

Abstract
Background:
Adolescence is associated with so many changes, and to provide sexual health it is necessary for teenagers to learn enough knowledge about the changes and appropriate health behaviors. The attraction of sexual issues in teenagers is associated with more conversations related to sexual matters. Therefore, this study has evaluated the effect of organizing these interactions using peer education in schools on the knowledge and attitude toward sexual health.
Materials and Methods:
This was an interventional study conducted on 282 girl teenagers from high schools of Isfahan that were divided into two groups of intervention and control. Peer education in the intervention group was done through 35 trained teenagers during normal communications in school. Before the training knowledge and attitude of students in both groups were evaluated; then peer education was conducted during 6 weeks through normal communications on the intervention group and then afterward the knowledge and attitude of the students were evaluated again. To analysis of data independent t-test and paired t-test were used.
Results:
The results showed that the mean score of knowledge and attitudetoward all sexual health dimensions during puberty in the intervention group was significantly higher after the intervention (P < 0.05). In addition, there was a significant difference between the mean score of knowledge and approach toward all the aspects of sexual health of both the studied groups.
Conclusions:
The results showed that using peer education in schools informally could enhance the knowledge and approach toward aspects of physical health, sexual behaviors, and social and mental changes among female adolescences and could be applied in schools.
Keywords: Adolescences, peer education, sexual health
INTRODUCTION
Adolescence is the time to gain individual identity and emerge sexual excitement along with rapid physical, mental, and emotional changes.[1] Puberty and sex appeal would cause teenagers to be more sensitive toward sexual subjects; therefore, they would try to find answers for their questions. The media, as a one-way informant, has also engaged teenagers’ minds with sexual matters[2] and stimulates sexual behaviors. On the other hand, the spread of sexually transmitted diseases among young adults[3,4] could indicate lack of knowledge about risky sexual behaviors among this vulnerable population.[5,6]
Therefore, due to its importance in enhancing public health and country's social and economic growth, the necessity of sexual trainings has been proposed and confirmed as an independent subject at the international conference on population and growth in Cairo in 1994 and it has developed ever since.[7,8] Although sexual trainings for teenagers, especially girls, is one of the most important educational matters that could have direct effect on long-term health enhancement and developmental programs,[9] but parents feel ashamed to train sexual matters to their children and do not have appropriate skills for these trainings.[10] Therefore presenting sexual training programs with regard to the context of social values and taking advantage of right opportunities, based on teenagers’ desires, is necessary.
One of the special characteristics of teenagers is their tendency toward their own peers that would develop conformance and consistency among them; this has made the peers the most important informant group for teenagers.[11,12,13] Although gaining information about sexual matters in puberty could be a threat to teenagers’ sexual health but using the right context could make it an opportunity to provide teenagers with right educational information. Therefore, the presence of educated peers in an official educational course could be used for unofficially distributing the appropriate educational content among their uneducated peers to enhance the sexual health of teenagers.
Although studies have shown that the training with peers approach could be successful in enhancing health issues among different age groups,[14,15,16,17,18] but channelizing teenagers’ conversation toward sexual matters has its own complexities that could affect educational interventions. Because although teenagers are highly conformance with each other,[19] but they necessary do not receive all of their information from people who has been officially trained in these matters. Especially the effect of these interventions on the knowledge and approach of teenagers in different social-cultural contexts could lead to different results.
In this regard, studies have shown that using peer-based trainings have increased the knowledge and enhanced the preventive behaviors about HIV and sexually transmitted diseases (STDs) among teenage girls.[16,20,21] However, the effect of this kind of trainings about sexual matters at the school level has not been evaluated before. On the basis of the school programs in Iran, students spend a little time outside classrooms with each other and the opportunity is limited for trainers compared with peers communications outside the school. Also the members of peers groups are fewer among girls than boys that could affect the opportunities for applying this method. Therefore, the effect of this approach at the school level and by trained peers on the knowledge and approach of teenagers toward sexual matters has been set as the aim of this study.
MATERIALS AND METHODS
This was an interventional study conducted on teenager students of female high schools of Isfahan from October 2013 to February 2014. The ethical committee of Isfahan University of Medical Sciences has approved this study. A total of 282 female teenager aged from 14 to 18 were participated in this study and were divided into three groups of trainers, trainees, and control. The trainers group consisted of teenagers who received official sexual educations and trained the trainees group unofficially at appropriate opportunities in school.
