a tumor cell injection into a defined remaining part of the liver, to simulate dormant tumor cells. Animals where observed for two weeks and then evaluated for tumor growth and liver hypertrophy.
The objective was to create a model that could be used to search for the molecular and pathogenetic factors that may play a role in post-hepatectomy tumor formation. This method may be helpful in assessing: the origin of endocrine factors involved in liver regeneration; the responsible mechanisms for intrahepatic tumor growth after liver resection; and the liver resection volume necessary for intrahepatic tumor growth induction. The following method has only been performed on animals because they promise to contribute to the understanding of fundamental biological principles and to the development of knowledge that can be expected to benefit humans by improved treatment options. Due to the mechanisms involved in these matters, it had to be examined in vivo, as in vitro methods may not provide a realistic representation of the human pathology.
These investigations may lead to the discovery of relevant targets for prophylactic treatment options for decreasing tumor recurrence.
Protocol
The government of Middle Franconia in Bavaria, Germany, granted permission for the procedures described. Any similar experiments require prior authorization by the appropriate authorities.
Note: The following manual can be used for previously discussed groups A through C. Steps that have to be left out in groups A and B are marked accordingly.
1. Preparations
Put on gloves, place the polystyrene pad underneath the microscope, and focus the lens on the area slightly above the pad.
Split the sterile sheet and place half over the polystyrene pad and the other half just next to it.
Sterilize the surgical instruments and place them on a sterile sheet next to the Polystyrene pad.
Unbend a large paper clip to form an arch. Turn it upside down and press it into the polystyrene pad at the top end - just next to where the animal's head will lie.
Place the mouthpiece of the vaporizer between the two limbs of the arch. (Figure 7)
Set up a heating lamp about 40 cm from the place where the animal's head will lie. Make sure the heat at the level of the polystyrene pad does not exceed 40 °C.
Prepare a separate cage for operated animals.
Prepare a defined quantity and volume (maximum of 50 µl) of tumor cells in a flex tube and store it on ice.
2. Anesthesia
Place the mouse into a plexiglas box and begin anesthetic induction on high flow isoflurane (5% isoflurane at a flow of 10 L/min).
After going through the different stages of anesthesia, remove the mouse from the plexiglas box just after it has entered the stage of agonal breathing, which can easily be recognized by a drastic decrease in respiratory rate (<20/min) and deep gasps shaking the animal's entire body.
Quickly place the animal belly-up onto the sterile drape covered polystyrene pad and continue ventilation on low-flow isoflurane by inserting the mouse's snout into the mouthpiece to maintain anesthesia. Use an inspiratory fraction of 1.8-2.2% at a flow of about 1 L/min.
Evaluate the depth of anesthesia during the operation by calculating the respiratory frequency, which is ideally between 45 and 60 breaths per min. Adapt the inspiratory isoflurane fraction accordingly if this is not the case. Note: Changes in the inspiratory isoflurane fraction take about 60 sec until they become effective. Avoid carrying out drastic changes rapidly. Instead, modify the anesthetic's application gradually.
3. Operation
Disinfect the chest and abdomen with an adequate disinfectant and change gloves afterwards.
Inject a weight-adapted volume of carprofen (5 mg/kg bodyweight) into the animal's thigh.
Gently pinch the abdominal skin with a forceps to test if the depth of anesthesia is adequate.
Perform an incision along the median line from the xiphoid to the mid-abdomen using scissors and forceps.
Carefully dissect the area around the xiphoid to expose it from the surrounding tissue.
Place a stay suture through the xiphoid (from inside to outside) and attach both threads to the retainer above the animals head using the clamp.
Pinch the retractor's limbs together and slowly introduce the "U"-shaped retractor tips along the animal's internal abdominal wall. Note: These measures expose the liver to facilitate access to the different lobes. The identification of the liver's median and left lateral lobe should now be possible.
Use a saline-soaked cotton swab and gently push the median lobe downwards. Dissect the ventral three quarters of the falciform ligament, which will now be visible between the median lobe's surface and the diaphragm.
Now, use two saline-soaked cotton swabs to shift the median lobe and left lateral lobe upwards against the diaphragm.
Visualize the thin membrane between the left lateral lobe and the caudate lobe and carefully dissect it. Note: When performing this protocol on animals from group A, jump to step 3.18 at this point.
Place a size 4-0 ligature diagonally along the left lateral lobe's base.
