

Abstract
Background:
Professionalism is the core duty of a doctor to be responsible to the society. Doctors’ professionalism depicts an internalization of values and mastery of professionals’ standards as an important part in shaping the trust between doctors and patients. Professionalism consists of various attributes in which current literature focused more on the perspective of the health professionals. Doctors’ professionalism may influence patients’ satisfaction, and therefore, it is important to know from the patients’ perspectives what was expected of medical doctors’ professionalism.
Objective:
This study was conducted to determine the attributes of physician professionalism from the patient's perspective.
Materials and Methods:
This was a qualitative research using a phenomenology study design. In-depth interviews were conducted with 18 patients with hypertension and diabetes who had been treated for at least 1 year in primary care facilities in the city of Yogyakarta, Indonesia. The results of the interview were transcribed, encoded, and then classified into categories. Results: Communication skills were considered as the top priority of medical doctors’ attributes of professionalism in the perspectives of the patients.
Conclusion:
This study revealed that communication skill is the most important aspects of professionalism which greatly affected in the process of health care provided by the primary care doctors. Doctor-patient communication skills should be intensively trained during both basic and postgraduate medical education.
Keywords: Communication skills, primary care, professionalism
Introduction
Medical professionalism is the basis of social contract between medical profession and society.[1] This professionalism entails behavior professional as an observed conduct that describes the values and standards of the profession.[2] Good Medical Practice states that professional behavior of the medical profession should be developed as a responsibility to patients, colleagues, and society.[3]
The relationship between doctor and patient is a reflection of the professionalism and is the center of quality health care. Patients as part of society expect that doctors in charge have a high standard of professional behavior. A good doctor-patient relationship will increase patients’ perception to the doctor's competence.[4] Patients perceive communication skills and compassion as an important aspect of physician professionalism.[5]
Professionalism attributes that must be owned by a professional doctor are, among others, competence, respect, communication skills, altruism, and integrity.[6,7,8] These identified attributes require doctors to provide the best health services for patients as embodied in physician professionalism.[9] The services provided can start at the level of primary health care as the first sustainable health services, which are holistic and coordinated in nature. Primary care doctors are a doctor who is authorized to regulate health care and referral for patients according to their medical needs.[10]
In relation to the best health care services that must first be provided at the level of primary care facilities, most of the people of Indonesia are now members of the national health insurance system that requires them to primary care treatment prior to disease not in emergency cases.[11] Facts show that Indonesia as a country located in Asia has different cultures with countries located in Europe or other continents. This cultural difference sometimes leads to a different professional role.[12] Sari found five attributes of professionalism according to patient perception which is almost similar to attributes found in the literature.[13]
Discourse on medical doctors’ professionalism needs linking to its attributes regarding the level of healthcare facility. Concerning this issue, this study was conducted to determine the attributes medical doctors’ professionalism at primary care settings which are considered important by the patients.
Materials and Methods
This was a qualitative research using a phenomenology study design conducted in the city of Yogyakarta, Indonesia. The subjects were patients who had been treated routinely into a primary care facility in Yogyakarta for at least 1 year of a minimum of five times. The research subjects were taken with intensity sampling amounted to 18 people.
The data were collected by in-depth interviews to the study subjects using an interview guide that had been tried out previously. The interviews were conducted by an experienced interviewer (anthropologist) carried out at the subjects’ house by considering the convenience and time provided by the subjects of research. The interviews were recorded and later made transcripts.
The data were analyzed based on a phenomenology study. In the data analysis, the examples of behavior were encoded and then classified into categories. These were later grouped and then seen what themes that appeared in most of the research subject considered important by patients. The researchers used a low inference descriptor on the reporting of the results so that readers could interpret directly and give the interpretation of the study subjects’ experience.[14]
This study had been approved by the Research Ethics Committee of Universitas Gadjah Mada (Ref KE/PK/788/EC). Anonymity of research subjects was guaranteed by the researchers according to informed consent that had been signed by the research subjects.
Results
Eighteen people became the subjects in this study consisted of six men and 12 women aged 40–60 years. The research subjects graduated from elementary school to university. The research subjects in this study were those treated at five primary care facilities in the city of Yogyakarta, Indonesia.
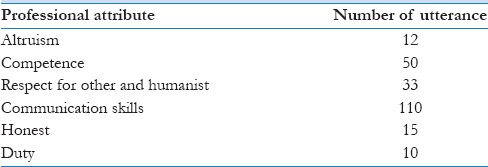
Based on data analysis, six themes were included in the examples of physician professional behavior or professionalism attributes as perceived by the patients. The identified attributes obtained in this research were altruism, competence, respect for other and humanist, communication skills, honesty, and duty [Table 1]. This is almost similar to attributes found in literature [Figure 1]. For the examples of professional behavior considered most important, the patients in this study chose the aspect of physician communication skills [Table 2].