The control group consisted of teenagers who received no unofficial education. The inclusion criterion for the trainees and control group was not having any mental diseases based on their school profile and the exclusion criteria were missing school for more than a week during the unofficial trainings and occurrence of accidents that could affect their learning ability.
The selection of trainers was targeted. The inclusion criterion was gaining the score of at least 80% in the checklist based on library studies and viewpoint of experienced people and it included moral authority, being loved by other students, the ability to communicate with others properly, and not having a history of violation, anti-social behaviors, and also having high learning abilities. This checklist was selected by school authorities and through interview. The exclusion criteria for this group was missing educational sessions, missing school during the unofficial trainings, and not gaining the threshold score at the end of the course.
The measurement tool for the level of knowledge in different aspects was a researcher made questionnaire included 54 questions which evaluated knowledge in physical, sexual health behaviors, and mental social domains. Questions were compiled as multiple-choice questions and true–false questions and its highest score was 96. Multiple-choice questions had no negative effect. Furthermore, the approach was evaluated using a researcher made questionnaire with 64 questions that was designed based on the Likert scale (0–4). These questionnaires were filled by the participants in at most 50 min. This questionnaire was a researcher made tool that was designed based on scientific studies and its content and figure validity was confirmed by five experts and its reliability was confirmed through a pilot study with a two-week interval gaining a Cronbach's α of 0.82.
Through the list of Isfahan's high schools two schools were randomly selected as the intervention center and two were selected as the control center. For selecting the trainers and the control group from each of the four schools five classes from all the grades were selected randomly and by the students’ list and the number of students in each class, 282 students were selected using simple random selection through the table of random numbers. From the same classes 35 students were selected as the trainers (one trainer for every four trainee). All of the participants of all groups and their parents filled written consent form.
The official training of the trainers group was done in three 90-min sessions. They were instructed by a midwife and a consultant that were totally acquainted with the purpose of the study and required educational content in a meeting. The presented educational content included the anatomy and function of the reproductive system, physical changes and health during puberty, mental changes through puberty, risky sexual behaviors and their consequences, and preventive behaviors for sexual diseases. At the end of the official sessions, scientific qualifications of the trainers group were evaluated through a test and gaining at least 90% of the possible score.
The demographic data, knowledge and approach of teenagers of the trainers, and the control groups were evaluated. At the schools that were the control center, routine trainings were provided by the school consultant. In the interventional schools, unofficial trainings were provided by the trainers group for 6 weeks. The trainees were not aware of the trainers’ identities. After 6 weeks both of the trainees group and the control group filled the questionnaire for evaluating knowledge and approach toward sexual health. The mean scores of knowledge and approach toward sexual health were compared in domains of physical health, healthy sexual behaviors, and social mental changes during puberty. Data were analyzed with SPSS 16 using independent t-test, paired t-test, Chi square, and Mann–Whitney. The significance level for tests was set at P < 0.05.
RESULTS
A total of 282 teenagers participated in the study. The mean age of the intervention group was 15.8 ± 1.1 years and the mean age of the control group was 15.6 ± 1.1 years. At the first stage, 282 questionnaires were distributed to and filled by participants. At the second stage, 263 questionnaires were completed. Five students due to missing school, one due to transfer to another school, and nine for not completing the questionnaire were excluded from the control group and four students were excluded from the intervention group for missing school.
Table 1 shows the comparison between demographic data of both groups. The results showed that the trainers group and the control group had no significant differences in their demographic data. Comparing the mean score of overall knowledge (t = 1.10, P = 0.27) and aspects of physical health (t = 0.96, P = 0.34), healthy behaviors (t = 0.94, P = 0.35) and social mental changes (t = 0.82, P = 0.41) between both groups before the trainings showed no significant differences [Table 2]. Also both groups had no significant differences in the mean score of overall approach (t = 1.002, P = 0.31), approach toward aspects of physical health (t = 1.02, P = 0.31), healthy sexual behaviors (t = 0.79, P = 0.43), and social mental changes (t = 0.43, P = 0.67) [Table 3].
Table 1.