Next, use the cotton swab to return the left lateral lobe to its original position.
Carefully tie the ligature as close to the lobe's base as possible and assess for color change in the lobe to test for adequately interrupted blood supply.
Resect the left lateral lobe by following the line of the lobe's base and note the resected lobe's weight. Note: When performing this protocol on animals from group B, jump to step 3.18 at this point.
Place a second ligature between the left lateral lobe's stump and the median lobe's base.
Reposition the median lobe as well and tie the ligature. Again, assess for color change in the lobe to test for adequately interrupted blood supply.
Resect the median lobe and note its weight.
Connect the 1 ml syringe to the 30 G needle and fill it with the tumor cells from the flex tube without tilting the syringe at any time.
Use the cotton swabs to move the intestinal loops to the animal's left in order to expose the inferior right lobe.
Insert the cell-loaded syringe into the "third-hand" device at a 30° angle to the vertical.
Carefully move the device next to the mouse with the needle just above the inferior right lobe.
Slowly advance the syringe within the third hand device until the needle's tip is in the inferior right lobe's center part.
Inject the entire volume into the lobe's center part over a period of 30-45 sec.
Compress the injection site for at least three minutes until bleeding has stopped.
Remove the stay suture and the retractor.
Close the fascia with a resorbable 5-0 suture using single button knots.
Close the skin with a 4-0, non-resorbable suture using single button knots.
Start ventilating the mouse on high flow oxygen for about 1 min.
4. Post-op procedure
Place the animal into a warm environment (approximately 40 °C) for the next half hour to ensure adequate recovery.
Admix the animal's drinking water with 5 mg/ml of metamizole for 72 hr postoperative.
Examine the integrity of the sutures closely for at least three days after the procedure.
5. Observation Period and Euthanasia
Measure the animal's weight daily for a total of 14 days. Score them regarding their well-being and limitations respectively.
After 14 days, anesthetize the animal following steps 2.1 and 2.2 of the operative protocol and proceed with institution's protocol for animal euthanasia.
Perform a median laparotomy as explained in step 3.4. To facilitate access to the abdomen, extend the incision 1-1.5 cm caudally. Insert the retractor as pointed out in 3.7.
Dissect along the rest of the falciform ligament and cut the inferior vena cava just as it exits the liver cranially.
Separate the liver from the diaphragm, by grabbing the diaphragm with the forceps and bluntly dissecting into the space between liver and muscle tissue.
Lift the mobilized liver tissue off the retroperitoneum and dissect it off the remaining structures it is still attached to: retroperitoneal fatty tissue, the inferior vena cava and the portal vein.
Inspect the liver after extraction for any additional tissue, which would falsely contribute to its actual size and weight. An extracted liver and its tumor are displayed in Figure 6.
Dissect the tumor off the inferior right lobe.
Measure the size and weight of both the tumor and the liver parenchyma.
Conserve additional tissue samples from the peritoneum, lymph nodes or other organs as needed for tissue analysis
Representative Results
In our specific experiment, we included 30 athymic nude-foxn1nu/nu mice. They received a median laparotomy, tumor cell injections of 500,000 MC38 tumor cells (dissolved in 50 µl of saline), and were subsequently treated with either a 70% liver resection, a 30% liver resection, or no further intervention.
After 14 days, almost complete regeneration of the remaining liver following 30% or 70% liver resections (liver hypertrophy-index of the 30% liver resection group was 1.06 versus 0.8 from the 70% liver resection group) was observed.
After a single laparotomy, the average weight of intrahepatic tumors was 332 mg (range: 10-608 mg). The mean tumor weight of intrahepatic tumors was 656 mg (range: 76-1,873 mg) after a 30% liver resection vs. 961 mg (range: 189 mg- 3030 mg) after a 70% liver resection with p<0.05 (Figure 1). After a 30% liver resection, tumor volume was 950 mm3 (range: 439-2,326 mm3) vs. 1,385 mm3 (range: 411-2,366 mm3) after a 70% liver resection, and 511 mm3 (range: 87-1,693 mm3) after a laparotomy alone with p <0.05 (Figure 2).
Tissue sections from the tumor tissue were taken and analyzed via KI-67 immunohistochemistry. Cells on the slides were evaluated regarding their proliferation rate. The average proliferation rate of tumor cells from the laparotomy group was 47% (range: 39-56%) compared to 61% (range: 51-69%) from animals that had undergone a liver resection of 70% (p <0.05) and 53% (range: 38-69%) from animals that had undergone a liver resection of 30% (p = 0.22), demonstrating an increased rate of cell proliferation in groups that underwent liver resection (Figures 3-5).
