

Abstract
Aims:
The aims of this study were to determine fluoride concentration in drinking water and staple foods consumed by residents of Dayyer port (Bushehr province, south of Iran) and to assess its health risk via human intake in 2013.
Materials and Methods:
Health risk assessment due to fluoride exposure via consumption of drinking water, date, vegetables and fish was conducted in spring and summer of 2013 using the US-EPA (United States—Environmental Protection Agency) method, which considers hazard quotient (HQ) as a ratio of the estimated dose of a contaminant to the reference dose. A fluoride ion-selective electrode (ISE) measured the fluoride contents of food samples. The sodium-2-(parasulfophenyl largo)-1,8-dihydroxy-3,6-naphtnalene disulfonate colorimetric method (SPADNS) was used to determine fluoride concentration in water samples.
Results:
The total estimated oral intake of fluoride for children in summer and spring were 120.6 and 145.6 µg/kg/day, respectively. These values for adults were 99.2 and 112 µg/kg/day. This survey demonstrated that drinking water was the most important contributor of dietary fluoride intake in the study area.
Conclusion:
HQ values for adults and children were >1 which approves that a potential health risk of fluorosis can exist. The recommendations for the study area are supplying drinking water from alternative sources and defluoridation of drinking water by an adsorption technique and membrane filtration, respectively. Furthermore, people are suggested to have a good nutrition (especially rich of vitamin C) to reduce the risk of fluorosis.
Keywords: Drinking water, fluoride, risk assessment, staple food
INTRODUCTION
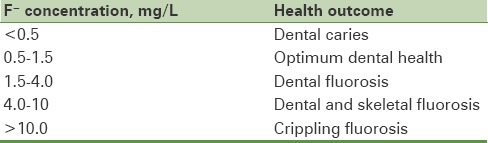
Fluoride is one of the very few micronutrients, which has been shown to cause profound effects on people through drinking water consumption or combination with exposure to fluoride from other sources.[1] Because of its strong electronegativity, fluoride is attracted by positively charged calcium in teeth and bones.[2] Fluoride at low concentration is an essential component for normal mineralization of bones and formation of dental enamel, but excessive exposure to fluoride can cause a number of adverse effects. These ranges varies from mild dental fluorosis that causes mottling and embrittlement of teeth to skeletal fluorosis that characterized by crippling as vary the level and period of exposure.[3] A guideline value of 1.5 mg/L was recommended by World Health Organization (WHO) as maximum permissible fluoride concentration level in drinking water.[4] Effects of fluoride exposure in different concentrations are summarized in Table 1.[5]
Table 1.
Effects of prolonged exposure to fluoride on public health
Globally, it has been reported that there are human population in countries such as Algeria,[6] China,[7,8] Egypt, Jordan,[9] India,[10,11,12,13] Iran,[14,15,16] Libya,[17] South Africa,[18,19] and Turkey[20] afflicted with fluorosis due to intake of fluoride-rich water and food.
Drinking water is the main source of fluoride intake by humans[15,20,21,22,23,24] but other sources of fluoride like some species of vegetables, fruits, fish, tea, cabbage, dental products,[20–31] vegetation growing in soils with high fluoride or irrigated with fluorinated water,[14] the sites in which the fertilizer and pesticides applied[32] and certain industrial processes contribute to the overall fluoride intake.[20]
Human health risk assessment (HHRA) is the identification, analysis, and characterization of potentially adverse health effects in humans from exposure to substances and agents in their environment.[33] Because of the wide effects of fluoride to public health, several research studies have performed risk assessment for fluoride exposure that mostly have studied the drinking water and beverages. In this study, the exposure pathways considered were either drinking water and very high consumed local foodstuffs including vegetables, date, and fish.[11,34,35,36,37,38,39,40]
Based on an estimation in the USA, food were composed a small part (6–33%) of total dietary fluoride intake in 4–6 years old children. However, a considerable effect of drinking water has been emphasized.[41]
Messaïtfa et al. observed that drinking water, tea, and date consist 70%, 20%, and 10% of daily intake of fluoride in the south of Algeria, respectively.[42] In a study conducted in the east Java, Indonesia, Heikens et al. reported that the lowest fluoride content in drinking water that poses a risk of fluorosis was about 0.5 mg/L for dental fluorosis and 1.1 mg/L for skeletal fluorosis that was below the guideline value (1.5 mg/L) suggested by WHO.[43]
According to several research studies, there are many regions in Iran, such as Borazjan,[44] Khormoj, Lar (south of Iran),[14] Maku (north west of Iran),[45] and Kuhbanan (central of Iran), which have come under threat of fluorosis.[46]
Dayyer port, located in south of Bushehr Province, Iran, is one of a typical endemic fluorosis areas caused by drinking water and foods for many years. In addition, symptoms of fluorosis are clear in residents of the study area. Ramezani et al.'s survey showed that prevalence of dental fluorosis in Dayyer is between 76% and 84.2%.[47]
As mentioned above, drinking water is the most important source of fluoride exposure, thus, estimation of optimum fluoride concentration in potable water of the study area is necessary.