Comparison of individuals’ characterizes between groups
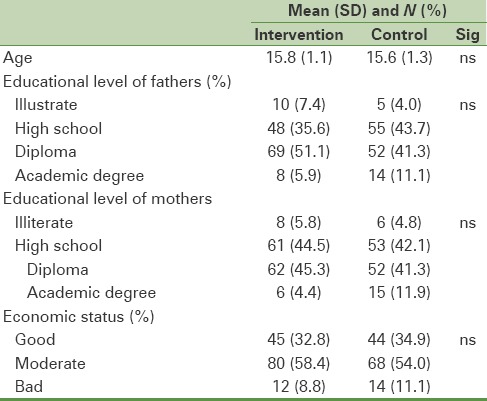
Table 2.
Comparison of knowledge before and after intervention
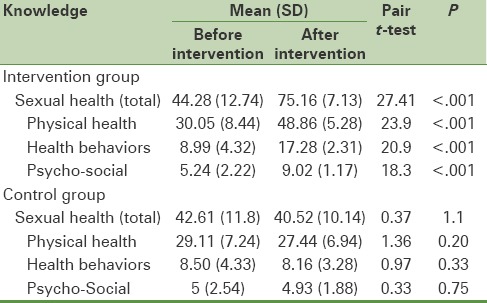
Table 3.
Comparison of attitude before and after intervention
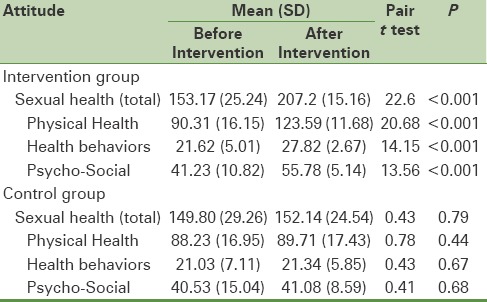
The results showed that the scores of knowledge and approach were improved in the intervention group after the trainings; but the control group showed no significant difference after the trainings in this regard [Tables 2 and 3].
The score of knowledge about physical health (t = 28.29, P = 0.001), healthy sexual behaviors (t = 26.16, P = 0.001), and social mental changes (t = 21.28, P = 0.001) in both the trainees group and the control group had a significant difference after trainings. Also there was a significant difference between the mean score of approach toward physical health (t = 18.64, P = 0.001), healthy sexual behaviors (t = 11.7, P = 0.001), and social mental changes (t = 16.98, P = 0.001) of both groups.
DISCUSSION
The importance of enhancing sexual health of teenagers has created many different educational methods to improve their level of knowledge and this study showed that using peer based trainings could be helpful in this regard.
Peer education in schools could raise the level of knowledge among female students to an acceptable level and enhance their approach toward these changes. The effect of this method on the knowledge of teenagers about sexual health has been confirmed through Ferrara et al. study.[22] Training teenagers through group discussions,[23] lectures, and educational packages[24,25] has also proved its effect on the knowledge and approach of teenagers; but using these educational methods needs official and semi-official educational programs and preset programs. But unlike those methods, peer education is an unofficial method and depends on communications occurring in natural contexts.
Peer education has also showed its effect on enhancing health information in other social and age groups.[26] Lessons about physical changes during puberty would be learned well through these communications and peer education has been able to attract them to learn these concepts and had a positive effect on their approach.
Teenagers are really sensitive toward changes in their appearance during puberty and with onset of puberty they would experience stress and negative feelings such as fear, tension, shame, and embarrassment. Increased awareness about these changes for teenagers is very important. Many of teenagers would experience fear, tension, and concern when facing these changes; they have a wrong impression about puberty.[27] If they would know that these changes are natural and transient, they would have a more appropriate attitude toward them.[28]
Although this study showed that using the natural context of teenagers’ communications in schools could affect the level of knowledge among teenagers and cause them to find an appropriate approach toward sexual health; but official peer education could have different results.
In a structured training, the audience expects the lecturer to have approved academic qualifications; but in an unstructured and completely unofficial communication teenagers would enjoy their own discussions and would be able to pass on health messages.
To provide sexual health, besides teenagers’ need to have efficient awareness about puberty based changes, it is necessary for them to have enough knowledge about healthy sexual behaviors and motivation to apply them. While many studies show that dysfunctional and unstructured interactions between teenagers would lead to risky sexual behaviors,[5,29,30,31] this study revealed that organizing these interactions through peer education could enhance the knowledge and motivation of teenagers about healthy sexual behaviors.