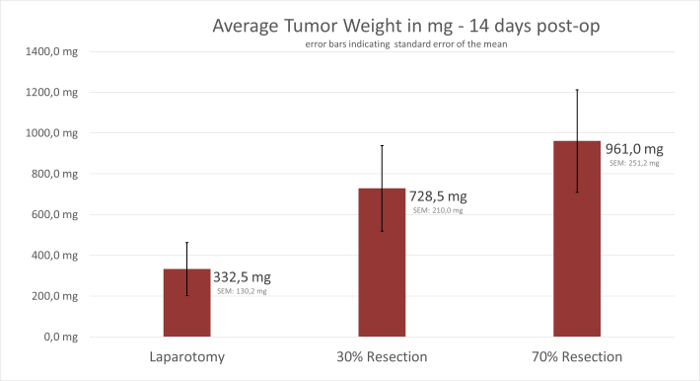 Figure 1: Weight of Intrahepatic Tumors. The diagram compares the average tumor weight among groups A, B and C after dissection from the liver and shows increased weight in tumors of group B and C. Error bars represent SEM. Please click here to view a larger version of this figure.
Figure 1: Weight of Intrahepatic Tumors. The diagram compares the average tumor weight among groups A, B and C after dissection from the liver and shows increased weight in tumors of group B and C. Error bars represent SEM. Please click here to view a larger version of this figure.
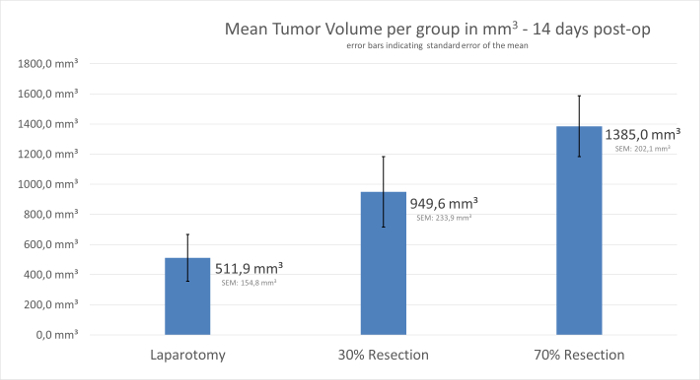 Figure 2: Volume of Intrahepatic Tumors. The diagram compares the average tumor volume among groups A, B and C after dissection from the liver and shows increased volumes in tumors of group B and C. Error bars represent SEM. Please click here to view a larger version of this figure.
Figure 2: Volume of Intrahepatic Tumors. The diagram compares the average tumor volume among groups A, B and C after dissection from the liver and shows increased volumes in tumors of group B and C. Error bars represent SEM. Please click here to view a larger version of this figure.
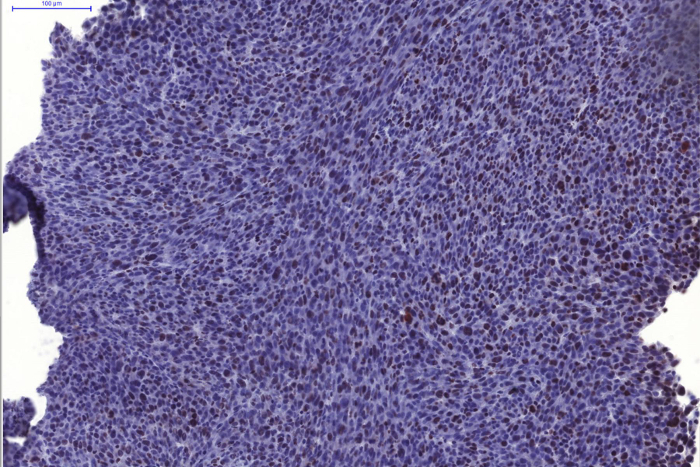 Figure 3: Proliferation Rate in tumors from Group A. KI-67 Immunohistochemistry of a slide from a tumor specimen from group A demonstrates mild proliferation of tumor cells. Scale bar = 100 µm. Please click here to view a larger version of this figure.