The optimum amount of fluoride level in drinking water (D) is calculated according to the following equation:[48]
D (mg/L) = 0.34/[−0.038 + (0.0062 × Tm)],(Eq. 1)
where Tm is the maximum average temperature (in °F).
Regarding to an average annual temperature of 31.5°C (87.8 °F) for the study area,[49] the optimum fluoride content in drinking water should be 0.66 mg/L, which is lower than the maximum acceptable concentration in drinking water (1.5 mg/L) issued by WHO.[4]
A complete survey in order to determination of accurate exposure to all sources of fluoride is practically difficult, because the sources are variable. It is almost present in all foods at various contents, therefore a partial assessment is valuable as a guide for estimation of total intake and consequently for the assessment of health effects. In addition, there is no information on exposure to fluoride via consumption of drinking water and other sources of fluoride in Dayyer. Thus, in this study health risk assessment was employed to explain the effects of fluoride on the local resident's health due to fluoride exposure by ingestion of drinking water and staple food that include vegetables, date and fish.
The aims of this study were to estimate the daily fluoride intake for residents of Dayyer port by consumption of drinking water, date, vegetables and fish, and to evaluate fluorosis risk of the population groups using health risk assessment.
MATERIALS AND METHODS
Study area
Dayyer port is situated in the south west of Bushehr Province, south of Iran, between longitudes 50° 52′ and 51° 15′ and latitudes 27° 50′ and 28° 20′ with an area of ~2727 km2. The study area has a semi-arid to arid climate having a mean annual precipitation of about 270 mm. The maximum, minimum, and annually averages of temperature are 49.5, 8.29, and 31.5°C, respectively. The consumed drinking water is supplied from Kowthar dam in Kohgiluye and Boyerahmad province and groundwater from ten deep wells in the study area.
Date is a main product of the study area, similarly fish is a much consumable food appraised among residents. Consumption of drinking water in this region is much because of its arid and warm climatic conditions. Drinking water, date, and fish ingested by the residents may form a basis to establish an exposure of fluoride in order to perform a health risk assessment.
Sample collection and preparation
Water samples
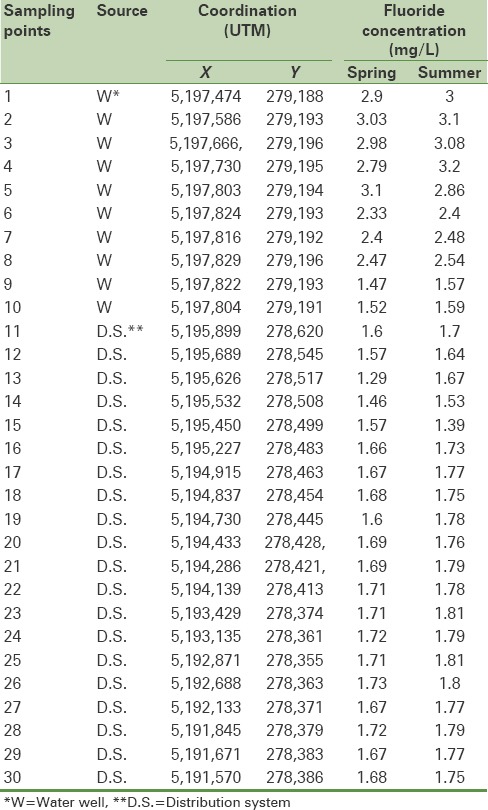
There are 10 operating water wells in this region that groundwater samples were collected from all of them. The rest of water samples were randomly collected from 20 locations of water distribution system with regard attention to their distance, during spring and summer seasons in 2013. These sampling points were first recorded using global positioning system (GPS) and reported in Universal Transverse Mercator (UTM) coordinates [Table 2]. The water samples were collected in 250 mL high-density polypropylene bottles (previously washed with distilled water and rinsed twice with the sampling water on the site).
Table 2.