Emerging and increasing sexual emotions during adolescence[1] would attract teenagers to talk about and discuss this matter. Wrong lessons from some teenagers, which could have been collected from various ways, could pass on through these interactions and they could shape a positive form through organized peer education. Although this study has not evaluated the effect of this method on reducing negative interactions, but revealed that this method could enhance the knowledge and attitude of teenagers which could lead to reduce risky sexual behaviors.
But sufficient knowledge and positive attitude toward healthy sexual behaviors could not reduce risky sexual behaviors just by itself. While having enough knowledge about risky sexual behaviors, previous studies have reported not using condoms among male teenagers.[32,33] A study conducted in New Jersey showed that peer education has not lead to commitment in sexual relationships.[34] Commitment in sexual relations is an important matter in sexual health; but considering the cultural context of the study environment sexual relations among unmarried female teenagers would not usually be reported. Therefore, participants’ commitment was not evaluated in this study and was one of the limitations of this study.
Anyhow, the effect of peer education on increasing the knowledge about risky sexual behaviors among high school student of Nigerian villages has been reported before.[35] Ross et al. reported that peer education would lead to reduced unwanted pregnancies and abortion among students.[36] Besides, the results of a systemic study revealed the effect of peer education on knowledge and awareness and changes in behaviors toward HIV infection and sexually transmitted diseases.[14]
Another result of this study showed that peer education would increase the awareness and lead to positive attitude toward mental and social changes during adolescence. In this period of time, teenagers would face dramatic changes that transform their social interactions. These changes are the way toward having an independent identity that might sometimes challenge teenagers. More desire to be isolated and alone, being indifferent, not having enough concentration, and being stressed and aggressive could challenge teenagers’ relation with their parents and could be considered as disorder by the teenager.
Mental desire to have sexual relations with other sex among female teenagers in a society that do not approve this kind of relations could have a negative effect on their mental health and make them feel guilty. If teenagers would learn that these desires are completely normal, they would deal with them more appropriately. The experiences of these mental desires would be shared among teenagers in different ways; this study showed that organizing these interactions through peer education could enhance positive attitude toward these changes among female teenagers.
It is believed that the need for empathy and being confirmed by peers is the root of many criminal acts among teenagers.[31,37] Especially among female teenagers being rejected by peers could lead to behavioral disorders.[38] Having knowledge about these mental changes could prepare the ground for gaining necessary skills for dealing with the tension caused by mental and social changes and reducing the stress caused by feeling rejected by peers.[31] Taghdisi et al. showed that peer education would increase the knowledge of female teenagers about sexual health matters, which would coordinate their puberty changes with their living environment and reduce their stress.[39]
Although the present has shown that peer education in schools would enhance the knowledge and attitude of teenagers toward sexual health matters, but not evaluating participants’ behaviors and skills in applying these lessons and transmitted messages through this method is one of this study's limitations.
CONCLUSIONS
This study showed that benefiting from natural opportunities that happen in schools, even if they are small, would increase the knowledge of teenagers about sexual health and could enhance their attitude toward different aspects of sexual health.
Financial support and sponsorship
Support Isfahan University of Medical Sciences (Grant Number: 392307).
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
The authors thank the Isfahan University of Medical Sciences for funding the survey (Grant no. 392307).