Figure 3: Proliferation Rate in tumors from Group A. KI-67 Immunohistochemistry of a slide from a tumor specimen from group A demonstrates mild proliferation of tumor cells. Scale bar = 100 µm. Please click here to view a larger version of this figure.
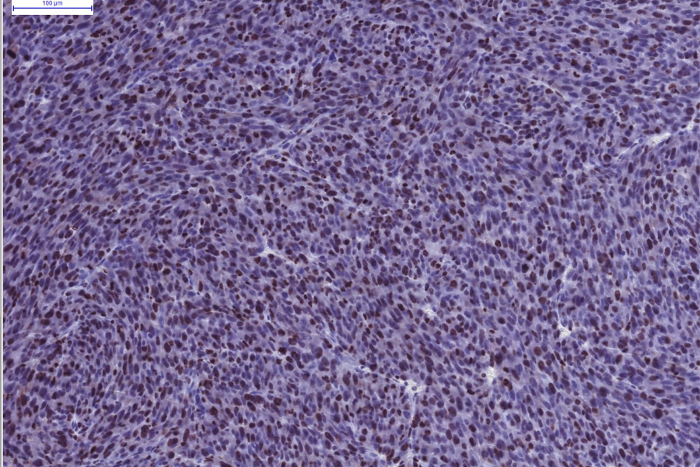 Figure 4: Proliferation Rate in tumors from Group B. KI-67 Immunohistochemistry of a slide from a tumor specimen from group B demonstrates moderate proliferation of tumor cells. Scale bar = 100 µm. Please click here to view a larger version of this figure.
Figure 4: Proliferation Rate in tumors from Group B. KI-67 Immunohistochemistry of a slide from a tumor specimen from group B demonstrates moderate proliferation of tumor cells. Scale bar = 100 µm. Please click here to view a larger version of this figure.
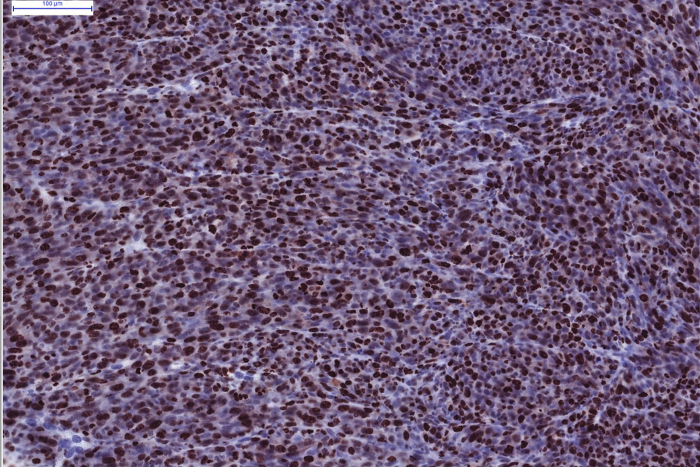 Figure 5: Proliferation Rate in tumors from Group C. KI-67 Immunohistochemistry of a slide from a tumor specimen from group C demonstrates marked proliferation of tumor cells. Scale bar = 100 µm. Please click here to view a larger version of this figure.
Figure 5: Proliferation Rate in tumors from Group C. KI-67 Immunohistochemistry of a slide from a tumor specimen from group C demonstrates marked proliferation of tumor cells. Scale bar = 100 µm. Please click here to view a larger version of this figure.
 Figure 6: Extracted Liver/Tumor specimen from Group B. This liver was extracted 14 days after performing a 30% liver resection and simultaneous tumor cell injection. A large tumor in the right inferior lobe can be seen, while the right superior, median and caudate lobes have gone through significant hypertrophy. * = tumor in the inferior right lobe, SRL = superior right lobe, ML = median lobe, CL = caudate lobe. Please click here to view a larger version of this figure.
Figure 6: Extracted Liver/Tumor specimen from Group B. This liver was extracted 14 days after performing a 30% liver resection and simultaneous tumor cell injection. A large tumor in the right inferior lobe can be seen, while the right superior, median and caudate lobes have gone through significant hypertrophy. * = tumor in the inferior right lobe, SRL = superior right lobe, ML = median lobe, CL = caudate lobe. Please click here to view a larger version of this figure.