Table 1.
Professional behavior attributes obtained from interview
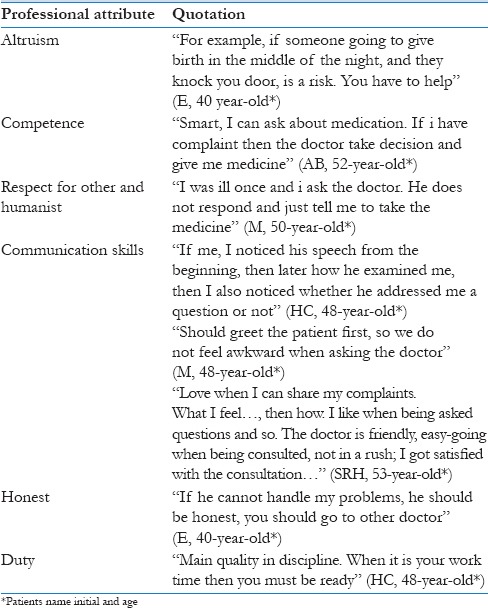
Figure 1.
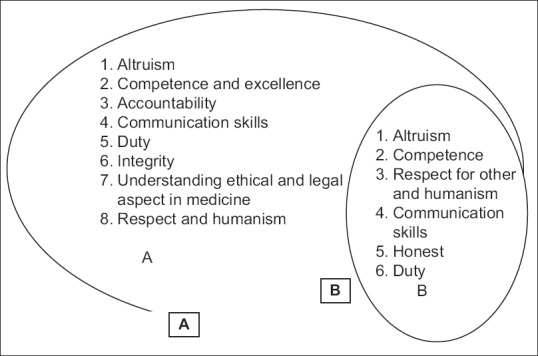
Relation between professional attributes in literature (A) and stated by patients (B)
Table 2.
Frequency of professional behavior attributes described by subjects of interview
The way doctor greet, speak and getting information from patient became the attention of the patients. Doctor who includes humor in consultation process was more preferable to the patient. Patients valued doctor who gave detailed information about their disease and management in the more friendly way and easy to understand. Nonverbal communication such as giving a smile, also part of communication skills that considered important to the patient.
Based on the results of the interviews, the patients could be assumed to see the professionalism of a doctor since they entered the examination room and how the doctors welcomed the patients. Communication during the consultation process was thus considered by the subjects in this study as the most important aspect when they sought treatment in primary care facilities.
Discussion
This study found that patients consider physicians’ communication skills as the most important part of the attributes of physicians’ professionalism. A good doctor-patient communication will give good impact on the health care provided to patients. Previous literature state that the ability of doctors to communicate effectively with patients is one aspect of physician professionalism.[6,7] In this study, communication skills revealed at the highest demand of the patients.
Communication with patients is an important clinical skill in medical practice. Doctor-patient communication skills are a specific task and behavior that can be observed. The skills observed consist of interviews to get a history of the disease, explaining the diagnosis and prognosis, providing treatment instruction, and providing counseling to motivate patients in therapy.[15] Clinical communication that occurs between doctors and patients is complex and individual factors can influence a doctor or medical student to master this skill.[16]
A good doctor-patient communication will influence the perception of patients to the physician. Communication problems between doctors and patients are found in the majority of patients that report malpractice complaints.[17] Doctor-patient communication starts since the patient enters the doctor's office. Therefore, a doctor who greets patients friendly when they enter the examination room is considered to have a good professional behavior. The expected communication is a type of communication in which the doctor not only thinks and responds to the patients in terms of disease but also understands and cares for the patient as an individual and their problems. Patients want to be treated with a friendly attitude and respected when having consultation sessions with doctors.[18]
Claramita et al.,[19] divides the process of doctor-patient communication in three stages, consisting of Greet, Invite, and Discuss. In the first stage, the doctor should establish a good relationship with the patients by greeting them and showing attention to the patients as an individual and at the same time positioning the doctors as if he/she is one of the patients’ family members by familial, friendly greetings such as: “Mother,” “father,” “so.” The second stage is that the doctor should be able to start a conversation with the patient. In Indonesian culture, there are still many patients who do not dare to express complaints when not asked by the doctor. Therefore, patients expect the doctor to begin a process of communication and ask to collect the patient's medical history; which all were expressed by mostly nonverbal communication. Patients want doctors to have good communication skills and show a sense of caring for patients.[20] The third stage is to discuss with the patient for the clinical decision-making. This is special for Indonesian culture because any clinical decision would be influenced by family or relatives’ preferences which often wins over patients’ preferences. Doctors; therefore, should maintain patients’ autonomy but still involving patients’ family (if the patient agrees).