Fluoride concentration in water samples
Vegetables, date, and fish samples
Vegetables including potato (Solanum tuberosum), onion (Allium cepa), leek (Allium porrum), tomato (Lycopersicumesculentum), sweet basil (Ocimum basilicum), mint (Mentha sativa), parsley (Petroselinum crispum), radish (Raphanussativus), and date were collected from the eight farms in the study area. Eight high-consumed fish samples also were collected from various points of Persian Gulf.
Analytical procedures
After sample collections, they were cleaned from dust and foreign material. Then, these samples were washed with tap water, followed by de-ionized water. After drying at 65°C to a constant weight, the samples were ground into powder, and passed through a 2-mm sieve. Then, the amount of fluoride was measured.
There are many methods for fluoride measurement in different substances, but the most applicable methods that Environmental Protection Agency (EPA) has approved are sodium 2-(parasulfophenyl largo)-1,8-dihydroxy-3,6 naphtnalene disulfonate (SPADNS) for water and ISE for food.[50]
The fluoride concentration in food samples was measured using a fluoride ISE (ISTEK neomet model 240 L ion meter, South Korea). In this regard, the NaOH fusion method was used because of its more extensive reading range, sensitivity, rapidity, and simplicity.[51] According to this method, NaOH 10 M was added to the samples in 25 mL nickel crucibles and placed inside a muffle furnace at 120°C for 1–3 h until completely drying and then fused at 600°C for 30 min. The residue was dissolved by heating with distilled water on a hot plate. The sample solutions were neutralized using concentrated HCl (37% purity) so that the pH of the solution was adjusted to 6. A 10-mL aliquot of each sample was mixed with an equal volume of total ionic strength buffer (TISAB). The buffer contains cyclo-hexylene-dinitrilo tetra acetic acid (CDTA), which forms stable complexes with Fe (III) and Al (III), thus preventing fluoride ions from complexes with these interferences. The obtained sample solutions were filtered and placed directly under the electrode.[52]
Fluoride
in water samples was analyzed by the SPADNS colorimetric method[52] using a DR-3900 spectrophotometer (HACH LANGE Company, UK). All chemical compounds and used reagents were purchased from Merck company and were of analytical grade.
The health risk assessment was determined by estimating the exposure doses of fluoride due to the consumption of drinking water, date, fish, and vegetables in terms of estimated daily intake (EDI) by following the generic equation (Equation 2):[36]
EDI = (C/BW) × IR, (Eq. 2)
BW: Body weight
EDI: Estimated daily intake
where EDI is the exposure daily intake (μg/kg/d); IR is the intake rate of water, date, fish, or vegetables (L/d, g/d and g/d), respectively; BW is the body weight (kg) that was assumed 70 kg for adults and 20 kg for children; and C is the concentration of fluoride (µg/L).[24]
The water intake for children in spring and summer was assumed 0.8 and 1 L.[49] These values for adults were 2.7 and 3 L, respectively. The date consumption was set to 200 g for adults and 100 g for children.[53] Intake rate of fish and vegetables are adapted from an integrated plan of nutritional condition of Bushehr Province.[54]
Various methods have been evolved to estimate the potential health risks of pollutants and to categorize the carcinogenic and non-carcinogenic effects. Non-carcinogenic risk assessments are usually based on the use of the HQ, which is defined as the ratio of the estimated dose of a contaminant to the reference dose (Eq. 3). This method is established by US-EPA at 1988.[55] Reference dose (RfD) is an estimation of daily exposure that is expected to be without significant risk of harmful effects during the lifetime. Its value in Integrated Risk Information System (IRIS) is 60 μg/kg/day, which comprises both the EDI from ingestion of fluoride through drinking water (50 μg/kg/day) and dietary intake of fluoride (10 μg/kg/day).[24]
HQ = EDI/RfD (Eq. 3)
When the HQ is greater than 1, the estimated potential exposure exceeds the RfD and a risk of fluorosis may be posed.[55]
RESULTS
Table 2 shows fluoride concentration in drinking water samples. As can be seen in this table, the highest concentration of fluoride (3.1 mg/L) was related to ground water samples in summer 2013; however, the lowest concentration of that (1.29 mg/L) was correlated to distribution system samples in spring 2013. In about 90% of the water samples analyzed in spring and 96.7% of those analyzed in summer, the fluoride content was higher than WHO guidelines (1.5 mg/L). In addition, the mean concentration of fluoride in drinking water was higher in summer (2.013 mg/L) than in spring (1.9 mg/L).
In Table 3, fluoride amount and its exposure dose, in common vegetables, date, and fish are presented. On the basis of these data, sweet basil with 7040 µg F-/kg and onion with 1100 µg F-/kg had maximum and minimum fluoride concentration and consequently the EDI level in vegetables, respectively.