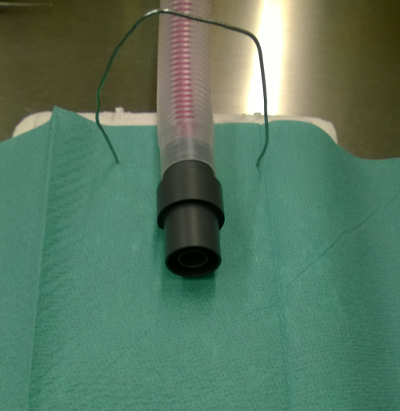 Figure 7: OR Table Setup. The polystyrene pad is covered by a sterile cloth. A bent open paper clip is pressed into the pad at its upper end overlying the breathing tube with its mouthpiece. Please click here to view a larger version of this figure.
Figure 7: OR Table Setup. The polystyrene pad is covered by a sterile cloth. A bent open paper clip is pressed into the pad at its upper end overlying the breathing tube with its mouthpiece. Please click here to view a larger version of this figure.
Discussion
Previous experiments performing surgery in rodents have been able to identify certain variables that could serve as sources for bias. In order to obtain reliable and valid results, consider the following precautions.
Routine pre-op fasting can lead to liver steatosis12, which may inhibit liver regeneration13,14. It is therefore not recommended. The highest mitotic activity of hepatocytes varies throughout the day15. If possible, conduct the procedures at a certain time during the day for all groups. Murine liver regeneration is most effective in animals 4-6 weeks old. Animals older than 10 months of age have a significantly decreased regeneration capacity16. Use mice of the same race, sex and age for the experiments to minimize the chance of bias. Working in a sterile environment is generally important in an open procedure like this. Especially in immunocompromised organisms, like the athymic mice used in the video, the risk of infection, which may lead to premature death or biased results, is high. Pursuing a three-zone-setup consisting of a preparation, a surgery and a recovery area is therefore warranted17. Due to its profound hepatotoxic effects, commonly used buprenorphine is not recommended for intra- or postoperative analgesic therapy18,19. Use other substances like carprofen or metamizole to provide adequate analgesia. Since metamizole is not available in many countries, carprofen may also be used for pain control after the procedure. Perform a subcutaneous injection of 5mg/kg bodyweight once daily for three days to substitute metamizole.
Postoperative recovery is best achieved when the recovering mouse is placed into a warm environment with easy access to food and water. It is ideally isolated from other mice overnight, to prevent more dominant animals from harming more vulnerable ones17.
Although the protocol is very straightforward, there are some minor pitfalls to avoid when performing this kind of surgery in mice. Dissection of the falciform ligament, a structure connecting the ventral aspect of the median lobe to the abdominal wall, is essential to achieve appropriate liver flexibility. As this ligament expands to an area very close to the point where the inferior vena cava leaves the liver cranially, caution is warranted in order to prevent damage to this major vein. On average, dissecting it about three quarters of the way will ensure satisfactory mobilization and at the same time maintain adequate distance to the vessel.
Using the right amount of tension when ligating a lobe with a ligature is a tremendously important task when performing the resection protocol. Ligatures with air knots or poorly tightened ligatures can lead to inadequately interrupted blood supply, hemorrhage, shock and death. At the same time, an attempt to thoroughly tighten a ligature knot may result in ligature rupture with associated damage to surrounding tissue and organs. An effective way of assessing ligature integrity is the observation of cyanotic color change within the ligated lobe. Selecting the correct suture material also plays an important role. Braided sutures are more likely to compress tissue, whereas monofilamentous materials will rather dissect through the soft liver tissue and causes hemorrhage.
Another critical step when removing liver lobes in mice involves correct positioning of ligatures. Ligation ought to be performed perpendicular to the main vessels entering the lobes. While this is rather straightforward in the median lobe, adequate resection of the left lateral lobe is more challenging. Its vessels enter the lobe in a ventro-caudal direction. As a result, the ligature thread must be placed along an imaginary line between the left lunge base to the inferior right lobe of the liver.
In the median lobe, however, resection may compromise the inferior vena cava. Because this major vessel runs through the dorsal portion of the lobe, it is prone to damage, which may lead to liver necrosis. Furthermore, tying the ligature with too much tension in this area, may result in diaphragm rupture and/or pneumothorax.
Adequate handling of tumor cells is also important when trying to obtain comparable results. Although the exact cell culture techniques are not meant to be part of this protocol, the handling of tumor cells within the procedure is as important as perfect preparation beforehand. When filling the syringe with the tumor cells, it is vital to keep it upright at all times. Major tilting of the syringe may result in tumor cells adhering to the syringes wall, therefore resulting in loss of cells at the time of injection. Only minor tilting is warranted at the time of injection, in order to insert the needle perpendicular to the inferior right lobe's surface.