At this point, the cultural background of the subject in this study is shifting from paternalistic into a more partnership communication. Doctors and patients have a role in determining the treatment process to be undergone by the patient. The principle of patient autonomy gives the right for patients to self-determine the therapeutic process that will be taken. In developed countries, patients have a greater role in determining health care for themselves.[21] Partnership communication is expected to occur between patient and doctor because, when it is inhibited, doctors will likely take more decisions for patients.[22] However, many factors sometimes cause a process of communication in medical practice not as expected. Differences in cultural characteristics will affect the way of communication between doctors and patients. Doctors in Indonesia still tend to use a more paternalistic communication styles with less contribution on patients’ site.[22]
Doctors working in primary care are expected to have good communication skills so that they can do optimal patient education and counseling process. Primary health care is the first level of health care facilities that prioritize promotive and preventive efforts to achieve high community health status. Patient education is one form of communication in the doctor-patient relationship.[23]
Primary care is very important to health service and has a great influence in the quality of care. Primary care is first contact, continuous, comprehensive, and integrated care provided to population.[10] Primary care physician uses the patient-centered clinical method in their practice.[24] They considered patient as a whole and not just to make a diagnosis. In medical practice, patient and doctor have their own agenda. Patients want to share their idea about the cause of their disease, and doctors want to make a diagnosis. Both patient and doctor have shared agenda in managing the disease. The patient sometimes has difficulty to tell their problem to doctors. It needs good communication skills from primary care physicians so they can work with patient to reach common ground on the definition of problems and patient management.[24,25]
Patient-physician relationship is important in primary care practice.[24] Primary care physicians have better understanding of their patient. In patient-centered practice, patients want to be “seen” and “heard” by their physician. Not just their sickness but also their personal issue.[26] To be able to do this role, primary care physician should have good communication skills.
Medical professionalism is the basis of a social contract between the medical profession and society; therefore, professionalism needs to be included in the curriculum of medical education. Indonesian Medical Council has drawn up a standard of competence that must be possessed by the graduates of the faculty of medicine in Indonesia. The standard is derived from the description of duties, role, and function of primary care doctors. Those standards have included the importance of professional behavior and communication skills as one of the aspects that should be included in the curriculum of medical education.[27] However, the core national curriculum should be implemented in more detail and strengthened with the primary care context, to be able to engage the medical students to the important of building trust with the patients by using proper communication skills.
The results of this research show the importance of communication skills as part of physician professional behavior. The results of this study are expected to provide feedback in learning professionalism in medical school about the importance of communication in a professional practice. We recommend that this study could be replicated in the wider scope of society, for example by doing a multicenter study across Asia.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Cruess SR. Professionalism and medicine's social contract with society. Clin Orthop Relat Res. 2006;449:170–6. doi: 10.1097/01.blo.0000229275.66570.97. [DOI] [PubMed] [Google Scholar]
- 2.van Luijk SJ, editor. Professional Behavior: Teaching, Assesing and Coaching Students. Maastricht: Universitaire Pers Maastricht; 2005. [Google Scholar]
- 3.General Medical Council and Medical School Council. Medical Students: Professional Behavior and Fitness to Practice, Guidance from the GMC and the MSC. [Last accessed on 2012 Nov 12]. Available from: http://www.gmc-uk.org/education/./professionalbehaviour.asp .
- 4.Moore PJ, Adler NE, Robertson PA. Medical malpractice: The effect of doctor-patient relations on medical patient perceptions and malpractice intentions. West J Med. 2000;173:244–50. doi: 10.1136/ewjm.173.4.244. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Wiggins MN, Coker K, Hicks EK. Patient perceptions of professionalism: Implications for residency education. Med Educ. 2009;43:28–33. doi: 10.1111/j.1365-2923.2008.03176.x. [DOI] [PubMed] [Google Scholar]
- 6.Flexner A. Is Social Work a Profession? New York: Cornell University Library; 1915. [Google Scholar]
- 7.Arnold L, Stern DT. What is medical professionalism. In: Stern DT, editor. Measuring Medical Professionalism. New York: Oxford University Press; 2006. [Google Scholar]
- 8.ABIM. Project Professionalism. American Board of Internal Medicine. 1995. [Last accessed on 2012 Nov 11]. Available from: http://www.abimfoundation.org/ResourceCenter/Bibliography/_/media/Files/Resource%20Center/Project%20professionalism.ashx .