Table 3.
Fluoride concentration and exposure dose of fluoride in vegetables, date, and fish samples
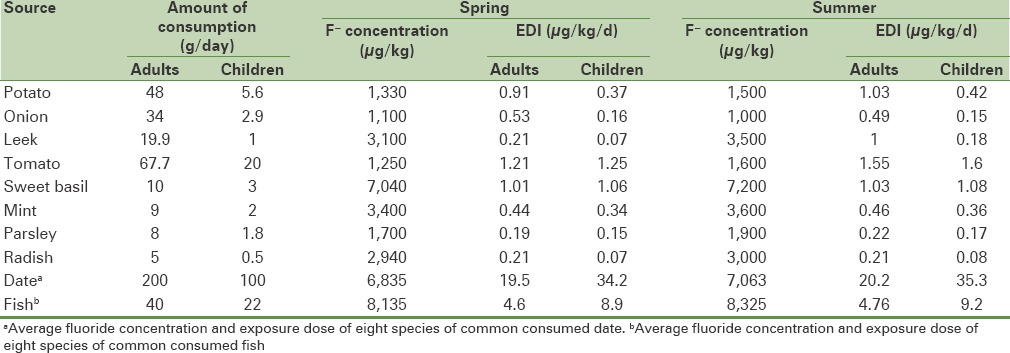
Table 4: Shows the total exposure dose of fluoride and its HQ index. As mentioned previously, reference dose for fluoride exposure in this study is 60 μg/kg/d.
Table 4.
Total exposure dose and HQ index
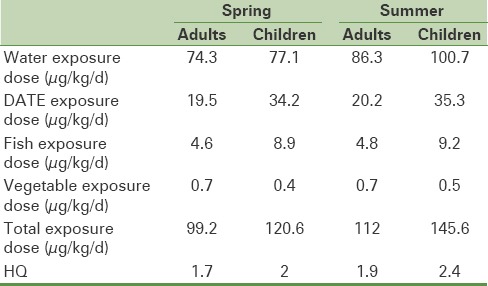
Figure 1a and b shows contribution percentage of each source in total fluoride intake for children and adults. According to these figures, drinking water is the major contributor of fluoride ingestion, both in adults and children.
Figure 1.

Contribution percentage of the studied sources in total fluoride intake (a) for adults and (b) for children
DISCUSSION
In this study, 60 drinking water samples were analyzed for fluoride concentrations within two warm and cold season [Table 2]. The fluoride concentrations were varied from 1.29 to 3.1 and 1.39 to 3.2 mg/L in spring and summer, respectively. Groundwater samples exhibit higher fluoride content compared with distribution system samples. It may be due to reactions of water with minerals in rock and soil which groundwater comes into contact. In an investigation carried out by Mesdaghinia et al., the high fluoride content of groundwater in Bushehr Province was confirmed.[15] One-sample T-test also showed that there was significant difference between the fluoride concentrations in water supply system by the WHO guideline value.[4] In this study, one-way analysis of variance (ANOVA) showed that there was no seasonal significant difference in groundwater fluoride concentrations (P = 0.759), while the difference between water distribution system samples were significant with respect to fluoride concentrations (P = 0.011), whereas the mean fluoride level in water distribution system in summer was higher than spring that maybe due to more water withdrawal of groundwater in summer. Unlike this result, Chavoshi et al. found that due to more precipitation in spring, fluoride content of water was lower in summer, when water was discharged for irrigation. She claimed that the lower fluoride content of groundwater in summer than spring was also probably because of the formation of insoluble fluorite.[14]
Based on Table 3, date has the most fluoride concentration and exposure dose in all of the food samples. Battaleb et al. reported high fluoride concentration in date samples due to pH of 8.5 for soil, which means that fluoride is available for absorption by the plant.[53]
EDI through consumption of date and fish in children was higher than adults. As mentioned in Eq. (2), for EDI calculation, average body weight for children was considered 20 kg, while its value for adults was 70 kg. In all of the food samples, except onion, fluoride concentration and consequently EDI in summer were higher than spring [Table 3]. The most concentration of fluoride among vegetables belonged to sweet basil. However, Jha et al. in 2011 concluded that spinach had maximum content of fluoride and maximum EDI between their studied vegetables.[36] In this study, the fluoride amount of fish samples was higher in summer. It may be due to higher fluoride concentration of seawater, where the fish in this study were harvested in summer (82 mg/L) than spring (73 mg/L).