Hemorrhage and peritoneal metastases may occur as a result of bleeding and spillage from the puncture site on the liver's surface. Hence, gentle compression of the lobe with a cotton swab for a period of three minutes is essential to control bleeding from the liver parenchyma and prevent tumor cell fluid leaking into the peritoneum.
Publications containing procedure protocols for intraabdominal operations in rodents rarely contain information about the type of abdominal closure. Yet, this aspect is another possible source of complications. Even with adequate pain control, animals will try to remove the foreign bodies in their abdominal wall. Consequences may be intraabdominal infection, an open abdomen or even death. This can be prevented by both performing single interrupted stitches for wound closure instead of a running suture and closing the abdominal wall in two layers.
Female athymic nude-foxn1nu/nu mice (provided by Harlan Laboratories B.V., Kreuzelweg 53, NL-5961 NM Horst) were used in this experiment. The T-cell deficiency this breed is known for allows relatively unrestricted tumor growth and therefore ideal conditions for tumor implantation. In order to minimize the influence of ranking fights among the animals, only female animals were used. Preliminary results using different strains like the C57BL/6 Inbred Mice have also shown significant, yet lower volume tumor growth. Thus, the technique may very likely be practicable in even more mouse strains.
Yet, using immunocompromised organisms in this setting requires special animal hygiene precautions, as pathogens may interfere with tumor growth20. Measures like the use of sentinel animals to monitor the presence of pathogenic agents21 as performed in the animal testing facility our study took take place in can be helpful in detecting possible sources of bias.
This experiment used a murine colorectal cancer cell line called MC38 (obtained from the Institute of Clinical Chemistry at the Medical Faculty of Mannheim, Germany). 5 x 105 tumor cells were dissolved into 50 µl of saline. The concentration was determined in preliminary experiments, where this amount was identified as ideal for solid tumor formation within two weeks. Depending on the immunocompetence of the animals used in these experiments (see discussion above), it might very well also be possible to use human colorectal cancer cells and therefore create a xenograft. Initial testing performed in athymic nude-foxn1nu/nu mice using human SW480 tumor cells was able to successfully demonstrate tumor growth in the remnant liver after resection. Due to the dimension of murine livers, it is recommended to only use volumes up to 50 µl to prevent complications. A possible enhancement at this point would be to label tumor cells with luciferase. Depending on the problem that is being investigated, interesting information may arise when closer monitoring of tumor cell growth and size is possible.
Alternative ways of ligating liver lobes include the clipping method22 or a clipping-suturing hybrid technique23. Positioning of clipping devices, however, may render the clipping methods difficult. Adequately performed suture ligation remains an easy to learn technique and is very likely to be the most cost effective way of removing a lobe in this experiment.
Because live animals are used in this experiment, it requires prior permission by the appropriate authorities. Depending on the region, this can be a costly and time-consuming task. Even after official approval, animal experiments are far less accessible than research methods like cell culture testing or molecular methods. In addition to the infrastructure of a modern animal testing facility, special equipment has to be allocated in order to perform the protocol. Furthermore, a period of two to four weeks should be scheduled to master this technique. This protocol may applicable for a wide range of cell lines in a large number of mouse strains. Yet, with respect to the possible modifications mentioned above, not every cell line may be studied in every organism.
A main target of investigative studies using this protocol will be the complex growth factor system involved in liver regeneration and its exact effects on liver malignancy recurrence. In order to investigate these possible correlations adequately, it is essential to implement an animal experiment, in contrast to different molecular methods or cell culture experiments. These methods should rather be used as complimentary means of investigation. Although several different liver resection models have been published so far22-24, this procedure for the first time implements simultaneous tumor cell injection into a well-established operation.
This mouse model demonstrates that liver resection in mice is a fairly simple, feasible and easily reproducible method. The liver's regeneration after minor and major resections was able to compensate the tissue loss by hypertrophy within two weeks. Mice can cope with liver volume reductions of up to 70%.
Tumor cells were able to grow inside the remnant liver and solid tumors can be established. Tumor growth and tumor cell proliferation correlated with the amount of resected liver tissue. The process of resection lead to an activation of tumor growth within the remaining liver, which was expressed, by greater tumor weights and volumes. This greater degree of proliferation could be demonstrated by immunohistochemistry examinations.
