

Abstract
Split-hand/split-foot malformation (SHFM) is mainly inherited as an autosomal dominant trait with incomplete penetrance and characterized by malformation of the limb involving the central rays of the autopod. It presents with a deep median cleft of the hand and/or foot, aplasia/hypoplasia of the phalanges, metacarpals, and metatarsals. Pathogenic mechanism is a failure to maintain signaling from the median apical ectodermal ridge. Without this signaling, cells of the underlying progress zone stop proliferation and differentiation which in turn results in defects of the central rays. We describe a case of SHFM in 10-year-old boy.
Keywords: Autosomal dominant, ectodermal ridge, ectrodactyly, split-hand/foot malformation
Introduction
Split-hand/split-foot malformation (SHFM) is also known as ectrodactyly. It is a malformation of the limb involving the central rays of the autopod and presenting with a deep median cleft of the hand and/or foot, aplasia/hypoplasia of the phalanges, metacarpals, and metatarsals. It can occur as part of a syndrome or isolated entity. The incidence of SHFM is around 1 in 90,000 live births.[1] SHMS expresses in two ways, one is nonsyndromic, where the isolated involvement of limbs occurs and other is associated anomalies known as syndromic form.[2] We report a nonsyndromic case of SHFM.
Case Report
A 10-year-old boy, second child of physically normal parents, presented with deformed hands and feet since birth. In hands, bilateral syndactyly, aplasia of the phalanges and metacarpals was seen in Figure 1. The X-ray of the hand [Figure 2] showed absence of first metacarpal and multiple phalanges in both the hands. Both the feet had deep midline cleft [Figure 1a and b] and syndactyly. X-ray showed absence of multiple metatarsals and phalanges in both the feet. There were no other dysmorphic features. Anthropometric measurements were within normal limits. Physical and systemic examination were normal. Developmentally appropriate for the age. He was a product of nonconsanguineous marriage and term normal delivery with no significant perinatal events. The index case was second in birth order. There was no facial dysmorphism in the patient. The two siblings of the index case were physically normal. The probable inheritance pattern in our case is autosomal recessive as no other sibling or other family members are affected.
Figure 1.
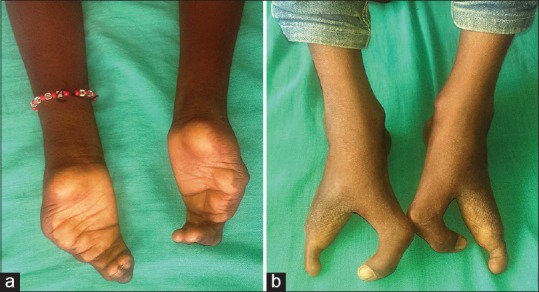
(a) Median clefts of feet and (b) syndactyly of hands
Figure 2.

X-ray showing aplasia/hypoplasia of the phalanges (a), metacarpals and metatarsals (b)
Discussion
SHFM is developed due to a failure of median apical ectodermal ridge activity, which leads to increased cell death or reduced cell proliferation. Defects in genes among antero-posterior signaling (Shh), proximo-distal signaling (Tp63, Dlx5/6) or dorsoventral signaling (Lrp6, Dkk1), can also cause SHFM.[3]
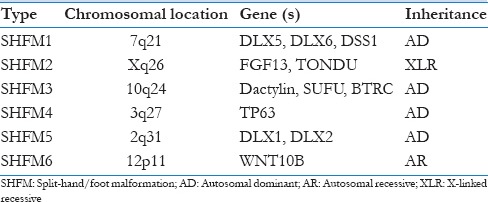
SHFM is commonly inherited as autosomal dominant mode with reduced penetrance. Some cases have been reported to have been inherited as autosomal recessive and X-linked forms.[4,5] Six types SHFM have been described till now [Table 1], among which type I is most common variety. Chromosomal rearrangement leads to association of ectrodactyly with other abnormalities. Disorders associated with ectrodactyly are ectrodactyly-cleft palate syndrome, ectrodactyly-ectodermal dysplasia-clefting syndrome, ectrodactyly-fibular aplasia/hypoplasia syndrome, ectrodactyly-ectodermal dysplasia-macular dystrophy syndrome, and ectrodactyly-polydactyly.[6] SHFM may need surgical treatment to the improve function and appearance. Parents should be counseled regarding the possibility of recurrence of the disease in the future siblings.
Table 1.
Types of split hand/foot malformation
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Barsky AJ. Cleft hand: Classification, incidence, and treatment. Review of the literature and report of nineteen cases. J Bone Joint Surg Am. 1964;46:1707–20. [PubMed] [Google Scholar]
- 2.Pinette M, Garcia L, Wax JR, Cartin A, Blackstone J. Familial ectrodactyly. J Ultrasound Med. 2006;25:1465–7. doi: 10.7863/jum.2006.25.11.1465. [DOI] [PubMed] [Google Scholar]
- 3.Duijf PH, van Bokhoven H, Brunner HG. Pathogenesis of split-hand/split-foot malformation. Hum Mol Genet. 2003;12:R51–60. doi: 10.1093/hmg/ddg090. [DOI] [PubMed] [Google Scholar]
- 4.Gül D, Oktenli C. Evidence for autosomal recessive inheritance of split hand/split foot malformation: A report of nine cases. Clin Dysmorphol. 2002;11:183–6. doi: 10.1097/00019605-200207000-00006. [DOI] [PubMed] [Google Scholar]
- 5.Ahmad M, Abbas H, Haque S, Flatz G. X-chromosomally inherited split-hand/split-foot anomaly in a Pakistani kindred. Hum Genet. 1987;75:169–73. doi: 10.1007/BF00591081. [DOI] [PubMed] [Google Scholar]
- 6.Winter RM, Baraitser M. The London dysmorphology database. J Med Genet. 1987;24:509–10. doi: 10.1136/jmg.24.8.509. [DOI] [PMC free article] [PubMed] [Google Scholar]