The results of Table 4 reveal that the daily fluoride intake from drinking water varies with the season, from 74.3 and 77 μg/kg/day in spring to 86.3 and 100.7 μg/kg/day in summer for adults and children, respectively. In attention to the amount of water consumption that was considered to be 2.7 and 0.8 L in spring, and 3 and 1 L in summer for adults and children, respectively, it can be mentioned that as temperature of ambient air increased, water consumption and consequently fluoride intake from drinking water were increased. These results are in agreement with previous investigations such as Zohouri's findings, which showed that the average fluoride intake was much higher in summer than in winter, mainly because of the higher consumption of water in summer.[56]
The HQ values of fluoride for the two age groups are listed in Table 4, which is 1.7 and 2 times greater than 1 in spring, and 1.9, and 2.4 in summer for adults and children, respectively. Similar findings were also reported by Jha et al., which demonstrated that HQ from fluoride exposure through ingestion of vegetables and cereal crops in children (3–14 years) in brick kiln area and sodic areas in Unnao district, Uttar Pradesh, India was 1.37 and 1.08, respectively.[36]
Assessment of health risks associated with fluoride concentration in drinking water in China revealed that the HQ of this area was >1 for 68% of the total residents of west plain region in Jilin Province, China.[21] In another study, HQ values through consumption of drinking water and date were 1.6 and 3.4 for adults and children, respectively.[53]
HQ values of present research indicated that health risks associated with fluoride exposure for children and adults are significant only from drinking water, date, vegetables, and fish consumption and a potential risk of dental fluorosis would be exist.
Figure 1a and 1b display contribution percentage of each source in total fluoride intake. As can be seen, ~76% and 67% of the total fluoride intake for adults and children, respectively, is derived from drinking water. This proportion increased with increasing drinking water consumption due to climate temperature and raising fluoride content of water.
According to these charts, as the temperature goes higher, role of drinking water in total fluoride intake increases. In agreement with this result, Battaleb-Looie in 2013 observed that about 63% of dietary fluoride intake derived from drinking water.[53]
In addition, fluoride intake from drinking water, vegetables, meal, and air in Jilin Province, China, was accounted 90.55%, 4.69%, 3.7% and 1.06% of the total fluoride intake, respectively.[21] According to the findings of Chavoshi et al., drinking water was the principal source of fluoride ingestion.[14] Therefore, this survey showed that in the study area, drinking water was the main contributor of fluoride ingested by the population.
CONCLUSIONS
The performed health risk assessment through the consumption of drinking water, date, common vegetables, and fish based on estimated HQ revealed that the total HQ values were greater than 1 for both adults and children, so the local residents of the study area was at a high risk of fluorosis due to excessive fluoride ingestion.
Drinking water was the main source of fluoride intake in the study area. Therefore for decrease of fluorosis prevalence, it is recommended as the first option that drinking water be supplied from low fluoride content alternative sources. While alternative sources are not available, a prior treatment in order to de-fluoridation of drinking water with readily applicable technologies such as adsorption using activated alumina and membrane filtration (reverse osmosis and electrodialysis) is the other solution that is suggested. Furthermore, people are advised to have a good nutrition (rich of calcium, vitamins especially vitamin C, and proteins) to reduce the risk of fluorosis. The children are more susceptible to excess fluoride intake than adults. Thus, they also advised to avoid use of toothpaste and items that contain fluoride.
Financial support and sponsorship
Isfahan University of Medical Sciences, Isfahan, Iran.
Conflicts of interest
There are no conflicts of interest.
Acknowledgement
This article is the result of MSc approved thesis of Mrs Somayye Keshavarz, research project #391309, in Isfahan University of Medical Sciences (IUMS). Thus, the authors are thankful for the funding provided by the department of environmental health engineering and environment research center, IUMS.