It is well known that the amount of hepatic regeneration factors released for liver hypertrophy increases with the extent of liver resection25,26. Therefore, a link between liver regeneration factors and tumor cell growth may exist. This is in concordance with clinical observations where metastatic recurrence correlates with the amount of metastases within the liver prior to resection. Liver metastases that are visible on preoperative imaging may only reflect the tip of the iceberg while more, not yet detectable tumor cell deposits, may be present at diagnosis. After liver resection, hepatic regeneration factors may then stimulate the growth of these tumor cells, which eventually become evident as recurrent metastases.
Although the correlation mentioned above is very likely, it has not been proven so far. The influence of hepatic regeneration mechanisms on intrahepatic tumor progress therefore requires further molecular analyzes. Precise instructions as well as an illustrative video allow a rapid adoption of the technique introduced in this video. It can serve as a foundation for different kinds of studies around the world that are trying to discover the missing link in this well-known chain of events.
Disclosures
The authors have nothing to disclose.
Acknowledgments
Special acknowledgements go to Dr. Benjamin Motsch for his assistance in technical questions. The authors would also like to acknowledge Dr. Marcus Forschner and Birk Müller for their multimedia support, Erica Magelky for her editorial expertise and Lisa Hornung, Dr. Roland Jurgons and Professor Stephan von Hörsten (all from the Franz-Penzoldt-Center, University of Erlangen) for their professionalism in animal handling and care. We thank Professor Michael Neumaier at the Institute of Clinical Chemistry, Medical Faculty Mannheim of the University of Heidelberg, Germany for providing MC38 tumor cells.
The present work was performed in fulfillment of the requirements for obtaining the degree "Dr. med." at the Friedrich-Alexander-University Erlangen-Nürnberg (FAU).
References
- Haggar FA, Boushey RP. Colorectal cancer epidemiology: incidence, mortality, survival, and risk factors. Clin. Colon Rectal Surg. 2009;22:191–197. doi: 10.1055/s-0029-1242458. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fong Y, et al. Liver resection for colorectal metastases. J. Clin. Oncol. 1997;15:938–946. doi: 10.1200/JCO.1997.15.3.938. [DOI] [PubMed] [Google Scholar]
- Kato T, et al. Therapeutic results for hepatic metastasis of colorectal cancer with special reference to effectiveness of hepatectomy: analysis of prognostic factors for 763 cases recorded at 18 institutions. Dis. Colon Rectum. 2003;46:S22–S31. doi: 10.1097/01.DCR.0000089106.71914.00. [DOI] [PubMed] [Google Scholar]
- Poston GJ, et al. OncoSurge: a strategy for improving resectability with curative intent in metastatic colorectal cancer. J. Clin. Oncol. 2005;23:7125–7134. doi: 10.1200/JCO.2005.08.722. [DOI] [PubMed] [Google Scholar]
- Neumann UP, Seehofer D, Neuhaus P. The surgical treatment of hepatic metastases in colorectal carcinoma. Dtsch Arztebl Int. 2010;107:335–342. doi: 10.3238/arztebl.2010.0335. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Alwayn IP, et al. A critical role for matrix metalloproteinases in liver regeneration. J. Surg. Res. 2008;145:192–198. doi: 10.1016/j.jss.2007.04.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fausto N, Campbell JS, Riehle KJ. Liver regeneration. Hepatology. 2006;43:S45–S53. doi: 10.1002/hep.20969. [DOI] [PubMed] [Google Scholar]
- Fujiyoshi M, Ozaki M. Molecular mechanisms of liver regeneration and protection for treatment of liver dysfunction and diseases. J. Hepatobiliary. Pancreat. Surg. 2011;18:13–22. doi: 10.1007/s00534-010-0304-2. [DOI] [PubMed] [Google Scholar]
- Jin X, et al. Paradoxical effects of short- and long-term interleukin-6 exposure on liver injury and repair. Hepatology. 2006;43:474–484. doi: 10.1002/hep.21087. [DOI] [PubMed] [Google Scholar]