REFERENCES
- 1.Dahl RE, Gunnar MR. Heightened stress responsiveness and emotional reactivity during pubertal maturation: Implications for psychopathology. Dev Psychopathol. 2009;21:1–6. doi: 10.1017/S0954579409000017. [DOI] [PubMed] [Google Scholar]
- 2.Refaei Shirpak K, Eftekhar Ardebili H, Mohammad K, Chinichian M, Ramezankhani A, Fotouhi A. Developing and testing a sex education program for the female clients of health centers in Iran. Sex Educ. 2007;7:333–49. [Google Scholar]
- 3.Garmaroudi GH, Makarem J, Alavi SS, Abbasi Z. Health related risk behaviors among high school students in Tehran, Iran. Payesh. 2010;9:13–9. [Google Scholar]
- 4.Smeltzer SC, Bare BG, Hinkle JL, Cheever KH. Philadelphia: Lippincott Williams and Wilkins; 2008. Brunner and Suddarth's textbook of medical-surgical nursing; p. 1402. [Google Scholar]
- 5.Olfati F, Aligholi S. A study on educational needs of teenage girls regarding the reproductive health and determination of proper strategies in achieving the target goals in Qazvin. J Qazvin Univ Med Sci. 2008;12:76–82. [Google Scholar]
- 6.Benner MT, Townsend J, Kaloi W, Htwe K, Naranichakul N, Hunnangkul S, et al. Reproductive health and quality of life of young Burmese refugees in Thailand. Confl Health. 2010;4:5. doi: 10.1186/1752-1505-4-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Golbasi Z, Taskin L. Evaluation of school-based n reproductive health education program for adolescent girls. Int J Adolsec Med Health. 2009;21:395–404. doi: 10.1515/ijamh.2009.21.3.395. [DOI] [PubMed] [Google Scholar]
- 8.Moronkola OA, Ojediran MM, Amosu A. Reproductive health knowledge, beliefs and determinants of contraceptives use among women attending family planning clinics in Ibadan, Nigeria. Afr Health Sci. 2006;6:155–9. doi: 10.5555/afhs.2006.6.3.155. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.New York: UNFPA; 1994. International Conference on Population and Development. Programme of Action of the International Conference on Population and Development. [Google Scholar]
- 10.Turnbull T, Van Wersch A, Van Schalk P. A review of parental involvementin sex education: The role for effective communication in British families. Health Educ J. 2008;67:182–95. [Google Scholar]
- 11.Malek A, Abbasi Shokoohi H, Faghihi A, Bina M, Shafiee Kandjani A. A study on the sources of sexu knowledge acquisition among high school students in Northwest of Iran. Arch Iran Med. 2010;13:53742. [PubMed] [Google Scholar]
- 12.Kamalikhah T, Rahmati Najarkolaei F, Karimi M. Barriers of Reproductive Health Education in Schools, Zahedan. J Res Med Sci. 2012;14:71–5. [Google Scholar]
- 13.UNFPA. Adolescent and youth. [Last accessed on 2014 Sep]. Retrieved from Available from: http://www.unfpa.org/adolescents and youth/.2008 .
- 14.Medley A, Kennedy C, O’Reilly K, Sweat M. Effectiveness of Peer Education Interventions for HIV Prevention in Developing Countries: A Systematic Review and Meta-Analysis. AIDS Educ Prev. 2009;21:181–206. doi: 10.1521/aeap.2009.21.3.181. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Layzer C, Rosapep L, Barr S. Peer Education Program: Delivering Highly Reliable Sexual Health Promotion Messages in School. J Adol Health. 2014;54:70–7. doi: 10.1016/j.jadohealth.2013.12.023. [DOI] [PubMed] [Google Scholar]
- 16.Jodati AR, Nourabadi GR, Hassanzadeh S, Dastgiri S, Sedaghat K. Impact of education in promoting the knowledge of and attitude to HIV/AIDS prevention: A trial on 17,000 Iranian students. Int J STD AIDS. 2007;18:407–9. doi: 10.1258/095646207781024829. [DOI] [PubMed] [Google Scholar]
- 17.Miller AN, Mutungi M, Facchini E, Barasa B, Ondieki W, Warria C. An outcome assessment of an ABC-based HIV peer education intervention among Kenyan university students. J Health Commun. 2008;13:345–56. doi: 10.1080/10810730802063470. [DOI] [PubMed] [Google Scholar]
- 18.Salama H, Elsebai N, Abdelfatah F, Shoma A, Elshamy K. Effects of peer education on the knowledge of breast cancer and practice of breast self-examination among Mansoura University Female Students. J Am Sci. 2013;9:253–61. [Google Scholar]
- 19.Gokengin D, Yamazhan T, Ozkaya D, Aytuğ S, Ertem E, Arda B, et al. Sexual knowledge, attitudes, and risk behaviors of students in Turkey. J Sch Health. 2003;73:258–63. doi: 10.1111/j.1746-1561.2003.tb06575.x. [DOI] [PubMed] [Google Scholar]