REFERENCES
- 1.Fawell JK. Geneva: World Health Organization; 2006. Fluoride in drinking-water. [Google Scholar]
- 2.Hussain I, Arif M, Hussain J. Fluoride contamination in drinking water in rural habitations of Central Rajasthan, India. Environ Monit Assess. 2012;184:5151–8. doi: 10.1007/s10661-011-2329-7. [DOI] [PubMed] [Google Scholar]
- 3.Arveti N, Sarma M, Aitkenhead-Peterson J, Sunil K. Fluoride incidence in groundwater: A case study from Talupula, Andhra Pradesh, India. Environ Monit Assess. 2011;172:427–43. doi: 10.1007/s10661-010-1345-3. [DOI] [PubMed] [Google Scholar]
- 4.Vol. 1. Geneva: World Health Organization; 2006. WHO. Guidelines for drinking-water quality: Recommendations. [Google Scholar]
- 5.Mohapatra M, Anand S, Mishra B, Giles DE, Singh P. Review of fluoride removal from drinking water. J Environ Manage. 2009;91:67–77. doi: 10.1016/j.jenvman.2009.08.015. [DOI] [PubMed] [Google Scholar]
- 6.Susheela A, Mudgal A, Keast G. Fluoride in water: An overview. Water front. 1999:11–13. [Google Scholar]
- 7.Xiang Q, Liang Y, Chen L, Wang C, Chen B, Chen X, Zhou M. Effect of fluoride in drinking water on children's intelligence. Fluoride. 2003;36:84–94. [Google Scholar]
- 8.Wang B, Zheng B, Zhai C, Yu G, Liu X. Relationship between fluorine in drinking water and dental health of residents in some large cities in China. Environ Int. 2004;30:1067–73. doi: 10.1016/j.envint.2004.05.006. [DOI] [PubMed] [Google Scholar]
- 9.Barot V. Occurrence of endemic fluorosis in human population of North Gujarat, India: Human health risk. Bull Environ Contam Toxicol. 1998;61:303–10. doi: 10.1007/s001289900763. [DOI] [PubMed] [Google Scholar]
- 10.Maheshwari R. Fluoride in drinking water and its removal. J Hazard Mater. 2006;137:456–63. doi: 10.1016/j.jhazmat.2006.02.024. [DOI] [PubMed] [Google Scholar]
- 11.Garg V, Malik A. Groundwater quality in some villages of Haryana, India: Focus on fluoride and fluorosis. J Hazard Mater. 2004;106:85–97. doi: 10.1016/j.jhazmat.2003.09.007. [DOI] [PubMed] [Google Scholar]
- 12.Kundu N, Panigrahi M, Tripathy S, Munshi S, Powell M, Hart B. Geochemical appraisal of fluoride contamination of groundwater in the Nayagarh District of Orissa, India. Environ Geol. 2001;41:451–60. [Google Scholar]
- 13.Ramanaiah S, Mohan SV, Rajkumar B, Sarma P. Monitoring of fluoride concentration in ground water of Prakasham district in India: Correlation with physico-chemical parameters. J Environ Sci Eng. 2006;48:129–34. [PubMed] [Google Scholar]
- 14.Chavoshi E, Afyuni M, Hajabbasi M, Khoshgoftarmanesh A, Abbaspour K, Shariatmadari H, et al. Health risk assessment of fluoride exposure in soil, plants, and water at Isfahan, Iran. Hum Ecol Risk Assess. 2011;17:414–30. [Google Scholar]
- 15.Mesdaghinia A, Vaghefi KA, Montazeri A, Mohebbi MR, Saeedi R. Monitoring of fluoride in groundwater resources of Iran. Bull Environ Contam Toxicol. 2010;84:432–7. doi: 10.1007/s00128-010-9950-y. [DOI] [PubMed] [Google Scholar]
- 16.Nouri J, Mahvi AH, Babaei A, Ahmadpour E. Regional pattern distribution of groundwater fluoride in the Shush aquifer of Khuzestan County, Iran. Fluoride. 2006;39:321. [Google Scholar]
- 17.Sunil Tejaswi K, Shetty S, Annapoorna B, Pujari SC, Reddy S, Nandlal B. A Pioneering Study of Dental Fluorosis in the Libyan Population. J Int Oral Health. 2013;5:67–72. [PMC free article] [PubMed] [Google Scholar]
- 18.Ncube E, Schutte C. The occurrence of fluoride in South African groundwater: A water quality and health problem. Water SA. 2005;31:35–40. [Google Scholar]
- 19.Srikanth R, Viswanatham K, Kahsai F, Fisahatsion A, Asmellash M. Fluoride in groundwater in selected villages in Eritrea (North East Africa) Environ Monit Assess. 2002;75:169–77. doi: 10.1023/a:1014491915537. [DOI] [PubMed] [Google Scholar]