- 9.Harms R. Physicians, professionalism and organizational efforts to improve quality - A systems perspective. WMJ. 2004;103:63–4. [PubMed] [Google Scholar]
- 10.Stanfiled B. Is primary care essential. Lancet. 1994;344:1129–33. doi: 10.1016/s0140-6736(94)90634-3. [DOI] [PubMed] [Google Scholar]
- 11.Indonesia Law No 24 Year 2011 about Social Security Administrator. 2012. [Last accessed on 2015 Nov 25]. Available from: http://www.publikasi.kominfo.go.id/handle/54323613/102. 2012 .
- 12.Cruess SR, Cruess RL, Steinert Y. Teaching professionalism across cultural and national borders: Lessons learned from an AMEE workshop. Med Teach. 2010;32:371–4. doi: 10.3109/01421591003692730. [DOI] [PubMed] [Google Scholar]
- 13.Sari MI. Patient Perception on Physician Professional Behaviour at Primary Care Facilities. A Master Thesis on Medical and Health Professional Education. Submitted to Graduate School of Universitas Gadjah Mada. 2015 [Google Scholar]
- 14.Johnson RB, Christensen LB. Educational Research: Quantitative, Qualitative, and Mixed Approaches. 3rd ed. Thousand Oaks: Sage; 2008. [Google Scholar]
- 15.Stern DT, Papadakis M. The developing physician - Becoming a professional. N Engl J Med. 2006;355:1794–9. doi: 10.1056/NEJMra054783. [DOI] [PubMed] [Google Scholar]
- 16.Noble L. Communication skills training: Pragmatism versus proof. Med Educ. 2002;36:108–9. doi: 10.1046/j.1365-2923.2002.01132.x. [DOI] [PubMed] [Google Scholar]
- 17.Beckman HB, Markakis KM, Suchman AL, Frankel RM. The doctor-patient relationship and malpractice. Lessons from plaintiff depositions. Arch Intern Med. 1994;154:1365–70. [PubMed] [Google Scholar]
- 18.Moore M. What does patient-centred communication mean in Nepal? Med Educ. 2008;42:18–26. doi: 10.1111/j.1365-2923.2007.02900.x. [DOI] [PubMed] [Google Scholar]
- 19.Claramita M, Susilo AP, Kharismayekti M, van Dalen J, van der Vleuten C. Introducing a partnership doctor-patient communication guide for teachers in the culturally hierarchical context of Indonesia. Educ Health (Abingdon) 2013;26:147–55. doi: 10.4103/1357-6283.125989. [DOI] [PubMed] [Google Scholar]
- 20.Porter KK, Rai G. Medical Ethics and the Elderly. 4th ed. Ch. 1. Abingdon, UK: Radcliffe Publishing Ltd; 2014. [Last accessed on 2015 Aug 27]. Principles of medical ethics. Available from: http://www.radcliffe.oxford.com/Books/samplechapter/pdf . [Google Scholar]
- 21.Claramita M, Utarini A, Soebono H, Van Dalen J, Van der Vleuten C. Doctor-patient communication in a Southeast Asian setting: The conflict between ideal and reality. Adv Health Sci Educ Theory Pract. 2011;16:69–80. doi: 10.1007/s10459-010-9242-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Passi V, Doug M, Peile E, Thistlethwaite J, Johnson N. Developing medical profesionalism in future doctors: A systematic review. Int J Med Educ. 2010;1:19–29. [Google Scholar]
- 23.Ministry of Health Regulation No 75 Year 2014 about Primary Care Service. 2014. [Last accessed on 2015 Nov 30]. Available from: http://depkes.go.id .
- 24.The College of Family Physician Canada. Four Principles of Family Medicine. The College of Family Physician Canada. [Last accessed on 2015 Nov 29]. Available from: http://www.cfpc.ca .
- 25.Goto M, Yokoya S, Takemura Y, Gayle AA, Tsuda T. Describing the factors that influence the process of making a shared-agenda in Japanese family physician consultations: A qualitative study. Asia Pac Fam Med. 2015;14:6. doi: 10.1186/s12930-015-0023-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Greenfield G, Ignatowicz AM, Belsi A, Pappas Y, Car J, Majeed A, et al. Wake up, wake up! It's me! It's my life! Patient narratives on person-centeredness in the integrated care context: A qualitative study. BMC Health Serv Res. 2014;14:619. doi: 10.1186/s12913-014-0619-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Indonesian Medical Council. Standards of Indonesian Medical Doctors Competencies. Jakarta: Indonesia Medical Council; 2012. [Google Scholar]