- 20.Abbaspour1 Z, Saidian M, Abedi P. Peer Education vs Health provider Education in knowledge and Attitude about prevention and transmission of AIDS in High School Student. Med Sci. 2007;23:108–10. [Google Scholar]
- 21.Van der Maas F, Otte WM. Evaluation of HIV/AIDS secondary school peer education in rural Nigeria. Oxford Univ Press. 2009;24:547–57. doi: 10.1093/her/cyn056. [DOI] [PubMed] [Google Scholar]
- 22.Ferrara M, Langiano E, De Vito E. A school based community randomized trial of the effect of peer health education on primary prevention knowledge, attitude and behaviors towards HPV among adolescents Italian. IJPH. 2012;9:20–32. [Google Scholar]
- 23.Shirazi M, Anoosheh M, Rajab A. The effect of self-care program education through group discussion method on knowledge and practice in diabetic adolescent girls referring to Iranian Diabetes Society. Iranian Journal of Medical Education. 2011;10:982–93. [Google Scholar]
- 24.Khakbazan Z, Jamshidi F, Mehran A, Damghanian M. Effects of lecture presentation and presenting educational packages on girls’ knowledge about adolescence health. Journal of Hayat. 2008;14:41–8. [Google Scholar]
- 25.Majlessi F, Mahmoudi M, Rahimi, Hosseinzadeh P. The impact of lecture and educational package methods in knowledge and attitude of teenage girls on puberty health. J Hormozgan Med Sci. 2011;15:327–32. [Google Scholar]
- 26.Noori Sistani M, Merghati Khoi E, Taghdisi MH. Promoting Knowledge, Attitude and Practices (KAP) of the mothers in their girls pubertal health based on peer education approach. J Babol Univ Med Sci. 2010;11:33–9. [Google Scholar]
- 27.Houston AM, Abraham A, Huang Z, D’Angelo LJ. Knowledge, attitudes, and consequences of menstrual health in urban adolescent females. J Pedi Adoles Gyneco. 2006;19:271–5. doi: 10.1016/j.jpag.2006.05.002. [DOI] [PubMed] [Google Scholar]
- 28.Moodi M, ZamaniPour N, SharifZadeh G, Akbari-Bourang M, Salehi S. Evaluating Puberty health program effect on knowledge increase among female intermediate and high school students in Birjand. J Birjand Uni Med Sci. 2006;13:36–42. [Google Scholar]
- 29.Ali TS, Rizvi SN. Menstrual knowledge and practices of female adolescents in urban Karachi, Pakistan. J Adol. 2010;33:531–41. doi: 10.1016/j.adolescence.2009.05.013. [DOI] [PubMed] [Google Scholar]
- 30.World Health Organization. [Last accessed on 2012 Sep 15]. Available from: http://www.who.int/
- 31.Parvizi S, Ahmadi F. Peer group and adolescent health: A qualitative study. Feiz J. 2006;10:46–52. [Google Scholar]
- 32.Mellanby AR, Newcombe RG, Rees J, Tripp JH. Comparative study peer–led and Adult–led school sex education. Health Educ Res. 2001;16:481–9. doi: 10.1093/her/16.4.481. [DOI] [PubMed] [Google Scholar]
- 33.Piero B, Chiara M, Patrizia S, Carlo AP. Is peer education the best approach for HIV prevention in schools?. Findings from a randomized controlled trial. Adol Health. 2005;36:508–16. doi: 10.1016/j.jadohealth.2004.03.005. [DOI] [PubMed] [Google Scholar]
- 34.Mahat G, Scoloveno M, Leon T, Frenkel J. Preliminary Evidence of an Adolescent HIV/AIDS Peer Education Program. J Pedia Nurs. 2008;23:358–63. doi: 10.1016/j.pedn.2007.12.007. [DOI] [PubMed] [Google Scholar]
- 35.Maas F, Otte WM. Evaluation of HIV/AIDS secondary school peer education in rural Nigeria. Health Educ Res. 2009;24:547–57. doi: 10.1093/her/cyn056. [DOI] [PubMed] [Google Scholar]
- 36.Ross DA. Approaches to sex education: Peer-Led or Teacher-Led? PLoS Med. 2008;5:229. doi: 10.1371/journal.pmed.0050229. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.RezaeiAbhari F, Hamzehgardeshi Z, Hajikhani Golchin N, Zabihei M. Drug user girls’ perceptions of their sexual decision making: Qualitative research. Nurs Res J. 2009;6:78–87. [Google Scholar]
- 38.Anisi J, Salimi H, Mirzamani M, Reisi F, Niknam M. A survey study on Behavioral problems in adolescence. Behavi Sci J. 2007;1:164–70. [Google Scholar]
- 39.Taghdisi MH, Noori Sistani M, Merghati Khoi E, Hoseini F, Asgharnejad Farid AA. Impact peer education approach on knowledge and practice about mental health of adolescent girls. TB. 2012;10:92–105. [Google Scholar]