- 20.Oruc N. Occurrence and problems of high fluoride waters in Turkey: An overview. Environ Geochem Health. 2008;30:315–23. doi: 10.1007/s10653-008-9160-2. [DOI] [PubMed] [Google Scholar]
- 21.Bo Z, Mei H, Yongsheng Z, Xueyu L, Xuelin Z, Jun D. Distribution and risk assessment of fluoride in drinking water in the west plain region of Jilin province, China. Environ Geochem Health. 2003;25:421–31. doi: 10.1023/b:egah.0000004560.47697.91. [DOI] [PubMed] [Google Scholar]
- 22.Edmunds WM, Smedley PL. New York: Springer; 2013. Fluoride in natural waters. Essentials of medical geology; pp. 311–6. [Google Scholar]
- 23.Jha S, Nayak A, Sharma Y. Fluoride occurrence and assessment of exposure dose of fluoride in shallow aquifers of Makur, Unnao district Uttar Pradesh, India. Environ Monit Assess. 2009;156:561–6. doi: 10.1007/s10661-008-0505-1. [DOI] [PubMed] [Google Scholar]
- 24.Perumal E, Paul V, Govindarajan V, Panneerselvam L. A brief review on experimental fluorosis. Toxicol Lett. 2013;223:236–51. doi: 10.1016/j.toxlet.2013.09.005. [DOI] [PubMed] [Google Scholar]
- 25.Haftenberger M, Viergutz G, Neumeister V, Hetzer G. Total fluoride intake and urinary excretion in German children aged 3–6 years. Caries Res. 2001;35:451–7. doi: 10.1159/000047489. [DOI] [PubMed] [Google Scholar]
- 26.Jackson RD, Brizendine EJ, Kelly SA, Hinesley R, Stookey GK, Dunipace AJ. The fluoride content of foods and beverages from negligibly and optimally fluoridated communities. Community Dent Oral Epidemiol. 2002;30:382–91. doi: 10.1034/j.1600-0528.2002.00002.x. [DOI] [PubMed] [Google Scholar]
- 27.Maguire A, Zohouri FV, Hindmarch PN, Hatts J, Moynihan PJ. excretion in 6-to 7-year-old children living in optimally, sub-optimally and non-fluoridated areas. Community Dent Oral Epidemiol. 2007;35:479–88. doi: 10.1111/j.1600-0528.2006.00366.x. [DOI] [PubMed] [Google Scholar]
- 28.Mahvi AH, Zazoli MA, Younecian M, Esfandiari Y. Fluoride content of Iranian black tea and tea liquor. Fluoride. 2006;39:266. [Google Scholar]
- 29.Martínez-Mier E, Soto-Rojas AE, Ureña-Cirett JL, Stookey GK, Dunipace AJ. Fluoride intake from foods, beverages and dentifrice by children in Mexico. Community Dent Oral Epidemiol. 2003;31:221–30. doi: 10.1034/j.1600-0528.2003.00043.x. [DOI] [PubMed] [Google Scholar]
- 30.Zohouri FV, Maguire A, Moynihan PJ. Sources of Dietary Fluoride Intake in 6–7-Year-Old English Children Receiving Optimally, Sub-optimally, and Non-fluoridated water. J Public Health Dent. 2006;66:227–34. doi: 10.1111/j.1752-7325.2006.tb04074.x. [DOI] [PubMed] [Google Scholar]
- 31.Kramer L, Osis D, Wiatrowski E, Spencer H. Dietary fluoride in different areas in the United States. Am J Clin Nutr. 1974;27:590–4. doi: 10.1093/ajcn/27.6.590. [DOI] [PubMed] [Google Scholar]
- 32.Myers HM. Fluorides and dental fluorosis. Monogr Oral Sci. 1978;7:1. [PubMed] [Google Scholar]
- 33.Patterson J, Hakkinen PJ, Wullenweber AE. Human health risk assessment: Selected internet and world wide web resources. Toxicology. 2002;173:123–43. doi: 10.1016/s0300-483x(02)00027-6. [DOI] [PubMed] [Google Scholar]
- 34.Erdal S, Buchanan SN. A quantitative look at fluorosis, fluoride exposure, and intake in children using a health risk assessment approach. Environ Health Perspect. 2005;113:111–7. doi: 10.1289/ehp.7077. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Ghojazadeh M, Azar FP, Naghavi-Behzad M, Mahmoudi M, Azami-Aghdash S, Jamali Z. Fluoride Concentration of Drinking Waters and Prevalence of Fluorosis in Iran: A Systematic Review. J Dent Res Dent Clin Dent Prospects. 2013;7:1–7. doi: 10.5681/joddd.2013.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Jha S, Nayak A, Sharma Y. Site specific toxicological risk from fluoride exposure through ingestion of vegetables and cereal crops in Unnao district, Uttar Pradesh, India. Ecotoxicol Environ Saf. 2011;74:940–6. doi: 10.1016/j.ecoenv.2011.01.002. [DOI] [PubMed] [Google Scholar]