- Nakamura T, Sakai K, Nakamura T, Matsumoto K. Hepatocyte growth factor twenty years on: Much more than a growth factor. J. Gastroenterol. Hepatol. 2011;26:188–202. doi: 10.1111/j.1440-1746.2010.06549.x. [DOI] [PubMed] [Google Scholar]
- Van Sweringen HL, et al. CXC chemokine signaling in the liver: impact on repair and regeneration. Hepatology. 2011;54:1445–1453. doi: 10.1002/hep.24457. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heijboer AC, et al. Sixteen hours of fasting differentially affects hepatic and muscle insulin sensitivity in mice. J. Lipid Res. 2005;46:582–588. doi: 10.1194/jlr.M400440-JLR200. [DOI] [PubMed] [Google Scholar]
- Yang SQ, Lin HZ, Mandal AK, Huang J, Diehl AM. Disrupted signaling and inhibited regeneration in obese mice with fatty livers: implications for nonalcoholic fatty liver disease pathophysiology. Hepatology. 2001;34:694–706. doi: 10.1053/jhep.2001.28054. [DOI] [PubMed] [Google Scholar]
- Selzner M, Clavien PA. Failure of regeneration of the steatotic rat liver: disruption at two different levels in the regeneration pathway. Hepatology. 2000;31:35–42. doi: 10.1002/hep.510310108. [DOI] [PubMed] [Google Scholar]
- Matsuo T, et al. Control mechanism of the circadian clock for timing of cell division in vivo. Science. 2003;302:255–259. doi: 10.1126/science.1086271. [DOI] [PubMed] [Google Scholar]
- Iakova P, Awad SS, Timchenko NA. Aging reduces proliferative capacities of liver by switching pathways of C/EBPalpha growth arrest. Cell. 2003;113:495–506. doi: 10.1016/s0092-8674(03)00318-0. [DOI] [PubMed] [Google Scholar]
- Pritchett-Corning KR, Luo Y, Mulder GB, White WJ. Principles of rodent surgery for the new surgeon. J Vis Exp. 2011. [DOI] [PMC free article] [PubMed]
- Skoulis NP, James RC, Harbison RD, Roberts SM. Depression of hepatic glutathione by opioid analgesic drugs in mice. Toxicol. Appl. Pharmacol. 1989;99:139–147. doi: 10.1016/0041-008x(89)90119-1. [DOI] [PubMed] [Google Scholar]
- Berson A, et al. Mechanisms for experimental buprenorphine hepatotoxicity: major role of mitochondrial dysfunction versus metabolic activation. J. Hepatol. 2001;34:261–269. doi: 10.1016/s0168-8278(00)00050-7. [DOI] [PubMed] [Google Scholar]
- Baker DG. Natural pathogens of laboratory mice, rats, and rabbits and their effects on research. Clin. Microbiol. Rev. 1998;11:231–266. doi: 10.1128/cmr.11.2.231. [DOI] [PMC free article] [PubMed] [Google Scholar]
- FELASA working group on revision of guidelines for health monitoring of rodents and rabbits. FELASA recommendations for the health monitoring of mouse, rat, hamster, guinea pig and rabbit colonies in breeding and experimental units. Lab. Anim. 2014;48:178–192. doi: 10.1177/0023677213516312. [DOI] [PubMed] [Google Scholar]
- Nikfarjam M, Malcontenti-Wilson C, Fanartzis M, Daruwalla J, Christophi C. A model of partial hepatectomy in mice. J. Invest. Surg. 2004;17:291–294. doi: 10.1080/08941930490502871. [DOI] [PubMed] [Google Scholar]
- Hori T, et al. Simple and reproducible hepatectomy in the mouse using the clip technique. World J. Gastroenterol. 2012;18:2767–2774. doi: 10.3748/wjg.v18.i22.2767. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mitchell C, Willenbring H. A reproducible and well-tolerated method for 2/3 partial hepatectomy in mice. Nat. Protoc. 2008;3:1167–1170. doi: 10.1038/nprot.2008.80. [DOI] [PubMed] [Google Scholar]
- Sowa JP, et al. Extent of liver resection modulates the activation of transcription factors and the production of cytokines involved in liver regeneration. World J. Gastroenterol. 2008;14:7093–7100. doi: 10.3748/wjg.14.7093. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bonninghoff R, et al. Effect of different liver resection methods on liver damage and regeneration factors VEGF and FGF-2 in mice. Can. J. Surg. 2012;55:389–393. doi: 10.1503/cjs.007911. [DOI] [PMC free article] [PubMed] [Google Scholar]