- 37.Shyam R, Kalwania G. Health risk assessment of fluoride with other parameters in ground water of Sikar city (India) Environ Earth Sci. 2012;65:1275–82. [Google Scholar]
- 38.Zabin SA, Foaad M, Al-Ghamdi AY. Non-carcinogenic risk assessment of heavy metals and fluoride in some water wells in the Al-Baha Region, Saudi Arabia. Hum Ecol Risk Assess. 2008;14:1306–17. [Google Scholar]
- 39.Battaleb-Looie S, Moore F, Jacks G, Ketabdari MR. Geological sources of fluoride and acceptable intake of fluoride in an endemic fluorosis area, southern Iran. Environ Geochem Health. 2012;34:641–50. doi: 10.1007/s10653-012-9451-5. [DOI] [PubMed] [Google Scholar]
- 40.Waziri M, Musa U, Stephen S, Hati Assessment of Fluoride Concentrations in Surface Waters and Groundwater Sources in Northeastern Nigeria. Resour Enviro. 2012;2:67–72. [Google Scholar]
- 41.McClure F. Fluorine in foods. Public Health Rep. 1949;64:l061–74. [PMC free article] [PubMed] [Google Scholar]
- 42.Messaïtfa A. Fluoride contents in groundwaters and the main consumed foods (dates and tea) in Southern Algeria region. Environ Geol. 2008;55:377–83. [Google Scholar]
- 43.Heikens A, Sumarti S, Van Bergen M, Widianarko B, Fokkert L, Van Leeuwen K, et al. The impact of the hyperacid Ijen Crater Lake: Risks of excess fluoride to human health. Sci Total Environ. 2005;346:56–69. doi: 10.1016/j.scitotenv.2004.12.007. [DOI] [PubMed] [Google Scholar]
- 44.Dobaradaran S, Mahvi AH, Dehdashti S, Abadi DRV, Tehran I. Drinking water fluoride and child dental caries in Dashtestan, Iran. Fluoride. 2008;41:220–6. [Google Scholar]
- 45.Moghaddam AA, Fijani E. Distribution of fluoride in groundwater of Maku area, northwest of Iran. Environ Geol. 2008;56:281–7. [Google Scholar]
- 46.Poureslami HR, Khazaeli P, Nooric GR. Fluoride in food and water consumed in Koohbanan (Kuh-e Banan), Iran. Fluoride. 2008;41:216–9. [Google Scholar]
- 47.Ramezani Gh, Valaei N, Eikani H. Prevalence of DMFT and fluorosis in the students of Dayer city (Iran) J Indian Soc Pedo Prev Dent. 2004;22:49–53. [PubMed] [Google Scholar]
- 48.Galagan DJ, Vermillion JR. Determining optimum fluoride concentrations. Public health Rep. 1957;72:491–3. [PMC free article] [PubMed] [Google Scholar]
- 49. [Last accessed on 2014 May 29]. Available from: http://www.waterintakecalculator.com/Index.html.water intake calculator.MGD .
- 50.Chambers RD. United States: CRC Press; 2004. Fluorine in organic chemistry. [Google Scholar]
- 51.Malde MK, Maage A, Macha E, Julshamn K, Bjorvatn K. Fluoride content in selected food items from five areas in East Africa. J Food Compost Anal. 1997;10:233–45. [Google Scholar]
- 52.Eaton AD, Franson MA. Washington, DC: American Public Health Association; 2005. Standard methods for the examination of water and wastewater. [Google Scholar]
- 53.Battaleb-Looie S, Moore F, Malde M, Jacks G. Fluoride in groundwater, dates and wheat: Estimated exposure dose in the population of Bushehr. Iran J Food Compost Anal. 2013;29:94–9. [Google Scholar]
- 54.Kalantari N, Ghaffarpour M, Kianfar H, Hooshiarrad A, Bandaarianzade D, Abdollahi M, et al. Tehran: National Nutrition and Food Technology Research Institute; 2001. Integrated plan of nutritional condition of Bushehr province. [Google Scholar]
- 55.Barnes DG, Dourson M, Preuss P, Bellin J, Derosa C, Engler R, et al. Reference dose (RfD): Description and use in health risk assessments. Regul Toxicol Pharmacol. 1988;8:471–86. doi: 10.1016/0273-2300(88)90047-5. [DOI] [PubMed] [Google Scholar]
- 56.Zohouri FV, Rugg-Gunn AJ. Sources of dietary fluoride intake in 4-year-old children residing in low, medium and high fluoride areas in Iran. Int J Food Sci Nutr. 2000;51:317–26. doi: 10.1080/096374800426911. [DOI] [PubMed] [Google Scholar]